Download to read offline

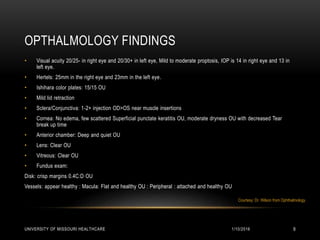
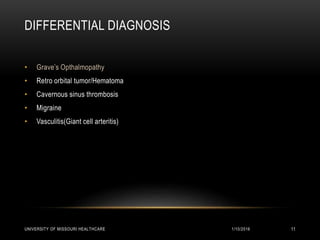

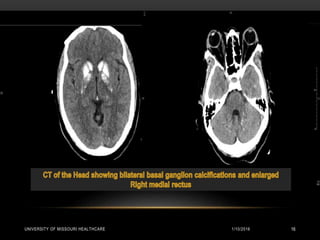
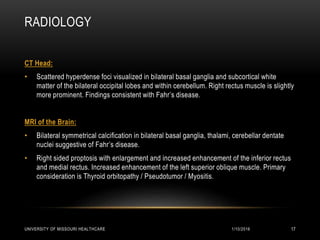
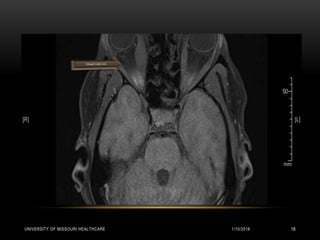
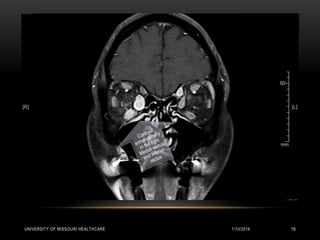
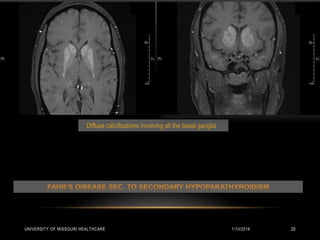
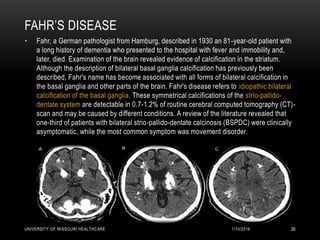

This patient presented with new onset right-sided headache, eye redness, and double vision when looking to the right. Physical exam revealed proptosis and injection of both eyes, with greater involvement on the right side. Imaging showed diffuse calcifications in the basal ganglia consistent with Fahr's disease, as well as enlargement and enhancement of the right extraocular muscles, concerning for thyroid orbitopathy. The differential diagnosis included Graves' ophthalmopathy, retroorbital tumor/hematoma, cavernous sinus thrombosis, and migraine. Management focused on treating the thyroid orbitopathy while further evaluating the neurological condition of Fahr's disease.



































































