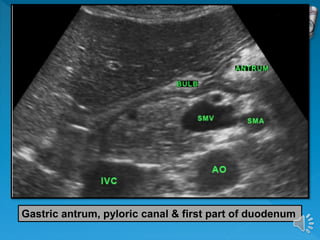
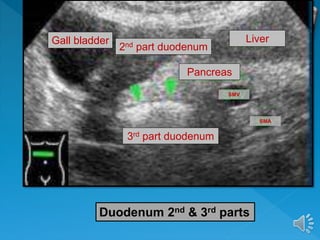
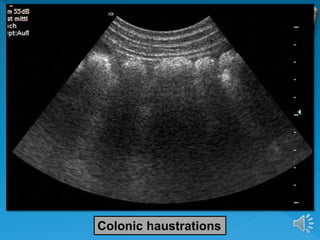
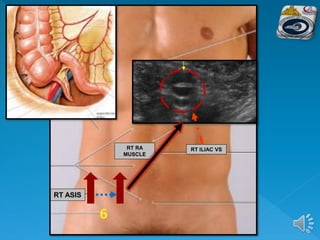
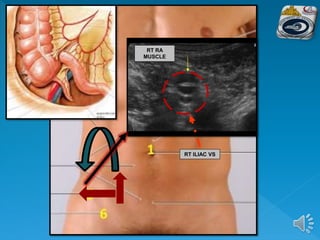
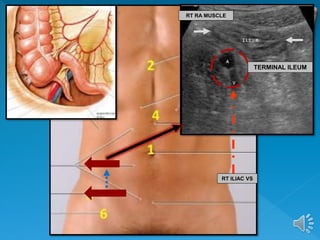
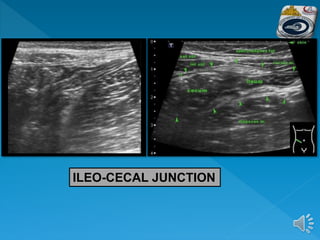
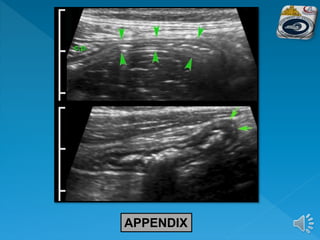
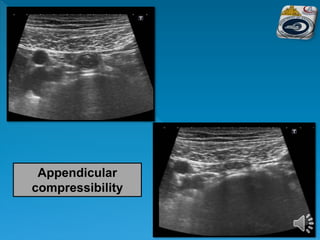
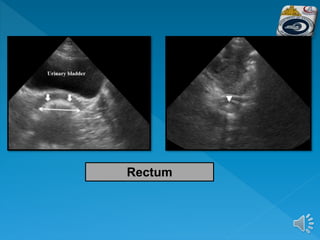
The document describes the normal ultrasound appearance and technique for scanning the gastrointestinal tract. Key areas that can be visualized include the gastroesophageal junction, gastric antrum, duodenum, ileocecal region, ascending and descending colon, rectum, and lower sigmoid colon. The normal wall layers of the bowel are described as well as measurements for bowel diameter and wall thickness in different regions. Dynamic assessment of peristalsis and compressibility are also discussed.