GINGIVITIS
• Is inflammationof the gums
Types
• Marginal gingivitis
• Ulcerative gingivitis
• General gingivitis
3.
Marginal gingivitis
Etiology
• Lackof sufficient mastication
• Lack of cleanliness of gums
• Use of hard toothbrushes
• Use of hard toothpicks
4.
Clinical presentation
• Bleedingof the gum
• Soreness of gums especially on brushing
• Gums appear red and swollen
• Pus may be squeezed out of margin of the gum
5.
Treatment
• Advice onsoft toothbrush use
• Remove tatters of food debris gently
• Advice on good hygiene at least twice daily
• Give antibiotics if there is sign of infection
• Give analgesic in case of pain preferably an anti-
inflammatory analgesic eg brufen
6.
GENERAL GINGIVITIS
• Involvesthe whole gum i.e. all gum is inflamed
Etiology
• Lack of vitamin c
• Ingestion of substance like mercury and lead
• Ill fitting dentures
• Some drugs eg phenytoin sodium( epileptic)
7.
Treatment
• Give vitC about 200mg TDS for 1 month
• Hygiene
• Stop drugs us eg phenytoin sodium
• Give analgesics incase of pain especially anti-
inflammatory
• Advice on use of fresh fruits an use of proper fitting
dentures and antibiotics incase of infections
8.
ULCERATIVE GINGIVITIS
• Associatedwith ulceration of gums
Etiology
• Bacillus pisiform
• Treponema pallidum
• Other pyogenic microorganisms
Treatment
• Give antibioticseg septrin 960mg BD plus flagyl
400mg TDS for 3 days
• General oral care by use of hydrogen peroxide
( diluted)
• Betadine solution ( those who are able) as an
antifungal analgesic, antibiotic antiviral
• In absence of above use normal saline and this is
common
Simple stomatitis
• Itis due to local causes effecting the mucous
membrane of the mouth eg hot tea, hot porridge ,
smoking and drugs
15.
Clinical features
• Excessivesalivation
• Bad taste
• Heat sensation in the mouth
• Furred tongue
• Pain during mastication
• On exam, we have bad breath and there are ulcers
on floor, roof or cheeks of the mouth
16.
Aptuous stomatitis
Etiology areunknown but there are associated
factors
• Debilitating diseases or conditions
• Nervous tension ( emotional trauma)
• GI disturbance as a result of GI diseases eg ca
stomach, ca esophagus, peptic ulcer disease and
liver diseases
17.
Clinical features
• Painin mouth especially on chewing
• There are small round red areas that rapidly
ulcerate and are common in cheeks under the
tongue or gums. They keep recurring
18.
Ulcerative stomatitis( Vincent
Angina)
•Common in pts with low immunity
• It therefore is associated with the following conditions
• HIV
• Malnutrition
• Tb
• Diabetes mellitus
• Malignant disorders
• Long term use of cytotoxic drugs
• Measles in children
• Long term use of steroids
• Blood associated disorders eg leukemia, agranulocytosis
19.
Clinical features
• Pyrexia
•Cheeks are painful
• Tenderness on both cheeks and tongue
• Cheek may appear swollen and ulcerative
20.
Parasitic stomatitis
Etiology- candidaalbican ( oral candidiasis)
• It is the commonest type of stomatitis encountered
especially in children
• it also affects adult in case of low immunity
secondary to debilitating diseases or any other cause
of low immunity
• However oral thrush also occur in children on
prolonged use of broad antibiotics
• It is also common in pregnancy ( increase in steroids)
21.
Clinical presentation
• Infants,children and adults with debilitating illness
• Pain especially on biting food or putting food on
mouth or mastication
• On physical exam, whitish patch on mouth, cheek,
tongue, pharynx, gums and may spread to all of GI
• N/B: the whole of GI may be affected and the pt may
present with continuous epigastric pain and the
inability to swallow( pain on swallowing )
• Those who are unable to swallow may have
esophageal candidiasis
22.
Gangrenous stomatitis
• Etiology-treponema pallidum, fusiperm bacillum
• It is common in children and adults with debilitating
illness
23.
Presentation
• Pain inmouth
• Ulcer in inner mouth which may spread to
perforate the cheek
• Edema of face, gums and jaw
• They may have fever
• May complicate to septicemia
• For children it may complicate to bronchial
pneumonia
24.
Vesicular stomatitis
• Dueto virus mainly due to herpes simplex
• Herpes labialis may also affect the whole GI
especially in immuno-suppressed pts
• It is common in immuno-suppressed pts and it
presents with epigastric pain and dysphagia
25.
Clinical features
• Eruptionswhich are vesicular or pustules and may
be limited to the cleft palate
• May invade the tongue , however in most cases
they are found on lips of mouth
• Pts present also with general malaise and severe
pain on vesicle or pasture
26.
Treatment of stomatitis
•Analgesics and antipyretic in case of pain and fever i.e
brufen and dichlorophenol
• Incase of infection give antibiotics eg gangrenous
stomatitis , penicillin and flaggyl
• Lesion with pus take pus for culture and sensitivity to
guide on type of antibiotics to use
• Advice on general oral hygiene eg against smoking, eating
hot food and fruits
• Investigate and treat underlying condition eg incase of
cytotoxic drugs stop using them, incase of steroids stop
use, incase of Tb treat
27.
• Wash themouth with hydrogen peroxide or bentadine solution
or normal saline. Hydrogen peroxide should be diluted in ration
0f 1:5)
• Apply glycerine or boric acid incase of simple stomatitis due to
local causes. In the absence you can apply G.V paint
• In case of oral thrush apply nystatin oral drops, actarin , oral jelly
or clotrimazole mouth paint or candida mouth paint
• Advice on soft diet and use vitamin containing food
• Advice against eating hot food or taking hot drinks
• Observe oral hygiene
• N/B: treatment is symptomatic with removal of underlying cause
Acute Glossitis
Etiology
• Abrasionsand bruises secondary to trauma which
may be as a result of self bite , dental carries etc
• Insect bites eg bees
• Burns
• Chemical irritants and toxins
• Incase of an infection it is due to streptococcus
31.
Clinical features
• Painin tongue which radiate to ear
• Swelling of the tongue
• Fever
• On exam, the tongue is red and swollen
• The lymph nodes may be enlarged especially
sublingual and submandibular
32.
Course
• The diseaserapidly progresses and forms an
abscess
• If no immediate intervention is put in place,
gangrene forms on the tongue
33.
Complications
• Edema ofthe larynx
• Ludwig's angina- inflammation of the tongue of the
mouth
• Septicemia
34.
Treatment
• Analgesics areimportant eg diclofenac , brufen
• Oral hygiene
• Apply cold ice on the tongue, this also reduces
inflammation and hence the pain
• Give antihistamine to reduce the edema eg piriton
or in severe cases give steroids to reduce
inflammation hence edema
• In case of suspicion of infection give antibiotics
preferably ampiclox 500mg QID for 5 days
35.
Chronic inflammation
• Resultsfrom irritants due to:
• Smoking
• Alcohol intake
• Ill fitting dentures
• Conditions like syphilis or any other forms of chronic oral
sepsis
• Vit deficiency and iron defficiency
36.
Clinical features
• Hxof soreness of tongue with pain
• On exam you see areas of smooth patch on the
tongue
37.
Treatment
• Oral hygiene
•Avoid all irritating food and substances
• Stop smoking and alcohol
• Give multivit tablets and ferrous sulphate incase of
nutritional glossitis
• Incase of syphilis treat syphilis with penicillin 2.4 MU
every one week in 3 doses (benzathine pen I.M or
2.4MU stat followed by erythromycin 500mg QID for 1
week
• Giving antibiotics eg ampiclox 500mg QID for 3 days
38.
Differentials
• Simple ulcersdue to trauma
• Tuberculosis ulcers
• Granulomatous ulceration due to Tb or syphilis
• Oral thrush ( severe)
Causes
• Drugs egpotassium iodide( treatment)
• Oral/dental sepsis
• Oral thrush
• Mumps
• Ca esophagus
• Ca stomach
• Gastric ulcers
• Nervous lesion eg encephalitis
• Physiological trauma
• Dysphagia
• Hormonal imbalance eg pregnancy
• Fractures of jaw due to irritation of nerve which stimulate saliva production
42.
Treatment
• Is directedto specific cause with investigation
• Incase of a nervous lesion give atropine 0.3mg stat
and then continue with antihistamine
• If the pt. is depressed give antidepressants eg
amitriptyline
Causes
• Dehydration egDKA
• Febrile illness eg malaria
• Atrophy of salivary glands
• Obstruction of salivary glands eg tumors which compress
ducts
• Reduced fluid intake
• Nervous lesions or emotional state
• Hormonal imbalance
• Drugs like opium
• Chronic inflammation of salivary glands
46.
Treatment
• Treatment isdirected to the cause
• If psychological give counselling
• If due to drugs stop them
• If due to dehydration rehydrate the pts
Acute sepsis parotitis
•It is the infection( inflammation of parotid) of the
parotid gland which usually descends through the
parotid duct
• The parotid gland accounts for about 60% of saliva
in the mouth
49.
Etiology
• Staph aureus( commonest), strep viridians, strep
pneumoniae
• The infection is common in absent of mastication
• It also occurs on typhoid fever through
hematogenous spread
• it is more common in comatose pts, fractures jaw
and stomatitis
50.
Presentation
• Pain orswelling in one of the parotid glands
• Dysphagia
• General malaise
• On exam , parotid gland is enlarged and tender, skin
over it is red , there maybe signs of suppuration
( pus formation)
• Local temperature is raised
51.
Treatment
• Give antibiotics, broad spectrum, ampiclox 500mg
QID for 1 week, amoxycillin or cloxacillin in absent of
ampiclox
• Incase of pus, pus swab for culture and sensitivity
will guide on choice of antibiotics
• If an abscess is present incise and drain it
• Analgesics for pain , diclofenac 100mg BD or 50 mg
TDS for 3 days or until pain subsides
• Observe oral hygiene with oral mouth washing using
normal saline, betadine or hydrogen peroxide
Dysphagia
• Is difficultin swallowing or sensation of sticking or
obstruction in passage of food from the upper to
the lower GI i.e. passage of food through mouth,
pharynx and esophagus
57.
Terms associated withdysphagia
• Aphagia- inability to swallow
• Odynophagia – painful swallowing
• Pagophagia – fear of swallowing
58.
Physiology of swallowing
•Normal transport of an ingested bolus through the
swallowing pathway depends on
a) Size of ingested bolus
b) Luminal size of esophagus pharyngeal opening
c) Peristaltic contraction. These are also affected by
nervous and muscle injury( peristaltic)
d) Degglutitive inhibition which is associated with normal
relaxation of lower and upper sphincter during
swallowing
Mechanical dysphagia
• Largebolus of food
• Intrinsic narrowing of esophagus like in stricture which could
be congenital or acquired. The narrowing could also result
from inflammation or tumour eg ca esophagus
• Extrinsic compression resulting from cervical spondylitis
which cause prolapse of cervical disc leading to compression
• Enlarged thyroid gland
• Vascular compression eg aneurysm
• Retropharyngeal abscess or masses
• Zenkers diverticulum /esophageal diverticulum
61.
Motor/ neuromuscular dysphagia
•Difficult in initiating reflex as a result of oral lesion or tongue
paralysis
• Sjogren’s syndrome
• Dry mouth caused by wasting of salivary gland
• Vagus and glossopharyngeal nerve paralysis
• Lesions of swallowing center
• Disorders of oropharyngeal and esopharyngeal striated
muscles eg incase of muscle weakness as it is in lower motor
neuron lesion
• Other disorders eg myopathy ( abnormal overgrowth of
muscle may lead to dysphagia)
62.
• Rabies ortetanus- may impair with degglution as a
result of constant spasm of muscles and poor
relaxation to allow swallowing
• Disorders of esophageal smooth muscles- there may
be paralysis of esophageal body or interference in
neuromuscular transmission or decreased muscle of
esophagus so that the coordinated swallowing is
impaired. Food reaches the area but there is failure
of relaxation of cardiac sphincter leading to
accumulation of food at that level ( achalasia cardia)
63.
Investigations
• Testing forcranial nerve ( x, ix)
• Ct scan to rule out space occupying lesions
• Chest Xray to rule out tumors that are adjacent to
the passage
• A barium swallow to rule out cancer of esophagus
• Cervical x-ray to rule out prolapse of cervical disc
• MRI
Acute esophagitis
Causes
• Chemicalirritations like poison and other corrosive
substances like spices
• Impacted foreign body eg bones( fish bones)
• Infections eg candidiasis, syphilis , herpes
• Neoplasms eg ca esophagus
• Repeated vomiting
• Sliding hiatus hernia- this displaces the curving of
esophagus and allows reflux of food. It is an opening
/herniation of fundus into the diaphragm. In this case the
stomach passes partly or completely into the chest cavity
through the hole( weakness of esophagus)
68.
Clinical features
• Therewill be a hx of causative condition
• Pain on swallowing ( retrosternal pain)
• Vomiting blood and mucus
• General malaise( body weakness)
69.
Complication
• Ulceration causingstenosis of esophagus as a result
of healing by scarring and fibrosis
• Submucous abscess formation causing mediastinitis
• Perforation of esophagus
70.
Treatment
• Analgesics egmorphine and pethidine in case of pain
i.e 10-15 mg of morphine PRN . Pethidine about 50mg
PRN. However if the pain is not severe you can give
Panadol or diclofenac
• Beta blockers- H2 antagonists eg cimetidine ( Tagamet)
or Ranitidine ( zantal). Cimetidine 400mg BD for 1
week and ranitidine 150mg BD or 300mg OD for 1
week
• In the absences of h2 antagonist or if the esophagus is
not severe we give antacid. Misled antacid 20mls TDS
for 1 week or until pain subsides
71.
• Use ofsoft or blended diet
• Avoid spiced food or food suspicious of poisoning
• Incase of infections like abscess formation give
antibiotics eg amoxyl , erythromycin, ampiclox
• Finally treat and remove underlying cause
Clinical features
• Signsand symptoms suggestive of the cause
• Burning sensation retrosternal
• Repeated small hematemesis
74.
Treatment
• Use ofsoft and bland diet
• Antacid
• H2 antagonist cimetidine 400mg BD or ranitidine
300 mg OD for 4 weeks
• Treat or remove the underlying cause
Achalasia cardia
• Thereis obstruction in the lower end of esophagus
due to failure of relaxation of cardiac sphincter on
deglutition
• This is as a result of unknown cause but
disturbances of the neuromuscular mechanism is
considered as the etiological factor
• Some physiological elements have been considered
with it eg emotions
77.
Clinical features
• Occurscommonly in adults above 20 years of either sex
• There is discomfort on swallowing
• There is regurgitation of food
• The patient feels obstruction in the esophagus
• Pt prefers eating while standing ( gravity)
• Dysphagia begins with fluid rather than solids
• There is chocking sensation and substernal pain which
occurs during or after swallowing
• Vomiting may occur even during sleep
78.
• Pts mayalso experience pressure symptoms eg
dyspnea, palpitations, pain radiating to shoulders
etc
• Wasting occurs only if it is chronic unlike in ca
esophagus
79.
Investigations
• Barium swallowwhich shows: dilated esophagus above an
obstruction at the level of diaphragm, in some cases there
may be some fluid behind the cardiac shadow, there is
absence of gaseous shadow in fundus of stomach which is
usually there in normal cases
• Ct scan to rule out an SOL which may interfere with normal
neuromuscular function
• Esophagoscopy- this rules out tumour eg ca esophagus, it
may also rule out esophagitis or presence of a foreign body
in the esophagus. It is done when pt is under G.A. a biopsy
can be taken or a foreign body removed. It is not diagnostic
but helps to rule out other conditions
80.
Differentials
• Ca esophagus
•Aneurysm ( bruits)- distortion on barium swallow
• Hiatus hernia
• Esophagitis
• Esophageal strictures ( pain may be not be severe
on swallowing solids)
81.
Treatment
• Surgical dilationof cardiac sphincter
• Cardio-myotomy – surgical operation involving
removal of some parts of cardiac sphincter
Types of cardio-myotomy
• Hiller’s operation
• Ramstad's operation
Complications
• Chronic esophagitis
•Formation of diverticulum
• Hemorrhage with rupture of esophagus
• Wasting especially in chronic case
• Dysphagia
• Aspiration pneumonia
Predisposing factors
• Alcoholabuse
• Smoking approximately 20 stick per day
• Esophageal stricture secondary to any cause
• Irradiation as a result of treatment of malignancy of
chest
• Chronic ingestion of hot food
• Plummer Vinson syndrome
• Achalasia cardia as a result of food reflux
• Esophagitis
87.
N/B
• Plummer Vinsonsyndrome is a degeneration and
atrophy of epithelium of tongue, pharynx,
esophagus and stomach due to iron deficiency
Sites of caesophagus
• Commonest is mid 1/3 and it accounts for 60%
• Upper 1/3 is rare and accounts for 10%
• Lower 1/3 is rare and accounts for 30%
91.
Clinical features
• Dysphagiawhich starts with solid then semi-solids then liquid
• Weight loss
• Chest pain( retrosternal in most cases)
• Hoarseness of voice due to irritation to laryngeal nerve adjacent
• On exam, initially there will be nothing significant but there may
be cervical lymphadenopathy, anemia due to hemorrhage,
hematemesis, cachexia as a result of poor feeding and
metastasis to liver, bone and other organs.
• However, there may be other associated features according to
complication eg spread to lungs then there may be cough and
hemoptysis
92.
Investigations
• Barium swallow-this will show rat tail like appearance
( distortion is evidence and takes shape of rat tail)
• Esophagoscopy – one is able to visualize the tumour and you
can take a biopsy .done by surgeons
• In some cases we have esophagogastroscopy to rule out ca
stomach
• Full hemogram plus ESR where Hb drops and ESR increases
• A chest x-ray to rule out metastasis or pneumonia process in
the lungs
• Ultrasound to rule out metastasis in the liver
• Diagnosti- biopsy
Supportive
management( palliative)
• Analgesicif there is pain eg pethidine or morphine
• Transfuse or give hematemics depending on degree
of anemia
• Incase of severe dysphagia NGT for feeding but this
is a specialized form of NGT called cillestine tube. It
is a tube that bypass esophagus and goes to the
stomach
95.
Specific treatment
• Radicalsurgical – resection of esophagus and end
to end anastomosis
• Radiotherapy
• N/B: mgt is mainly palliative cause tumor is in most
cases discovered in its advanced stages where
metastasis has taken place
Acute gastritis
• Isinflammation of mucous membrane of stomach
which could be acute or chronic
• It is a common condition especially in alcoholic
people
100.
Causes
• Ingestion ofirritants eg spices , poisoned foods,
inhalation or swallowing irritant gases
• Uremia- high levels in which the gastric mucosa is
destroyed like incase of renal failure
• Infections eg viruses ( herpes simplex) , fungal
( candidiasis). These are common in HIV pts , other
infections could be bacteria and worms
• Alcohol ingestion – it is one of the most common
cause among heavy alcoholics
• N/B: these are mainly causes of acute gastritis
101.
Clinical presentation
• Hxof predisposing factor/cause
• Hx of sudden epigastric pain with nausea and vomiting-
the vomitus may contain some blood or may be stained
hematemesis
• Diarrhoea
• Temp is decreased but incase of incase of infections it
increases
• If dehydrated then there will be a rapid pulse
• On exam there is tenderness in epigastric region( gastritis
is commonest cause of tenderness in epigastric region)
102.
Differentials
• Peptic ulcerdisease- however PUD is marked by
periodicity
• Acute appendicitis- this is xtised by rebound
tenderness on Rt iliac fossa
• Ca stomach- is a chronic condition associated with
a lot of wasting
Investigations
• Involves carefulhx taking and physical exam which is
important in ruling out other causes of gastritis and
epigastric pain or tenderness
Otherwise the following can be done as lab investigations:
• Stool for ova and cyst
• Stool for culture and sensitivity
• Barium meal to rule out PUD
• Gastroscopy to rule out PUD and ca stomach
• Blood for FHG plus ESR- this rules out infections eg
bacteria , viral
105.
Treatment
• Depends oncause i.e. investigate and treat and remove the cause
• Bed rest
• NGT for feeding
• Rehydrate with iv fluids if dehydrated
• Sucking by NGT i.e gastric lavage
• Incase of corrosive give antacid or H2 antagonist
• Gastric lavage is indicated on organophosphate poisoning, drug
poisoning eg aspirin and chloroquine
• Advice on use of milk and antacid
• In severe cases, give H2 antagonists ( cimetidine or ranitidine
until pain subsides
106.
CHRONIC GASTRITIS
• Followsacute or chronic alcoholism
• It may also be due to peptic ulcer or ca stomach
• Pernicious anemia and blood diseases eg leukemia
• Clinical features vary from dyspepsia to heartburn,
anorexia, nausea especially in the morning and
vomiting mucous like vomitus
• On examination, there is epigastric tenderness
107.
Treatment
• Treat underlyingcause
• Avoid alcohol
• Give antacid and milk ( 2 glasses a day after every
meal)
• Avoid spiced food especially during treatment
Hematemesis
• It isalso called upper GI bleeding
• It is a sign of upper GI bleeding defined as vomiting
of blood
• Sometimes a real red color of blood doesn’t appear
but is seen as altered blood color popularly referred
to as coffee ground material, this may indicate
slight GI bleeding
110.
Causes
• PUD
• Esophagitis
•Gastroesophageal varices
• Gastritis ( from alcohol, drugs etc)
• Mallory Weiss tear/ syndrome- trauma caused by vomiting
• Malignancies eg ca stomach and ca esophagus
• Trauma as incase of NGT insertion or directed external trauma
in abdomen
• Infection: viral ( yellow fever , ebola, rift valley fever)
• Uremia- causes inflammation edema and ulceration on stomach
wall resulting in bleeding
111.
• Swallowed bloodeg bleeding from mouth then
swallowing and vomiting
• Ruptured esophageal aneurysm and varices
• Anticoagulant’s blood eg heparin , warfarin etc
• Blood bleeding disorder eg hemophilia , leukemia
etc
• Hepatic failure
112.
Evaluation of apatient with
hematemesis( approach)
• Take hx- this is important as it will rule out trauma, PUD,
infection, cause of uremia etc, use of drugs eg warfarin
• Physical examination- epigastric tenderness to rule out
gastritis , PUD, features of liver failure cirrhosis, ca stomach,
features of vasculitis, pus on NGT aspirate, blood
• Pass an NGT to be sure of site of bleeding. This is not always
positive as false negative may occur if bleeding has stopped
• Endoscopy – to spot the bleeding site and if possible for
therapeutic intervention eg taking biopsy, diathermy or
lesser therapy. This entails a beam of rays with same energy
that enables to make blood vessels to close
113.
• Sometimes therecan be injection of adrenaline and sclerosants
which may constrict the bleeding vessel or capillary and stop
further bleeding ( maneuver is called sclerotherapy)
• Barium swallow to find out the extend of bleeding- this may
show that the bleeding is arising from esophagus and not the
stomach
• Assess how much blood has been lost. If much blood is lost
then the patient has severe hematemesis. Such a patient may
have symptoms of shock( pallor, low blood pressure , thread
weak pulse , rapid respiratory rate
• N/B: severe hematemesis occurs only in raptured esophageal
varices , bleeding PUD and ca stomach
114.
Treatment : supportive
•Bed rest
• Blood for GXC
• Transfusion if patient has lost a lot of blood or is in
shock
• Meanwhile put up an iv line with iv fluids preferably
plasma expanders to stop or treat shock
• If plasma expanders are not available, give normal
saline coz it is isotonic and doesn’t disappear into
tissues very fast hence can improve blood pressure
• Monitor vital signs, temperature , blood pressure etc
115.
• Pass anNGT incase of severe bleeding to aspirate
the blood
• Give H2 antagonists incase of suspicion of
esophagitis or PUD : ranitidine 400mg BD for 4-6
weeks
• Incase of severe hematemesis, nil by mouth coz the
patient may be needed to be taken to theatre
116.
Specific treatment
• Dependson amount of blood loss
• Surgical intervention may be done in theater i.e
sclerotherapy, diathermy and lesser therapy.
However the treatment will depend on cause of
hematemesis eg
• Ca esophagus- surgical removal
• Ca stomach- surgical removal
• PUD – treatment of PUD preferably with H2 antagonists
PUD
• It’s anacute or benign ulceration occurring in the
portion of digestive tract accessible to gastric secretion
• May occur in the:
• Duodenum
• Gastric
• Esophagus
• Jejunum
• Pyloric channel
• Meckel's diverticulum
• However sites of importance are the duodenum-
duodenal ulcers(DU) and gastric ulcers ( GU)
119.
Etiology
• The realcause is unknown but we have predisposing
/associated factors:
1. Zollinger Ellison syndrome- is a benign growth of mucus
secretory gland ( gastrinoma) which leads to excess HCL
secretion
2. Trauma – can be due to irritant substances like: spiced
food, smoking, alcohol, drugs like aspirin and other anti-
inflammatory drugs, NSAIDS, caffeine eg coffee and tea
and colas
3. Nervous disturbances- this is as a result of overactivity of
vagus nerve resulting in overproduction of HCL . It may
occur coz of stress( physiological or physical)
120.
4. Genetic predisposition-it is said to run in families hence it is
genetically predisposed
5. Associated with blood group O- they are more predisposed to it
6. Helicobacter pylori- it is said that it initiates formation of an ulcer
and it also hinders healing of an ulcer
• It is an infection ( with a bacteria which is a short spiral shaped
microaerophilic gram-ve bacilli. It is associated with virtually all
ulcers not induced by NSAIDS
• H. pylori colonize the T-players of mucosa jelly that coats gastric
mucosa which presumably disrupts its protective properties
• H. pylori is thought to infect virtually all patients with chronic active
gastritis
121.
Pathophysiology of PUD
•Results from imbalance of aggressive factors eg
gastric acid, pepsin and defensive factors involved
in mucosal resistance which includes: gastric
mucous, bicarbonates, microcirculation
prostaglandin
• If the imbalance occurs then mucosal destruction
arises leading to formation of an ulcer i.e. if
environment becomes more acidic, chances of an
ulcer are increased
122.
N/B
• Internationally thefrequency of PUD is decreased
in developed world and increased in developing
world
• Mortality rate is low therefore prognosis is good if
treatment measures are put in place as early as
possible
• Male to female ratio is approximately 2:1
• Age – DU occurs mostly in young adults as
compared to GU which is more common in the old
123.
Clinical findings
1. Hxof epigastric pain associated with food i.e some minutes or
hours after food. Vomiting relieves the pain especially in
duodenum ulcers. The pain wakes up pts commonly at 2-3 am
and it wakes the pts to take food.
2. Persistence vomiting in ulcers usually indicates gastric outflow
obstruction which could be due to spasmodic or organic
narrowing
3. Hematemesis shows a bleeding ulcer
4. Pointing sign- pts localizes the pain ie epigastrium for GU and
slightly on the right side of epigastrium for DU. DU pain is also
referred to as hunger pain. Pain occurs less frequently at 1st
in
one episode or 2 episodes for days in a year but latter becomes
frequent as the ulcer progresses.
124.
• However suddensevere pain ( sudden acute pain)
may indicate perforation of duodenum
5. Other features are: nausea, anorexia, feeling
discomfort or distension at epigastrium, heart
burn, water brush
N/B: sometimes the vomiting can be copious and
often relieves pain in gastric ulcers
125.
On exam
• Thept is ill looking and appears pale usually middle
age
• Well nourished in case of DU or wasted incase of GU
• Per abdomen , there is epigastric tenderness
corresponding to the site of pain
• Succussion splash may be present especially if there is
an obstruction of gastric outflow
• Sometimes the epigastric tenderness may be absent eg
obese, mild ulcer, early stages, with drugs eg antacid
126.
Essentials of diagnosis
•Epigastric pain
• Pointing sign and localizing epigastric tenderness
• Periodic behavior with food
127.
Differential diagnosis
• Gastritis-there is a short hx which most of the time the
associated factor or causative factor can be identified eg alcohol
• Ca stomach- associated with wasting which is common in
elderly people
• Esophagitis – there is retrosternal pain on swallowing
• Cholecystitis- pain is more on the right hypochondrium an
muffis sign is positive
• Upper intestinal obstruction- there will be projectile vomiting
and abdominal bowel sounds may be increased
• Acute appendicitis- pain is more in RT iliac fossa. Usually
localized, however it may extend from umbilicus to iliac fossa
128.
• Pancreatitis –there will be mild jaundice and pain which
will be more on left epigastrium. There may be
associated or predisposing factor in hx eg alcohol
• Hookworm infestation- leading to duodenitis. There will
be hx of worms in stool. Pts may be anemia. Not
associated with food periodicity
• Opportunistic infections- eg herpes and candidiasis.
Especially in ISS. There will be a hx of physical sign
pointing at iss and may be other features associated with
local condition eg oral thrush for candidiasis
• Melaena
Investigations
a. Stool foroccult- is positive for upper GI bleeding and
is useful but not indicate that patient has PUD
b. Stool for ova and cyst- to rule out worm infestation
c. Barium meal- in this case one will visualize a crater in
GU i.e. there will be a small collection of barium in
mucosal fold radiating to the area of the ulcer. In
duodenal ulcer there will be duodenal cave deformity.
Barium meal is good for dx of PUD however one can
miss a small ulcer
d. Endoscopy- provide direct visualization of ulcer for
both GU and DU. It is good for even small ulcers
131.
e. Full hemogram-decreased Hb and increased ESR
f. Helicobacter pylori test- is only isolated on biopsy
exam. Stool for C/S or direct microscopy in search
for H. pylori is not patinent (informative)
• As H. pylori contain enzyme urease and dx can only
be by capture of mucosal biopsy in urea containing
Broth or by IZC-urea breath test or Enzyme
immunosorbent assay( ELISA) for H. pylori
immunoglobulin
132.
MANAGEMENT
Medical Mgt
1. GENERALMEASURES
Aims of mgt
• Reduce acid secretion
• Relieve pain
• Promote healing
Mgt
a. Advice patients to have rest, this will help in
allaying anxiety and relieving stress
133.
b. Give psychotherapy:
•Make her understand her condition
• It is recurrent
• To finish medication
• The problem may heal or it may not heal
• It is a chronic condition
• If there is any stress talk to her
c. Advice to stop alcohol and cigarette smoking. Cigarette
smoking is associated with poor healing. Alcohol leads to
more injury to mucosa
d. Avoid drugs that can initiate or irritate gastric and
duodenal mucosa eg Aspirin
134.
e. Avoid steroidswhether systemic or oral steroid. They
make skin and mucous membrane thin which lead to
ulceration
f. Advice on taking milk frequently. It facilitates ulcer
healing. Take at least twice a day ( a glass)
g. Avoid spiced food eg tea, coffee, cocacola, lemon
h. Promote emotional stability in pts with stress sometimes
mild sedative in case of anxiety reduces stress
i. Incase of bleeding PUD then give: iv fluids, take blood for
GXC, transfuse if he has lost a lot of blood or is in shock,
give hematinics
135.
DRUGS
Antacids
• Could beused in tablets or liquid form although they
may have low efficacy and poor compliance but they
are inexpensive and cheaply available
• Magnesium trysylicate and aluminium hydroxide
• Can be in doses ie 2 tabs TDS and not more than 10
tabs in a day for 4-6 weeks or until pts recover
• Liquid or missed antacid 15-30 mls TDS 4-6 weeks eg
Relcer and Maalox suspension
• Antacid combined with antispasmodic like bascopan
are good for pain relieve as compared to H2 antagonist
136.
Side effects ofantacid
• May lead to alkalosis
• Increase in metal like magnesium in body leading to
electrolyte imbalance
• Poor palatability
• Constipation/ diarrhea
137.
H2 receptor antagonist
•They block release of histamine which stimulate release of
gastric secretion
• Tagamet 400mg BD for 4-6 weeks or 800mg OD at bed
time or
• Sandak 150mg BD or 300mg OD at bed time for 4-6 weeks
• They are effective
• They give healing in 80% of pts who become symptomless
within one week
• If The pt doesn’t become symptomless with 1 week the dx
is incorrect and pts may be reviewed
138.
Side effects oftargamet
• Confusion especially in elderly as a mental problem
• Liver damage
• Diarrhea
• Acute pancreatitis
• Impaired hepato- renal function
• Gynecomastia
• Skin rash
• Impaired metabolism of warfarin and heparin
• Impotence
• Bleeding tendencies
• Rebound phenomenon
139.
Side effects ofsandak
• Headache
• Dizziness
• Leukemia with prolonged use
• Thrombocytopenia
• Confusion
Other drugs thatcan be used
a. Proton pump inhibitors
• They inhibit hydrogen and potassium and so it is called
proton pump
• Eg omeprazole ( losec) 40mg nocturnal for 4-6 weeks
• Is a good drug
• Good compliance
• Expensive
• Efficacy not as good as H2 antagonists
b. Ulcer coating drugs ( GI agents)
• Sucralfate ( caratate) –enhances healing by coating the
ulcer therefore protecting it against further injuries
142.
c. Prostaglandins
• Misoprostol– enhances mucosal defense by reducing
HCL secretion
d. Antibiotics and flaggyl
• Used with any of the above drugs to form triple therapy
• They are given for a period of one week
• The purpose is to clear H. pylori which is implicated in
formation of ulcers and poor healing
143.
SURGICAL TREATMENT
indications
• Perforation
•Obstruction
• Severe hematemesis
• Recurrent( repeated relapses despite medical
treatment)
• Failure of healing on medical treatment
• Non compliance to medical rx
• Gastric outflow ( pyloric stenosis)
144.
Types of surgery
•Vagotomy- removing of vagus nerve
• Gastroduodenostomy
• gastrojejunostomy
145.
IMPORTANT FEATURES
Gastric ulcers
•The ulcer may be asymptomatic
• There maybe dull or burning epigastric pain
precipitated by food 30-60min latter
• Relieved by alkaline solutions eg milk or vomiting
• Rebound last approximately 2-3 weeks with an
interval of relief for several weeks
• Common in older people usually > 40 years
• Average grade ( 55-65 peak grade)
146.
Duodenal ulcers
• Affectthe 1st
part of duodenum mainly the duodenal
curve
• The descending part is never affected coz it receives
pancreatic juice which neutralizes the acid
• Common in age 20-30 years
• Epigastric dull or burning worse 3-4 hours after a meal
or when the pts is hungry
• The pain awakes the pts at midnight more so at
around 2-3 am
• The pain may radiate to the back
147.
Clinical differences betweenGU
and PU
• Pain not relieved by food in GU but relieved by food in PU
• Mostly affect those over 40 yrs in GU and those of about
20-30 years in PU
• Weight loss is common in GU and weight gain in case of PU
• Vomiting relieves symptoms in GU while it is rare in PU
• GU has high instances of malignant changes unlike PU
• Increase of appetite in DU while poor appetite in GU
• Pain at night is evident in PU but absent in GU
• Excessive salivation occur in GU while no salivation in PU
148.
MANAGEMENT OF COMMONCOMPLICATIONS
Hemorrhage
• In this case the ulcer progressively develops and may
erode the major blood vessels causing bleeding
• Bleeding may be mild and chronic which leads to iron
deficiency
• There may be melaena stools and positive occult blood
test
• However the bleeding may be massive presenting with
fresh blood vomiting or coffee ground vomitus
• There may be features of shock: thread pulse rate , low
blood pressure, pallor, shallow increased respiratory rate
149.
Treatment
• Admit thepts
• Put up an I.V line preferably with plasma expanders.
However in absent of plasma expanders give normal saline
• Take blood for GXC at least 2 units and if blood ready
transfuse if the patient is in shock or has lost a lot of blood
• NGT for suctioning ( decompress stomach and assess the
level of bleeding to assess the amount of blood loss or
decompress stomach and hence control bleeding
• Monitor vital signs ie Bp and pulse rate
• Surgery if bleeding continues despite pts being on medical
treatment or if bleeding is very severe
150.
2. Perforation ofgut
• It may lead to peritonitis
• Common site of perforation is the anterior part
covered by peritoneum
• Gastric content spills over into the peritoneum
along with blood and causes peritonitis
151.
presentation
• Severe suddenonset of upper abdominal pain
• Fear to move or bleed
• Board like rigidity on abdominal examination
• Reduced or no bowel sounds ( coz of peritonitis)
4. Hour glass
•Results from scarring of chronic ulcers involving
lesser curvature leading to a deformity called hour
glass stomach
• Stomach loses its shape
Types
1. Ulcerative carcinoma
•Is the commonest
2. Polypoid carcinoma
• Appears like cauliflower mass protruding into the lumen
3. Infiltrating carcinoma
• Penetrate the entire stomach wall and destroy the
ruggae and may further result in obstructive of gastric
outflow
162.
Histology
• 90% areadenocarcinoma
• Most of them arise from antrum of lesser curvature
163.
prognosis
• 5 yearssurvival rate following diagnosis is very poor
• Therefor prognosis is poor and some oncologists
refer to it as the captain of death
164.
Spread
• Local spreadto adjacent organs
• Lymphatic spread
• Hematogenous spread to distance organs like liver
and pancreas
165.
Clinical features
• Adultof above 50 years
• Indigestion and abdominal distension
• Abdominal pain not related to food initially although later
may be aggravated by food, this helps to rule out PUD
• Nausea
• Anorexia
• Heartburn
• Persistence vomiting
• Cachexia
166.
• Malaise
• Dizziness
•On exam the pts is markedly wasted
• Pallor
• +/- jaundice
• Dehydration coz of failure to retain food
• The abdomen is scaphoid with hepatomegaly
• Palpable hypochondrium or fixed epigastric mass
• +/- ascitis
167.
Others
• Hematemesis
• Supraclavicularlymphadenopathy especially on the
left. Virchow's glands or trosiers nodes/sign hence
inflamed Virchow's gland is positive due to spread
on lt side of supraclavicular l. nodes
• Other l. nodes like groin and axillary may be
enlarged
• Liver is usually irregular and firm due to deposits
Investigations
• Full hemogram+ ESR- decreased Hb and elevated ESR
• Endoscopy – to visualize the tumor and biopsy may be taken at
same time
• Stool for occult blood- will be positive
• Barium meal to rule out PUD
• Plain abdominal x-ray may show abdominal calcification and
this may rule out other condition in the abdomen
• Ultrasound to rule out metastasis into liver
• LFTs- the normal values are altered incase of metastasis
• Chest X-ray to rule out metastasis to the lungs
• Gastric lavage for cytology
170.
Treatment
specific
• Partial gastrectomyin early stages or total
gastrectomy. They are done to prolong life however
this is not done coz most of time the tumor is
diagnosed when in late stages
• Radiotherapy which may be combined with surgery
• Chemotherapy where cytotoxic drugs are used
especially in metastasis to prolong life
171.
Supportive
• Analgesics
• Rehydrationincase dehydrated
• Transfusion or hematemics depending on degree of
anemia
• Treatment of recurrent infections
DIARRHEA
• Is definedas passage of watery/ loose stool/motion
two or more times in 24 hours which may be acute
or chronic
174.
Types of diarrhea
•Osmotic diarrhea
• Secretory diarrhea
• Exudative diarrhea
• Altered intestinal motility type of diarrhea
• Decreased absorptive surface type of diarrhea
175.
Osmotic diarrhea
• Nonabsorbed solid with increased intraluminal
oncotic pressure causes outpouring of water into
lumen this leads to passage of loose stool
• This type of diarrhea ceases on fasting
• It can also be brought about by bacterial
overgrowth in the lumen
176.
Secretory diarrhea
• Thereis active ion secretion causing obligatory
water loss
• This type is usually watery, profuse and not affected
by fasting
• It could be due to: viral infection eg Rota virus,
bacterial infection eg cholera and E.coli, protozoal
eg amoebiasis, medication eg colchine used in rx of
gout arthritis, Zollinger Ellison syndrome, HIV/AIDS
177.
Exudative diarrhea
• Ismainly due to inflammatory necrosis and
sloughing of colonic mucosa
• There could be a component of secretory diarrhea
• It is due to : salmonella, shigella, crohns disease,
campylobacter
178.
Altered intestinal motility
•Due to ulceration in the coordinated control of
intestinal movement
• In this case there is intermittent diarrhea
alternating with constipation
• Causes: DM, parasitic infection, oral antibiotics use,
upper GI bleeding, GI tumors
179.
Decreased absorptive surface
type
•Occurs as a result of surgical manipulation affecting
the GIT eg partial gastrectomy
• N/B:
• Diarrhea can also be classified as
a. Infective diarrhea
b. Non infective diarrhea
180.
Infective diarrhea
• Viral: HIV, Rota virus, hepatitis
• Bacterial- E.coli, salmonella, shigella and cholera
• Protozoal infection- G. lamblia and amoebiasis
• Parasitic infection- Ascaris and hookworm
• Fungal infection – candida albicans
181.
Non- infective
• Medication-colchicine drugs, antibiotic eg tetracyclines and
ampicillin
• Tumors – Zollinger Ellison syndrome and stomach
• Surgical – partial gastrectomy
• Malabsorption syndrome- DM, kwashiorkor
• Food poisoning
• Endocrine and metabolic causes – DM
• Crohn disease
• Ulcerative colitis
• Anatomical malformations of GI
182.
Parenteral causes
• Malaria
•Otitis media in children
• Pneumonia
• Tumors outside GI
• Psychological ( stress)
• This could be due to stress which affects intestinal
motility
183.
Investigations for diarrhea
•Stool for ova and cyst, C/S , occult blood
• Full hemogram plus ESR to rule out anemia or a
chronic condition, leukocytosis incase of infection
• Barium enema to rule out defects in rectum or anus
• Barium meal to rule out other GIT causes eg tumors
184.
N/B
• Diagnosis dependson signs and symptoms plus
investigation results
• Diarrhea is not a disease on itself but a sign of
organic lesions or condition
• It is significant to mention in your diagnosis or
impression that it should be written as diarrhea
secondary to suspected underlying cause eg
malaria, typhoid, food poisoning
185.
Management
• Rehydrate cozthe patients lose a lot of fluid most
of the time especially in severe cases of diarrhea.
Use half strength Darrow's, lingers lactate or 5%
dextrose
• Specific management depend on cause eg worms-
deworming, tumors- surgical removal
186.
Complications
• Dehydration
• Electrolyteimbalance
• Rectal prolapse ( in children)
• Malnutrition
• Anemia
• Malabsorption
• Edema
• Wasting in case of chronic diarrhea
• Metabolic alkalosis
• Hypoglycemia
• Acute renal failure
• Hypovolemic shock
Ulcerative colitis
• Itis a chronic illness which affects the colon
resulting into formation of an ulcer on its mucous
membrane
189.
Pathology
• The chronicmucosal inflammation is seen with
rectum almost always involved
• Inflammation is continuous proximally for a variable
extend and histological features include:
• Epithelial damage
• Inflammation
• Abscess formation
• Loss of goblet cells
190.
Etiology
• Unknown butis associated with psychological
factors eg stress
• Is more common between 20-40 years
191.
Clinical features
• Weightloss
• Diarrhea with mucous stools sometimes containing pus and
has bright red blood
• Onset is insidious ( gradual)
• Is associated with tenesmus with abdominal pain
• On exam the patient
• Wasted
• Low grade fever
• +/- anemia
• Tenderness particularly around iliac region ( left)
• Skin may show changes due to vit. Deficiency. This is called follicular
hyperkeratosis/ crazy pavements
Complications
• Secondary bacteriainfection leading to septicemia
• Perforation
• Peritonitis
• Hemorrhage
• Stricture formation in some case
• Dysplasia predisposing to ca colon
• Polyps formation
194.
Investigations
1. Full hemogram–ESR is elevated and Hb is decreased
2. Barium enema to rule out condition of rectum or anus
which may also bleed eg tumors or hemorrhoids
3. Stool for ova and cyst to rule out infective causes of
diarrhea eg hookworm and amoebiasis
4. Stool for macroscopy for eggs
5. Stool for culture and sensitivity – shigella , salmonella
6. Stool for occult blood to rule out PUD or any other upper GI
bleeding cause
7. Sigmoidoscopy- to visualize area affected and biopsy may
be taken to rule out ca colon and rectum
195.
Management
supportive
• Analgesic/ antipyretic
•Hematemics or transfusion depending on rate of
anemia
• Rehydration
• High pressure diet
• Low residue diet
• Mild sedation incase of anxiety
• Psychological counselling and support regarding
what is causing the stress
196.
Specific
• Surgical interventionincase of complications eg
stricture, perforation, severe hemorrhage
• Corticosteroid eg prednisone for about 2 weeks
starting with high dose and tapering ( to reduce
adrenal insufficiency)
• Eg start with 60mg stat, then continue with 40 mg
BD for 3 days, then 40mg OD for 4 days, then 20mg
BD for 5 days, 20mg OD for 3 days, 10mg OD for 3
days, then 5mg OD for 5 days
Malabsorption syndrome
• Itis defective absorption of food substance eg
protein, carbohydrates, vit by small intestine and
subsequent chronic diarrhea , abdominal distension
and malnutrition
199.
Etiology
1. Deficiency ofpancreatic enzyme as in:
• Chronic pancreatitis
• Ca pancreas
• Cystic fibrosis of pancreas
2. Deficiency of bile salts as incase of biliary obstruction-
bile salt deficiency may also be due to bacterial
obstruction as it occurs in blind loop diverticulum
3. Diseases of small intestines eg:
• Crohn's disease, fistula of small intestines
• Ulcerative colitis, lymphatic obstruction as in Hodgkin disease
• Bacterial enteritis, Tb, mesenteric thrombosis, parasitic infection
( candidiasis)
200.
4. Drugs –neomycin, kanamycin, colchicine( gouts).
They destroy normal flora of GI and affect
facilitation of absorption of some nutrients
5. HIV patients due to secondary bacterial infection
6. Surgery eg gastrectomy , gastroduodenostomy
201.
Clinical features
• Onsetis gradual
• Loss of weight
• Failure of growth
• Abdominal distension due to hypoalbuminemia and
hypotonic muscles
• Diarrhea with steatorrhea ( passing loose bulk pale
offensive and grey stool that floats on water). This
is due to lack of bile salts
202.
On exam
• Anemicdue to iron, folic acid or vit. B deficiency
• Hemorrhage due to B12
• Osteomalacia due to vit D deficiency
• Features of scurvy due to lack of vit C
• Dehydration
• Stomatitis
• Finger clubbing
• Progressive wasting
203.
Differentials
• Ulcerative colitis
•Lactose intolerance ( hypersensitivity to lactose
substance leading to diarrhea. It occurs commonly
in children and during weaning
204.
Investigations
1. Full hemogramand ESR- wbc elevated, Hb
decreased, ESR increased
2. Barium follow through- may show dilated loop of
intestine. After food, 3hours
3. Biopsy shows atrophic villi
4. Stool for occult blood to rule out upper GI
bleeding
5. Stool for ova and cyst to rule out parasitic
infections of GI
205.
Treatment
• Remove theunderlying cause eg biliary
obstruction- surgical removal, Tb enteritis- give ant
Tb drugs
• Transfuse or give hematinic depending on severity
of anemia
• If dehydrated- rehydrate and improve nutrition
Bacillary dysentery
• Itis characterized by:
• Diarrhea with passage of blood and mucous in stool
• The patient experiences tenesmus
208.
Etiology
• S. dysentery
•S. flexineri
• S. boydi
• S. sonnei
• The commonest is s. dysentery in developing
countries
• It is associated with severe profuse bloody diarrhea
otherwise in developed countries s. flexineri is the
commonest
209.
Pathology
• The microorganismdon’t invade the blood but
superficial mucosal of intestines causing micro
abscess which slough through stool
• They produce exotoxin which cause damage in the
GI walls ( intestinal mucosal)
210.
Transmission
oral fecal
• Thisis through person to person , handshaking, and in this
case crowded housing and institutions are associated with
this method
• May also be through flies moving from contaminated areas
to food and when eaten such food leads to ingestion of
microorganism and hence the infection
• Contamination of water and food by poor hygiene also
substantially contribute to the infection
• N/B: it is said to be rare in children <6 months who are
breastfeeding coz they don’t take some food orally other
than food given by mother and breastfeeding which is
usually clean
211.
Presentation
• Sudden onsetwith abdominal pain
• Diarrhea of high frequency
• The stool are blood stained and have little or no
mucus
• Fever
• +/- vomiting
• General body weakness
• Marked tenesmus
212.
Investigations
• Stool forova and cyst to rule out worm infestation
like the hookworm which can cause diarrhea or
amoebiasis
• Stool for culture and sensitivity
• Direct macroscopy – this may show numerous pus
cells
• Full hemogram- neutrophilia
213.
Management
general
• Analgesic/ antipyretic
•Rehydration with Hartman's solution, falos soluion,
iv fluids
• Transfuse or give hematinic depending on severity
of anemia
• Improve hygiene
• Improve nutrition
• Give bed rest
214.
Specific
• Sulphur drugsare drugs of choice: DOC nalidixic
acid 500mg TDS for 5 days( septrin 2 tabs BD may
cure condition however there is high resistance)
• Treatment should otherwise be guided by results of
culture and sensitivity
• Prophylactic treatment can be given for those in
contact with patient
215.
Differentials
• Amoebic dysentery
•Cholera- rice water stool not blood stained
• Typhoid fever/salmonella- step ladder fever, onset gradual,
constipation alternating with diarrhea, ross spots
• Food poisoning- typical hx which points at having eaten
suspicious food and usually many people are involved
• Viral diarrhea- acute in onset , lymphocytosis, no growth in
viral diarrhea, not blood stained instead liver failure as a
result of viral hepatitis and Ebola
• Ulcerative colitis- gradual onset, associated with wasting
• Giardiasis- associated with steatorrhea, no blood in stool
Amoebic dysentery
• Cause-Entamoeba hystolytica
• It exist in acystic and vegetative form ( trophozoite)
• The cyst are swallowed in food and water
• Incubation period is about 9-90 days
218.
Presentation
• Gradual onset
•Recurrent history
• Diarrhea up to 5 times in 24hrs and usually less than 10 times
• Diarrhea usually alternate with constipation
• Stool contain mucus with very little or no blood
• Stools are usually offensive and copious in amounts
• +/- tenesmus but not as pronounced as in bacillary dysentery
• On exam, the pts is afebrile but incase of hepatic liver abscess the pts
will be febrile
• There is tenderness over caecum or transverse colon or in right iliac
fossa
• Incase the liver is affected, there will be tenderness over enlarged liver
Treatment
• Rehydrate withHartman's solution
• Transfuse/hematinic incase of anemia depending
on the grade of anemia
• Proper hygiene
• Analgesic for pain
• Monitor vital signs
221.
Specific
1. Metronidazole –800mg TDS for 1 week. Act
mainly on trophozoites and doesn’t destroy cysts.
Can also be given as 1.2 g OD for 3 days
2. Incase of liver abscess or hepatitis give 500mg iv
TDS for 5 days then tabs 800mg TDS for 5 days
222.
Other drugs
1. Entamizole500mg TDS for 5 days- destroys both trophozoites
and cysts. Can also treat amoebic liver abscess only that it will
be slow yet in liver abscess you need to be aggressive
2. Tinidazole 2g stat or OD for 3 days
3. Tetracycline – good drug as it penetrates through tissues
hence destroy tissue amoebiasis but less effective
4. Chloroquine injection and tabs- treatment duration is long but
effective . It also treats amoebic hepatitis
5. Gabbrarol- destroys the cysts as well as the trophozoite but
expensive 250mg OD for 5 days
• N/B: among the above alternative drugs, entamizole, tinidazole
and Gabbrarol can be prescribed incase of lack of metronidazole
223.
Prevention
• Proper hygiene
•Proper refuse disposal
• Washing hands before eating
• Discourage eating raw food eg fruits, vegetables or
undercooked food
• Health education
• Prophylactic treatment for food handlers
224.
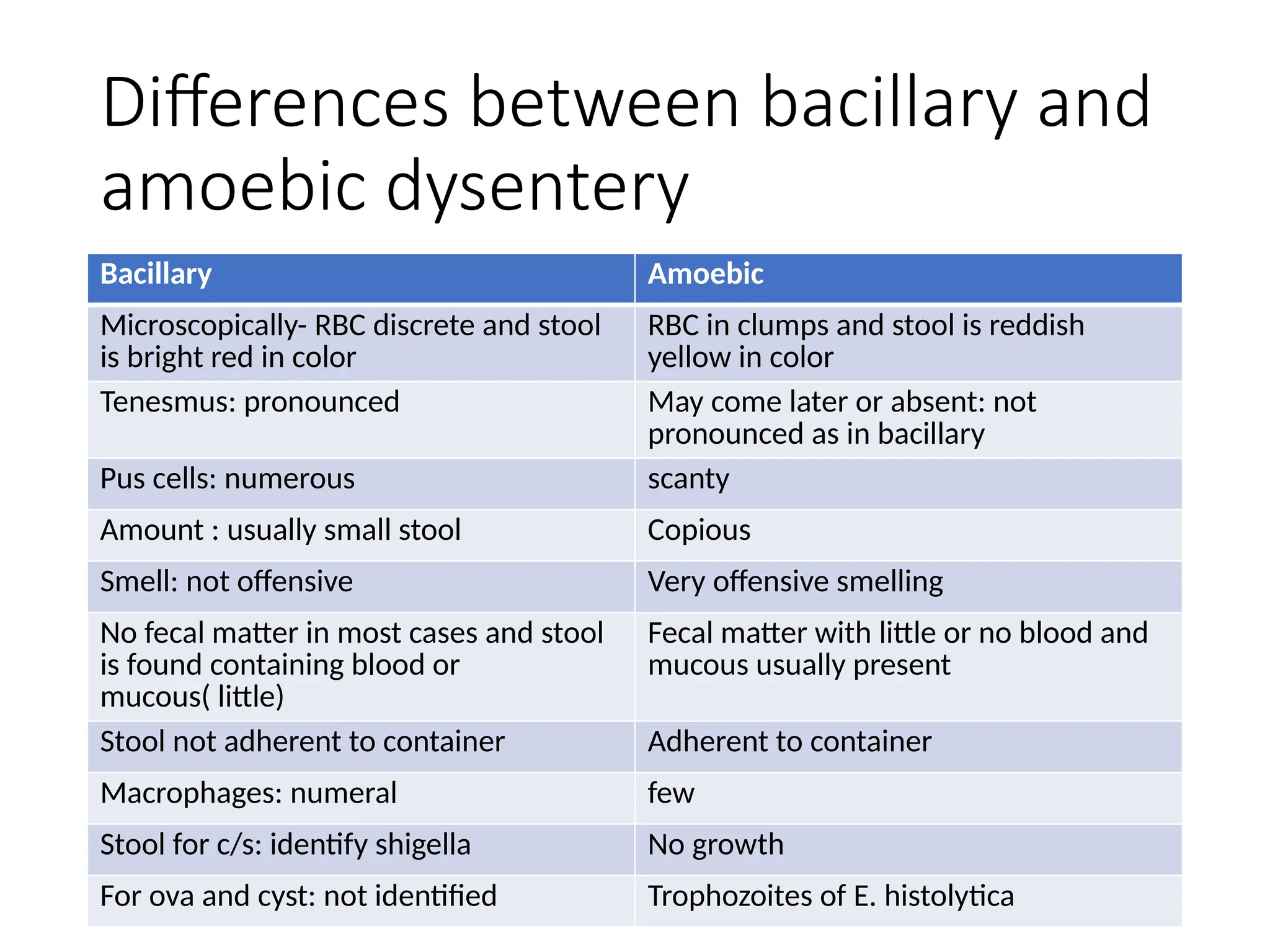
Differences between bacillaryand
amoebic dysentery
Bacillary Amoebic
Microscopically- RBC discrete and stool
is bright red in color
RBC in clumps and stool is reddish
yellow in color
Tenesmus: pronounced May come later or absent: not
pronounced as in bacillary
Pus cells: numerous scanty
Amount : usually small stool Copious
Smell: not offensive Very offensive smelling
No fecal matter in most cases and stool
is found containing blood or
mucous( little)
Fecal matter with little or no blood and
mucous usually present
Stool not adherent to container Adherent to container
Macrophages: numeral few
Stool for c/s: identify shigella No growth
For ova and cyst: not identified Trophozoites of E. histolytica
225.
Other causes ofdysentery
• S. mansoni
• Salmonella infection( typhoid)
• Dysentery is an infection of GI resulting to bloody diarrhea.
Otherwise causes of bld diarrhea include:
• Ulcerative colitis, ebola, liver failure
• Rectal trauma
• Ca colon/ rectum
• Dysentery, drugs like warfarin and heparin
• Hemorrhoids
• Food poisoning
• Anal fissures and fistula, blood bleeding disorders eg
thrombocytopenia, hemophilia
• Polyps of colon, diverticula disease of colon
Amoebic liver abscess
•Cause- E. histolytica
• Usually found in the colon
• The infection also causes amoebic dysentery
• If the amoeba is in the colon it erodes a vein and enters into
the vein and therefore it is carried to liver via portal vein
• Not all patients who suffer amoebic liver abscess suffer from
amoebic dysentery
• Usually affects the right lobe more commonly than the RT
• Micro abscess in the liver forms which later coalescence to
form one large solitary tender abscess
• Males are more affected than females
228.
Signs and symptoms
•Previous hx suggesting amoebic dysentery may or
may not be there
• Onset is sudden with fever , sweating, general
malaise, anorexia, weight loss
• Pain in RT upper quadrant which may be pleuritic
and radiate to the neck
229.
On exam
• Illlooking
• Dyspneic
• Jaundice is unusual
• Tender hepatomegaly
• Palpable epigastric mass if LT lobe is involved
• Bulging of the intercostal spaces occupied by the
liver
• Plus or minus crepitations due to spread of abscess
to involve the RT lung
230.
Investigations
1. Blood forFHG and ESR- there is leukocytosis with
elevated eosinophils
2. Stool for ova and cyst- motile trophozoites containing
ingested RBC may be seen
3. Blood for liver function test- usually normal
4. Plain abdominal x-ray shows raised RT diaphragm coz of
the mass/ abscess
5. Chest x-ray show opacities in RT lung and pleural effusion
may be seen
6. Aspiration is hardly done but fluid is usually sterile
containing scanty amoebae ( trophozoites)
231.
7. Amoebic latextest- it is positive incase of
amoebic liver abscess. In this case a specific
reagent react with antibodies that are produced
against amoebiasis
8. Abdominal ultrasound to show abscess
9. Ct scan shows the abscess
232.
Treatment
• Iv metronidazole500mg TDS for 1 week and
metronidazole oral 1.2 g OD for 1 week
• Surgical treatment if the abscess has ruptures.
Older cases may be very large, otherwise respond
to metronidazole
Complications
• Rupture intodiaphragm and lung causing: pleural
effusion, Broncho hepatic fistula, amoebic lung
abscess
• Rupture into abdomen leading to amoebic
peritonitis
• Rapture into pericardium leading to amoebic
pericarditis
235.
Differentials of tender
hepatomegaly
•Viral hepatitis
• Hydatid cysts
• Malaria
• Congestive cardiac failure
• Pyogenic liver abscess
• Hepatoma ( primary and secondary especially in late stages)
• Tertiary syphilis
• Sickle cell disease in children
• Chronic myelogenic leukemia
• Metastatic carcinoma
Associated factors
• Familyhx of ca colon
• Hypercholesteremia
• Ulcerative colitis
• Heart disease especially chronic disease
• Low fiber foods- that is why it is more common in
developed countries than underdeveloped
242.
Pathology
• Are adenocarcinoma type of tumors
• Maybe polypoid , fungating or constricting
243.
Clinical features
• Wasting
•Constipation
• Diarrhea
• Rectal bleeding ( striking features)
• Abdominal distension around LT iliac fossa as a result of tumor
• Abdominal pain with tenesmus and back pain
• Plus or minus anemia
• Perforation volvulus or inguinal hernia coz of straining at stool
• Inguinal lymohadenopathy
244.
Investigations
• Barium meals
•Barium enema
• Full hemogram + ESR- decreased Hb and elevated
ESR
• Sigmoidoscopy – to visualize the rectum and
sigmoid colon and also helps in biopsy taking
Diverticular disease
• Herniationor sac like protrusion of mucosa through
musclularis coat due to increased intraluminous
pressure in the colon
• They are associated with low fiber diet and the
sigmoid site. However they may occur in other
areas of GI
249.
Presentation
• May beasymptomatic
• Recurrent lower abdominal pain alternating with
constipation relieved by defecation
• Pain and fever especially if diverticulitis occur ( if
inflamed)
250.
Investigations
• Sigmoidoscopy tovisualize pouch and rule out ca
colon
• Full hemogram + ESR- WBC increased incase of
infection. ESR may be raised
• Barium enema or meal to visualize sacs or pouches
filled with barium
Complications
• Fistula formation
•Perforation
• May rupture
• Peri-colic abscess
• Hemorrhage- bleeding gives similar presentation as
in ca colon although more occasional as compared
to ca colon
Causes
Anorectal causes
• Hemorrhoids
•Anal fissures and fistula
• Proctitis- inflammation of rectum following worms
like s. mansoni infection
• Trauma
• Tumors of anus and rectum
Investigations
• Full hemogram
•Barium enema to visualize diverticular
• Sigmoidoscopy
• Stool for ova and cyst to rule out amoebiasis
• Blood culture and sensitivity to rule out shigella
• Stool for ova – Schistosoma
• Liver function test in suspicion of liver failure
Supportive
• Admit thepts
• Transfuse or give hematinic as per the degree of
anemia
• Analgesic incase of pain
• Health education on hygiene of pts
• Good nutrition
Constipation
• It ispassage of infrequent hard less stool less than
3 times in a week or passage of no stool at all in 24
hours
265.
Causes
• Mainly associatedwith disordered colonic to ano-rectal
dysfunction as a result of motility disturbances, drugs, systemic
disease affecting GI, etc
• Constipation can also occur in:
1. Chronic illness where there is mental impairment resulting in
inactivity or physical immobility( stress)
2. Lack of fiber in food
3. Generalized muscle weakness eg in stress or incase of anxiety
4. Obstructive lesion eg anal fissure, stricture, hemorrhoids,
tumors, or fissures
5. Drugs eg codeine( narcotics) and some analgesics and antacids
266.
6. Endocrine causeseg diabetes and hypothyroidism
7. Surgical causes eg intestinal
obstruction( common type of presentation is
absolute constipation)
8. Dehydration
9. Psychological factors eg emotions and stress
267.
Management
• Treatment ofunderlying cause
• Advice on fiber food eg Sukuma and cowpeas
• Give plenty of fluid eg water or porridge
• Encourage use of fruits like pawpaw, pineapples,
water, water melon, bananas
• In extreme cases, give laxative drugs: eg bisacodyl 2
tabs noctate for 3 days or PRN
• Soap enema- advisable if constipation has stayed for
more than 2 weeks and there must be a reason for
agent use ie severe abdominal pain
Vomiting
• Vomiting involvedboth autonomic and somatic neural pathway
• During vomiting the following contract to increase pressure of
abdomen( intra)
• Diaphragm
• Intercostal muscles
• These is followed by relaxation of lower esophageal sphincter
which cause gastric content to eject forcefully
• Vomiting is associated with:
• Nausea
• Vetching
• Salivation
• Anorexia and dyspepsia
270.
• Vomiting isassociated with the following symptoms
• Abdominal pain
• Fever
• Diarrhea
• Drugs, headache, vertigo
• Relation to food
• Weight loss
• On exam the following signs may be revealed
• Dehydration
• Fever
• Infections
• Search for abdominal masses, peritonitis, intestinal obstruction,
papilloedema, nystagmus, photophobia, neck stiffness
































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)














