Model Call Girl in Tilak Nagar Delhi reach out to us at 🔝9953056974🔝
Git
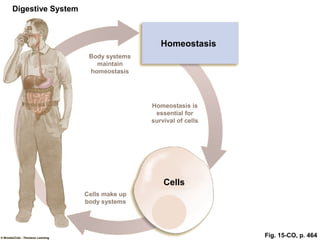
1. Fig. 15-CO, p. 464
Digestive System
Body systems
maintain
homeostasis
Homeostasis is
essential for
survival of cells
Cells
Cells make up
body systems
Homeostasis
5. Fig. 15-2, p. 470
Body wall
Peritoneum
Mesentery
Serosa
Submucosa
Duct of large
accessory digestive
gland (i.e., liver
or pancreas) emptying
into digestive tract
lumen
Outer longitudinal muscle
Inner circular muscle
Muscularis
externa
Lamina propria
Mucous membrane
Muscularis mucosa
Myenteric plexus
Submucous plexus
Lumen
Mucosa
6. Fig. 15-3, p. 471
External
influence
Local changes in
digestive tract
Receptors in digestive tract
Intrinsic
nerve plexuses
Extrinsic
automatic
nerves
Gastrointestinal
hormones
Smooth muscle
(contraction for motility)
Exocrine gland cells
(secretion of digestive juices)
Endocrine gland cells
(secretion of gastrointestinal
and pancreatic hormones)
Self-
excitable
= Short reflex
= Long reflex
= Hormonal pathway
7. Fig. 15-4, p. 473
Cerebral cortex Other inputs
Salivary center
in medulla
Conditioned
reflex
Pressure receptors
and chemoreceptors
in mouth
Simple reflex Autonomic nerves
Salivary glands
Salivary secretions
8. Fig. 15-5a, p. 474
Nasal passages
Hard palate
Soft palate
Uvula
Pharynx
Epiglottis
Esophagus
Trachea
Bolus
Tongue
Glottis at entrance
of larynx
9. Fig. 15-5b, p. 474
Tight apposition of vocal folds across
glottis prevents food from entering
respiratory airways (viewed from above)
Swallowing center
inhabits respiratory
center in brain stem
Elevation of uvula
prevents food from
entering nasal passages
Position of tongue
prevents food from
re-entering mouth
Epiglottis is pressed
down over closed
glottis as auxiliary
mechanism to prevent
food from entering
airways
10. Bolus
Fig. 15-6, p. 475
Ringlike peristaltic
contraction sweeping
down the esophagus
11. Fig. 15-7, p. 476
Esophagus Fundus
Smooth
muscle
Oxyntic
mucosa
Antrum
Pyloric
gland
area
Duodenum
Pyloric
sphincter
Stomach
folds
Body
Gastroesophageal
sphincter
12. Fig. 15-8a, p. 477
Esophagus
Duodenum
Pyloric sphincter
Stomach
Gastroesophageal
sphincter
Movement
of chyme
Peristaltic
contraction
Direction of
movement
of peristaltic
contraction
Gastric emptying
13. Fig. 15-8b, p. 477
Gastric mixing
Peristaltic
contraction
16. Table 15-3 (1), p. 480
Oxyntic
mucosa
Pyloric
gland
area
Stomach
lumen
Gastric
pit
Mucosa
Submucosa
17. Table 15-3 (2), p. 480
In oxyntic mucosa
Gastric
pit
Gastric
gland
Surface epithelial cells
Mucosa cells
Chief cells
Parietal cells
Enterochomaffin-
like (ECL) cells
In pyloric gland area
G cells
D cells
18. Fig. 15-9, p. 482
Autocatalysis
Digestion
Protein
Peptide fragments
Gastric
lumen
HCI
Pepsinogen Pepsin
21. Fig. 15-10, p. 484
Mucus coating
Impermeable
to HCI
Cells lining gastric mucosa
(including those lining
gastric pits and glands)Submucosa
Tight
junction
Luminal contents
22. Fig. 15-11, p. 487
Duodenum
Bile duct
from liver
Stomach
Hormones
(insulin,
glucagon)
Blood
Endocrine portion
of pancreas
(Islets of Langerhans)
The glandular portions of
the pancreas are grossly
exaggerated
Duct cells
secrete aqueous
NaHCO3 solution
Acinar cells
secrete digestive
enzymes
Exocrine portion of panaceas
(Acinar and duct cells)
23. Fig. 15-12, p. 488
Acid in
duodenal
lumen
Fat and protein
products in
duodenal lumen
Secretion release
from duodenal
mucosa
CCK release
from duodenal
mucosa
(Secretin carried
by blood)
Pancreatic acinar
cells
Secretion of aqueous
NaHCO3 solution into
duodenal lumen
Secretion of
pancreatic digestive
enzymes into
duodenal lumen
Pancreatic duct
cells
Neutralizes Digests(CCK carried
by blood)
25. Fig. 15-14a, p. 490
Branch of
hepatic
portal
vein
Bile
duct
Sinusoids
Branch
of
hepatic
artery
Bile canaliculi
Central vein
Cords of
hepatocytes
(liver cells)
Hepatic
portal vein
Hepatic
artery
To
hepatic
duct
26. Fig. 15-14b, p. 490
Branch of
hepatic artery
Branch of
hepatic portal vein
Connective
tissue
Kupffer cell
Bile
canaliculi
Sinusoids
Central vein
Hepatic plate
Cords of hepatocytes
(liver cells)
Bile
duct
27. Fig. 15-15, p. 490
Bile salts Cholesterol
Liver
Common bile duct
Duodenum
Gallbladder
Sphincter of Oddi
Portal
circulation
Terminal ileum
Colon
28. Fig. 15-16a, p. 491
Negativity charged
H2O-soluble portion
(a carboxyl group at
the end of a glycine
or taurine chain)
Lipid-soluble portion
(derived from cholesterol)
Small lipid (fat)
droplet with bile
salt molecules
absorbed on
its surface
29. Fig. 15-16b, p. 491
Large fat droplet
Through action
of bile salts
Lipid
emulsion
30. Fig. 15-17, p. 492
Hydrophobic core
Hydrophilic shell
All lipid-soluble
Cholesterol
Bile salt
Water-soluble portion
Lipid-soluble portion
Water-soluble portion
Lipid-soluble portion
Lecithin
34. Fig. 15-20ab, p. 497
Circular
fold
Villus
(Continue to next slide)
35. Fig. 15-20cd, p. 497
Epithelial cell
Mucous cell
Central lacteal
Capillaries
Crypt of Lieberkühn
Arteriole
Venule
Lymphatic vessel
Microvilli
36. Fig. 15-23, p. 500
Lipid emulsion
Micelles
Epithelial
cell of villus
Lumen
(Exocytosis)
Central lacteal
Aggregate and
coated with
lipoprotien
Short or
medium
chain
Basement
membrane
Capillary
Lumen
Micelles
diffusion
Micelle
Microvillus
Fatty acids,
monoglycerides
Passive absorption
FIGURE 15-1: An example of hydrolysis. In this example, the disaccharide maltose (the intermediate breakdown product of polysaccharides) is broken down into two glucose molecules by the addition of H2O at the bond site.
TABLE 15-1: Anatomy and Functions of Components of the Digestive System.
TABLE 15-1: Anatomy and Functions of Components of the Digestive System.
FIGURE 15-2: Layers of the digestive tract wall. The digestive tract wall consists of four major layers: from the innermost out, they are the mucosa, submucosa, muscularis externa, and serosa.
FIGURE 15-3: Summary of pathways controlling digestive system activities.
FIGURE 15-4: Control of salivary secretion.
FIGURE 15-5: Oropharyngeal stage of swallowing. (a) Position of the oropharyngeal structures at rest.
FIGURE 15-5: Oropharyngeal stage of swallowing. (b) Changes that occur during the oropharyngeal stage of swallowing to prevent the bolus of food from entering the wrong passageways.
FIGURE 15-6: Peristalsis in the esophagus. As the wave of peristaltic contraction sweeps down the esophagus, it pushes the bolus ahead of it toward the stomach.
FIGURE 15-7: Anatomy of the stomach. The stomach is divided into three sections based on structural and functional distinctions—the fundus, body, and antrum. The mucosal lining of the stomach is divided into the oxyntic mucosa and the pyloric gland area based on differences in glandular secretion.
FIGURE 15-8: Gastric emptying and mixing as a result of antral peristaltic contractions.
FIGURE 15-8: Gastric emptying and mixing as a result of antral peristaltic contractions.
TABLE 15-3: The Stomach Mucosa and the Gastric Glands.
TABLE 15-3: The Stomach Mucosa and the Gastric Glands.
TABLE 15-3: The Stomach Mucosa and the Gastric Glands.
FIGURE 15-9: Pepsinogen activation in the stomach lumen. In the lumen, hydrochloric acid (HCl) activates pepsinogen to its active form, pepsin, by cleaving off a small fragment. Once activated, pepsin autocatalytically activates more pepsinogen and begins protein digestion. Secretion of pepsinogen in the inactive form prevents it from digesting the protein structures of the cells in which it is produced.
FIGURE 15-10: Gastric mucosal barrier.
FIGURE 15-11: Schematic representation of the exocrine and endocrine portions of the pancreas. The exocrine pancreas secretes into the duodenal lumen a digestive juice composed of digestive enzymes secreted by the acinar cells and an aqueous NaHCO3 solution secreted by the duct cells. The endocrine pancreas secretes the hormones insulin and glucagon into the blood.
FIGURE 15-12: Hormonal control of pancreatic exocrine secretion.
FIGURE 15-13: Schematic representation of liver blood flow.
FIGURE 15-14: Anatomy of the liver. (a) Hepatic lobule.
FIGURE 15-14: Anatomy of the liver. (b) Wedge of a hepatic lobule.
FIGURE 15-15: Enterohepatic circulation of bile salts. The majority of bile salts are recycled between the liver and small intestine through the enterohepatic circulation (blue arrows). After participating in fat digestion and absorption, most bile salts are reabsorbed by active transport in the terminal ileum and returned through the hepatic portal vein to the liver, which resecretes them in the bile.
FIGURE 15-16: Schematic structure and function of bile salts. (a) Schematic representation of the structure of bile salts and their adsorption on the surface of a small fat droplet. A bile salt consists of a lipid-soluble part that dissolves in the fat droplet and a negatively charged, water-soluble part that projects from the surface of the droplet.
FIGURE 15-16: Schematic structure and function of bile salts. (b) Formation of a lipid emulsion through the action of bile salts. When a large fat droplet is broken up into smaller fat droplets by intestinal contractions, bile salts adsorb on the surface of the small droplets, creating shells of negatively charged, water-soluble bile salt components that cause the fat droplets to repel each other. This action holds the fat droplets apart and prevents them from recoalescing, increasing the surface area of exposed fat available for digestion by pancreatic lipase.
FIGURE 15-17: Schematic representation of a micelle. Bile constituents (bile salts, lecithin, and cholesterol) aggregate to form micelles that consist of a hydrophilic (water-soluble) shell and a hydrophobic (lipid-soluble) core. Because the outer shell of a micelle is water soluble, the products of fat digestion, which are not water soluble, can be carried through the watery luminal contents to the absorptive surface of the small intestine by dissolving in the micelle’s lipid-soluble core.
FIGURE 15-18: Segmentation. Segmentation consists of ringlike contractions along the length of the small intestine. Within a matter of seconds, the contracted segments relax and the previously relaxed areas contract. These oscillating contractions thoroughly mix the chyme within the small-intestine lumen.
FIGURE 15-19: Control of the ileocecal valve/sphincter. The juncture between the ileum and large intestine is the ileocecal valve, which is surrounded by thickened smooth muscle, the ileocecal sphincter. Pressure on the cecal side pushes the valve closed and contracts the sphincter, preventing the bacteria-laden colonic contents from contaminating the nutrient-rich small intestine. The valve/sphincter opens and allows ileal contents to enter the large intestine in response to pressure on the ileal side of the valve and to the hormone gastrin secreted as a new meal enters the stomach.
FIGURE 15-20: Small-intestine absorptive surface. (a) Gross structure of the small intestine. (b) One of the circular folds of the small-intestine mucosa, which collectively increase the absorptive surface area threefold.
FIGURE 15-20: Small-intestine absorptive surface. (c) Microscopic fingerlike projection known as a villus. Collectively, the villi increase the surface area another tenfold. (d) Electron microscope view of a villus epithelial cell, depicting the presence of microvilli on its luminal border; the microvilli increase the surface area another 20-fold. Altogether, these surface modifications increase the small intestine’s absorptive surface area 600-fold.