
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pancreatitis
Similar to Pancreatitis (20)
Recently uploaded
Recently uploaded (20)
Pancreatitis
- 1. Pancreatitis
- 2. Heterogenic gland 1) EXOCRINE GLAND Ductal cells and centro-acinar cells secrete: AMYLASE active form LIPASE TRYPSIN CHYMOTRYPSIN inactive CARBOXYPEPTIDASE 2)ENDOCRINE GLAND Islets of Langerhans secrete • ALPHA CELLS – GLUCAGON • BETA CELLS – INSULIN • DELTA CELLS – SOMATOSTATIN AND GASTRIN • PP CELLS – p.polypeptides, vasoactive intestinal peptides , gastro intestinal inhibitor peptides
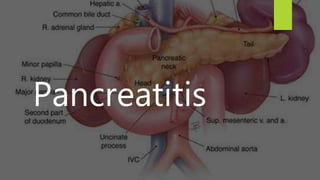
- 3. The pancreas is typically divided into five parts; Head – the widest part of the pancreas. It lies within the C-shaped curve created by the duodenum, and is connected to it by connective tissue. Uncinate process – a projection arising from the lower part of the head and extending medially to lie beneath the body of the pancreas. It lies posterior to the superior mesenteric vessels. Neck – located between the head and the body of the pancreas. It overlies the superior mesenteric vessels which form a groove in its posterior aspect. Body – centrally located, crossing the midline of the human body to lie behind the stomach and to the left of the superior mesenteric vessels. Tail – the left end of the pancreas that lies within close proximity to the hilum of the spleen. It is contained within the splenorenal ligament with the splenic vessels. This is the only part of the pancreas that is intraperitoneal.
- 5. Arterial blood supply Splenic artery ( branch of coeliac artery) Superior Pancreaticoduodenal artery – anterior and posterior(branches of the gastroduodenal (from coeliac trunk) Inferior Pancreaticoduodenal artery – anterior and posterior( branches of superior mesenteric arteries)
- 6. Venous drainage Portal vein Splenic veins Superior mesenteric veins
- 7. Lymph nodes This figure indicates the typical location of lymph nodes surrounding the pancreas. There is considerable individual variation in the location of lymph nodes and an image like this is idealized. Both A and B are anterior views. B includes some nodes that lie posterior to the pancreas.
- 8. Nerves supply Parasympathetic– Vagus nerves (secretory in nature) Sympathetic- greater , lesser& least splanchnic nerves (T5 TO T10) carrying pain fibres
- 9. Physiology Pancreatic secretion = 1500-2000 ml 1) Bicarbonates secretion 2) enzymes secretion 1)secretion of bicarbonates, Cl , Na , P ions is done by secretin hormone (released from duodenal mucosa ) in the presence of HCL, proteolytic byproducts, fatty acids and amino acids. Vasoactive intestinal peptides stimulates water bicarbonate secretion Insulin necessary for normal release of bicarbonates
- 10. Digestive Enzymes are synthesized on polysomes attached to endoplasmic reticulum. 1) Inactive forms of TRYPSIN, CHYMOTRYPSIN A & B , CARBOXYPEPTIDASE A&B. 2) Active forms of AMYLASE & LIPASE TRYPSINOGEN TRYPSIN CHYMOTRYPSINOGEN & CARBOXYPEPTIDASE
- 11. AMYLASE degrades starches to dissacharides LIPASE converts glycerol into fatty acids PANCREATIC PROTEOLYTIC enzymes converts proteins into peptides and amino acids
- 12. Cephalic Phase vagal stimulation – low volume enzyme rich fluid is secreted Gastric phase Gastrin stimulates i) enzyme secretion by pancreas ii) acid secretion by stomach Intestinal phase Acid enters duodenum, secretin stimulates pancreatic fluid & bicarbonate secretion Post cibal phase Inhibition of pancreatic secretion
- 13. Types of Pancreatitis 1. Acute 2. Acute relapsing 3. Chronic 4. Chronic relapsing
- 14. Pathogenesis 1. Gallstones and choledocholithiasis 2. Alcohol drinking 3. Obstruction=Acute pancreatitis may be the first sign of gallstones. Gallstones can block the pancreatic duct, which can cause acute pancreatitis. 4. Metabolic factors Hyperlipidemia Hyper calcemia , hyperparathyroidism 5. Postoperative pancreatitis
- 17. Symptoms of acute pancreatitis: Upper abdominal pain that radiates into the back; it may be aggravated by eating, especially foods high in fat. Swollen and tender abdomen Nausea and vomiting Fever Increased heart rate (tachycardia)
- 20. How Is Pancreatitis Diagnosed? measure levels in the blood of two digestive enzymes, amylase and lipase. High levels of these two enzymes strongly suggest acute pancreatitis. Pancreatic function test Glucose tolerance test to measure damage to the cells in the pancreas that make insulin Ultrasound, CT scan, and MRI, which make images of the pancreas so that problems may be seen ERCP to look at the pancreatic and bile ducts using X-rays Biopsy, in which a needle is inserted into the pancreas to remove a small tissue sample for study In more advanced stages of the disease, doctors may use blood, urine, and stool tests to confirm the diagnosis.
- 25. Complications Hemorrhage Pseudocyst formation Pancreatic abscess formation Obstruction of common bile duct or duodenum Acute renal failure (I/O chart should be maintained) Pancreatic ascites (abd girth is watched for ) Diabetes mellitus Pancreatic insufficiency leading to steatorrhoea, nutritional deficiency and at times diabetes
- 26. Conservative Management 1. Management of Shock & Electrolyte imbalance 2. Relief of pain 3. Suppression of Pancreatic Secretions (e.g.octreotide- inhibit secretion of many hormones, such as gastrin, cholecystokinin, glucagon, growth hormone, insulin, secretin, pancreatic polypeptide, TSH, and vasoactive intestinal peptide,thus reduce secretion of fluids by the intestine and pancreas) 4. Anti enzyme preparations- inhibits actions of trypsin & kallikrein e.g. Trasylol 1 lac units IV *(extracted from bovine parotid gland) 5. Anti-biotics 6. Peritoneal Lavage
- 27. Indication of Surgical Treatment Uncertain diagnosis Deterioration of clinical condition Correction of associated biliary tract disease Secondary pancreatic infection Local complication like pseudocyst or abscess
- 28. Surgery Ampullary dilatations / sphincteroplasty of ampulla of vater Drainage procedures of the pancreatic duct i. Duvals pancreatojejunostomy ii. Peustow’s longitudinal P-jejunostomy Excisional procedures i. Modified whipple operation ii. Distal subtotal pancreatectomy iii. Total pancreatectomy
- 31. Cysts of pancreas Pseudocyst (80%) – encapsulation of fluid or blood in the lesser sac of peritoneum. True cyst (20%) i. Congenital = single or multiple, simple , fibrocystic disease dermoid cyst i. Acquired =1. retention cyst, 2. hydatid cyst, 3. neoplastic cyst
- 33. Clinical feature Epigastric swelling, upper abdominal pain, anorexia , vomiting . Investigations Sr.amylase , straight Xray, barium meal xray, USG, Complications 1. Infection leading to abscess 2. Rupture 3. Haemorrhage Treatment 1. Conservative & 2. Surgical INTERNAL DRAINAGE = cystojejunostomy, cystogastrostomy, cystoduodenostomy Excision of pseudocyst EXTERNAL DRAINAGE
- 34. Treatment