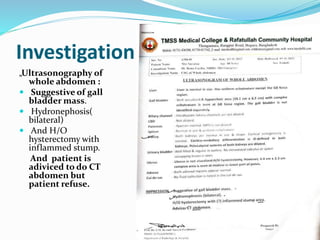
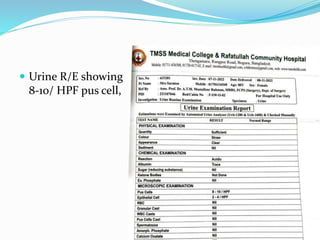
Mrs. Suraton, an 80-year-old widow, presented with a 4-month history of right upper quadrant pain and a 3-month history of weight loss and loss of appetite. Examination revealed a 4x3 cm hard lump in her right hypochondrium. Ultrasound and blood tests suggested gallbladder cancer with elevated CEA and CA 19-9 levels. She was diagnosed with gallbladder carcinoma. Treatment would involve palliative care like stenting for jaundice relief, as the cancer was advanced and unresectable. Her prognosis was poor with a 5-year survival rate of less than 5%.


















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

















