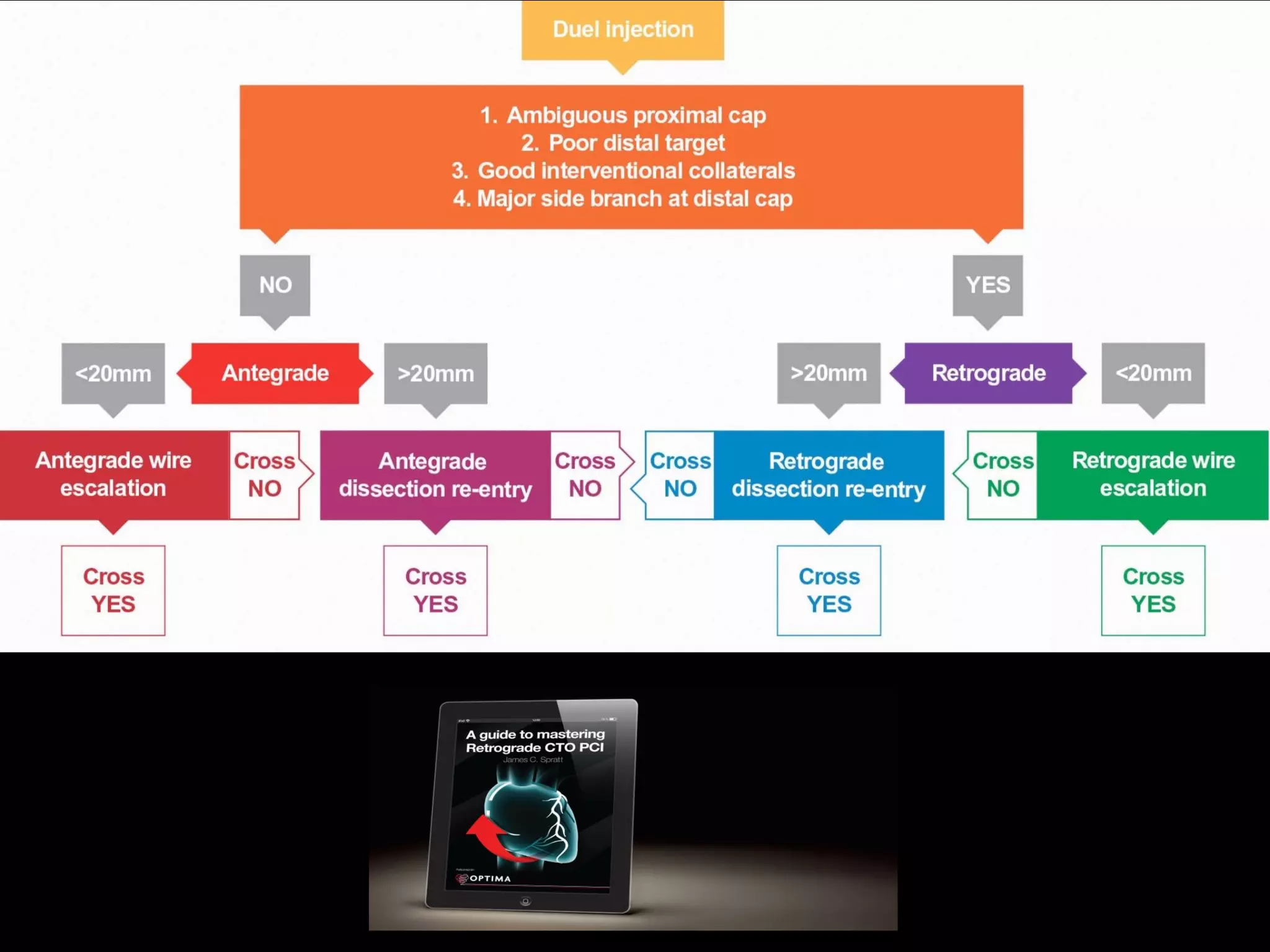
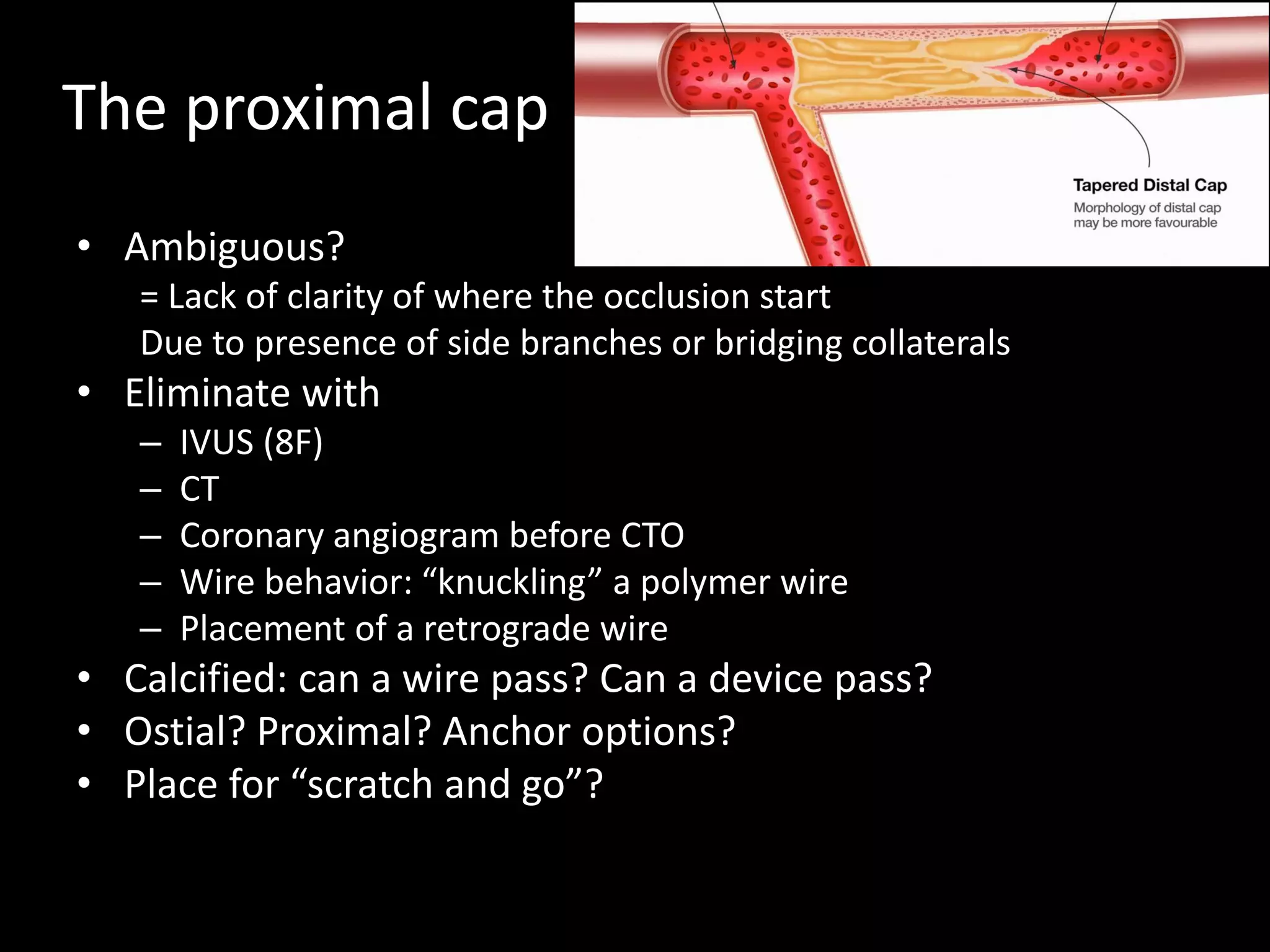
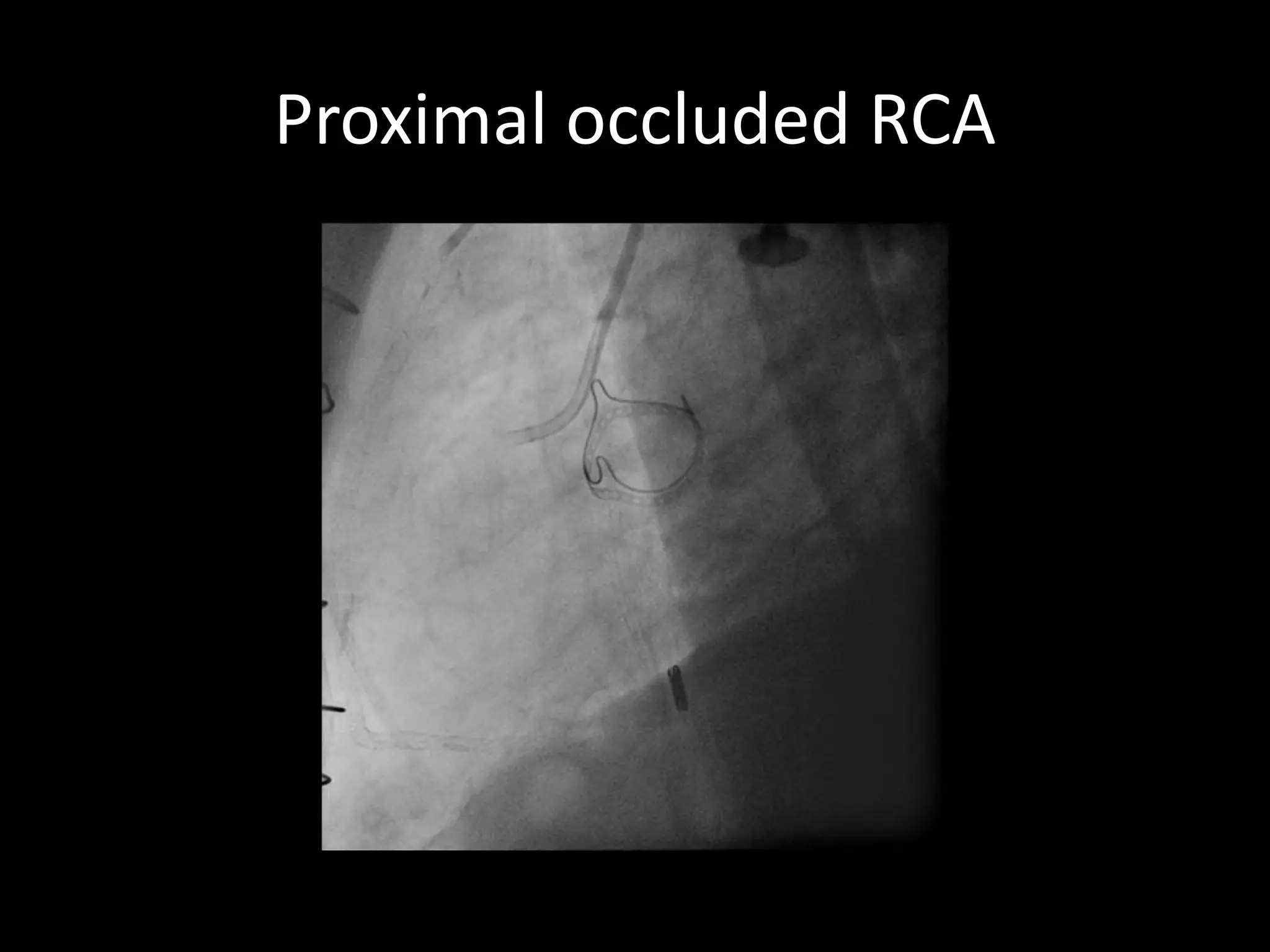
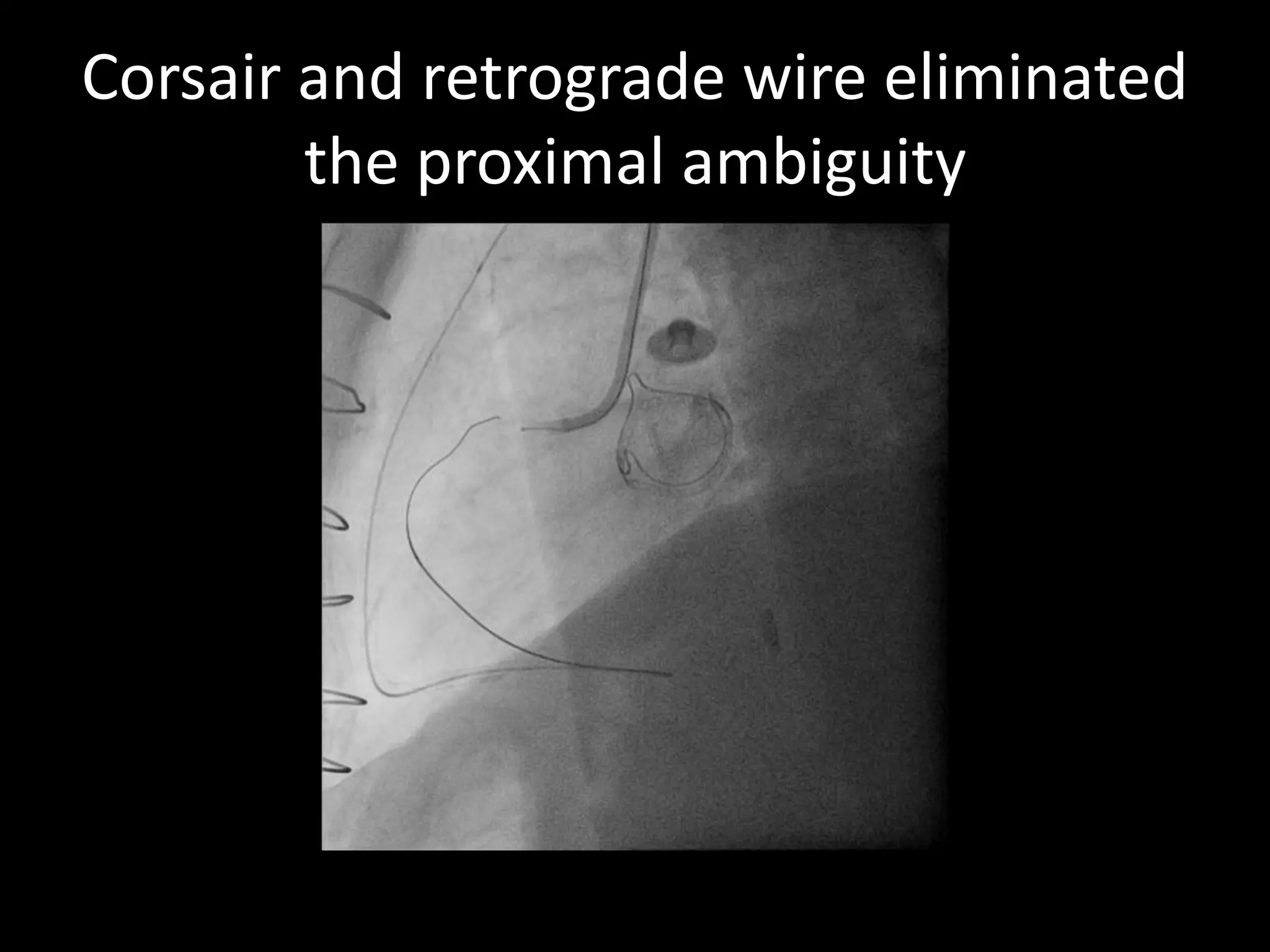
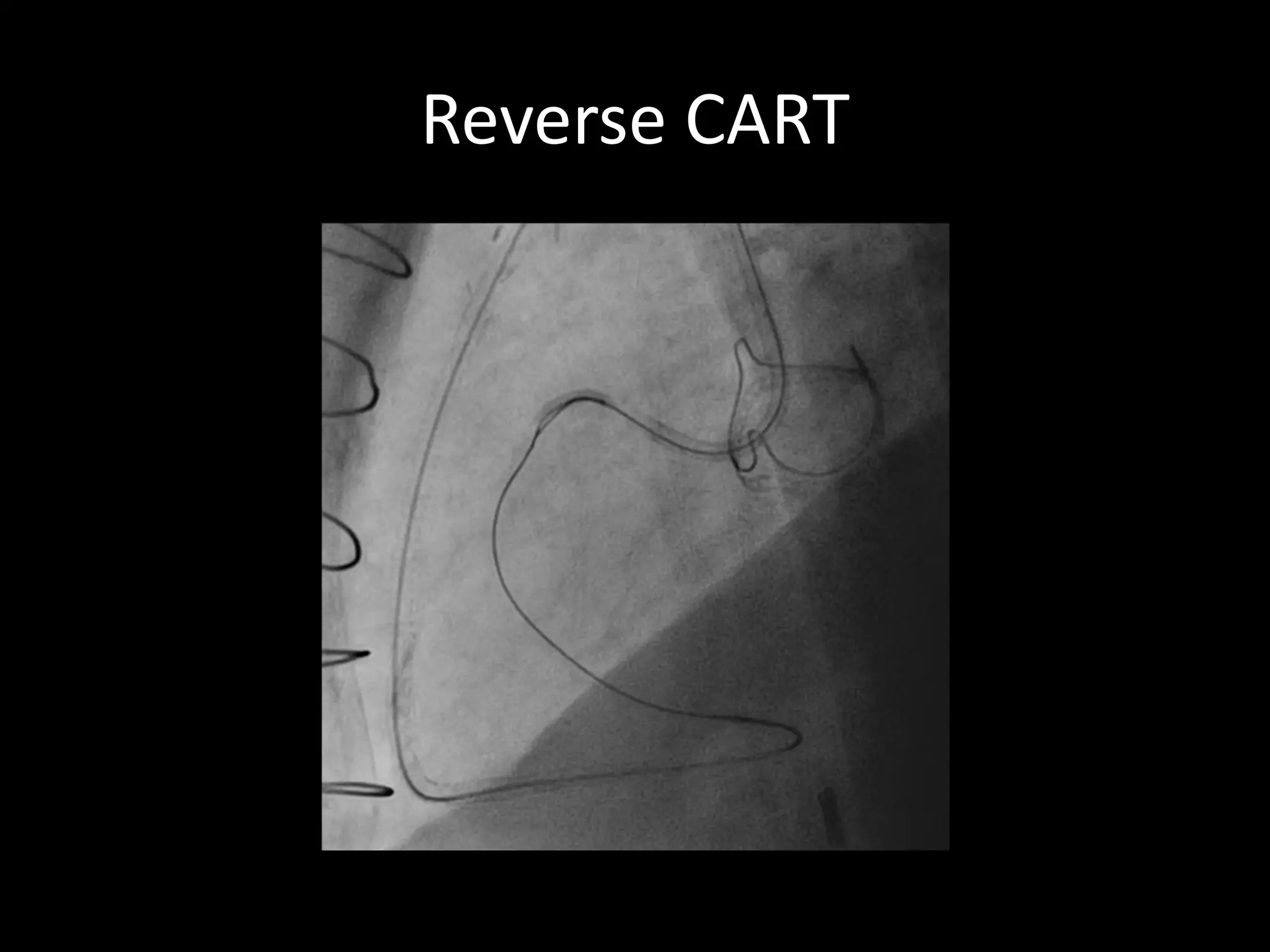
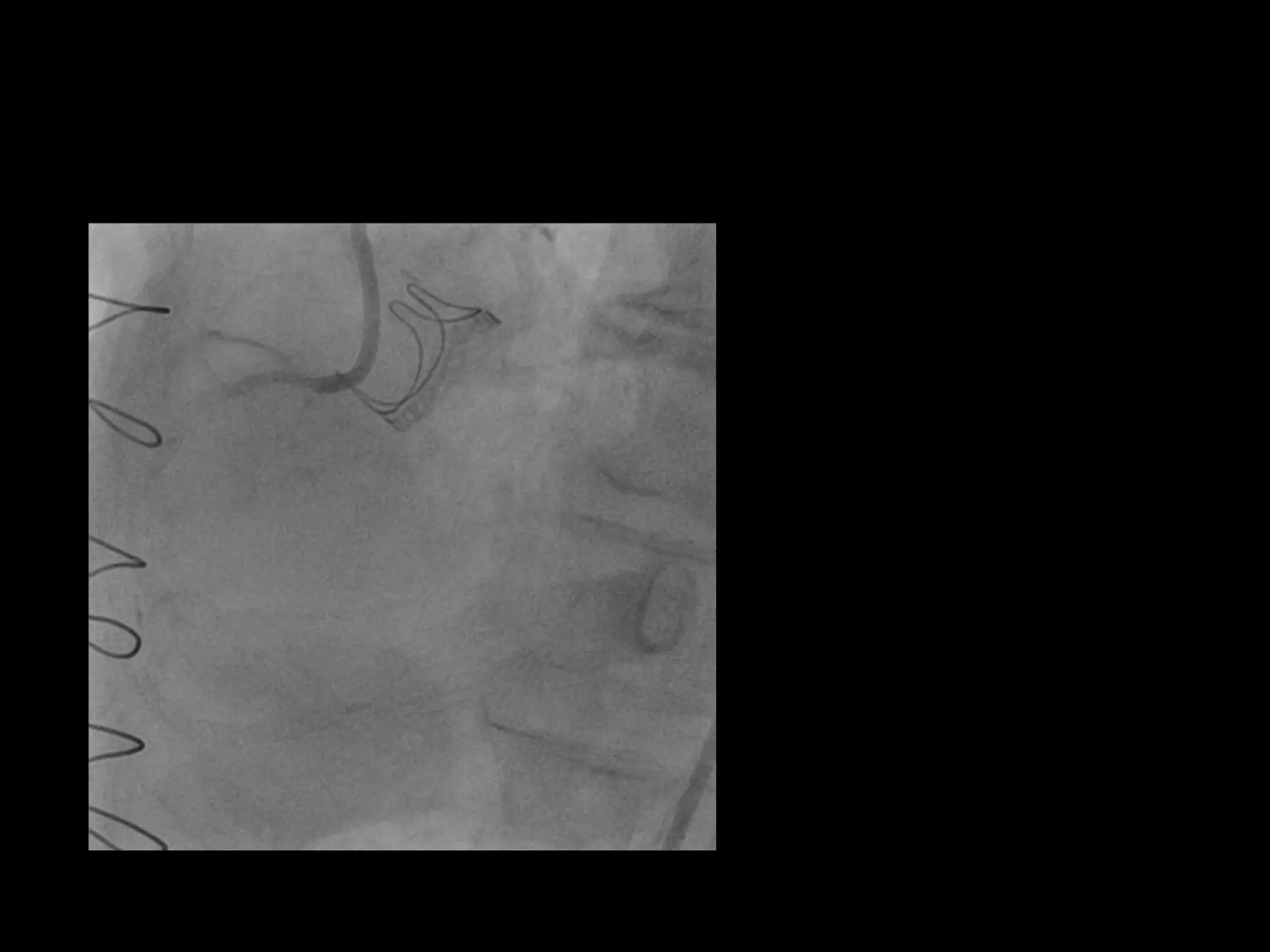
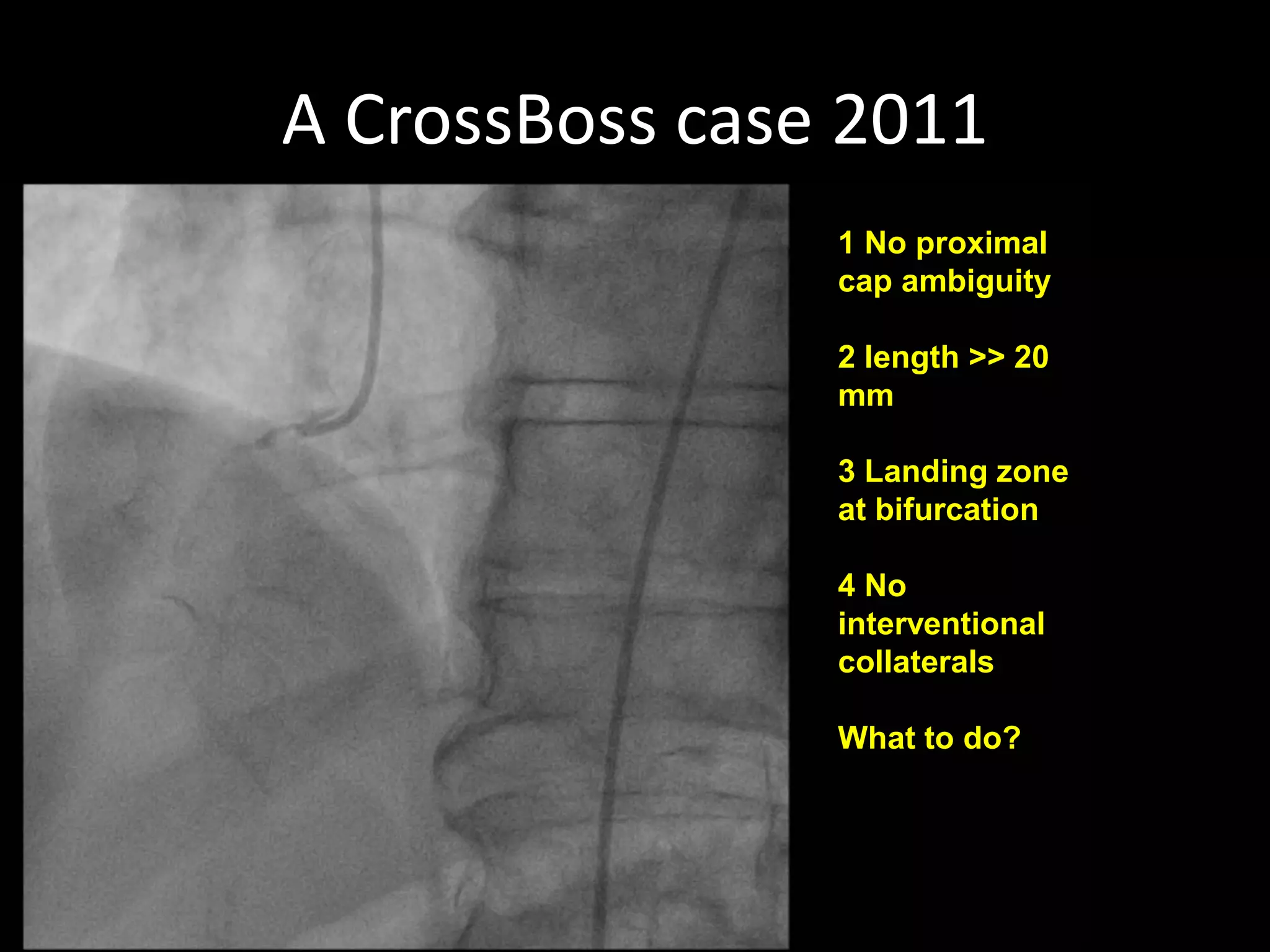
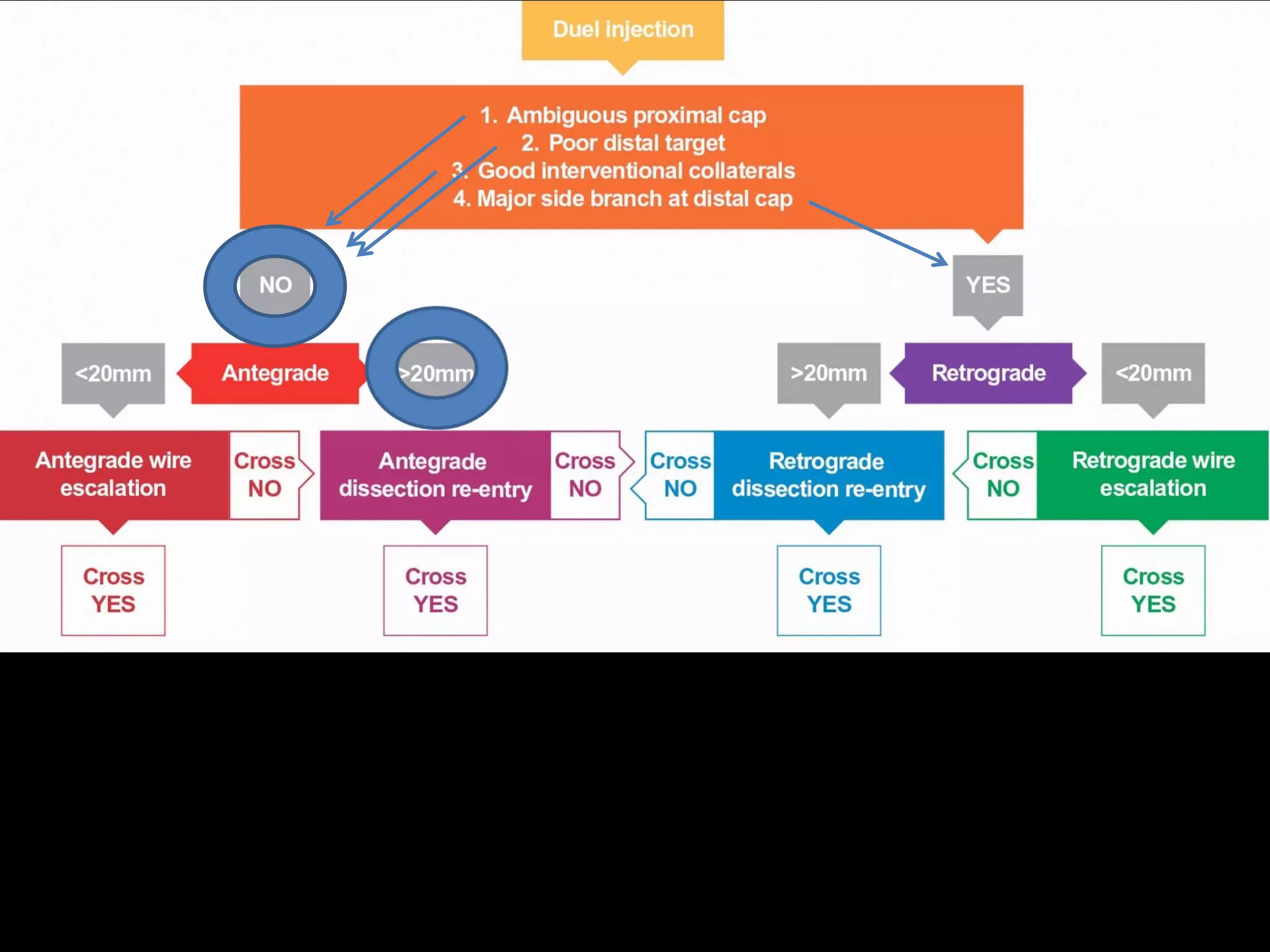
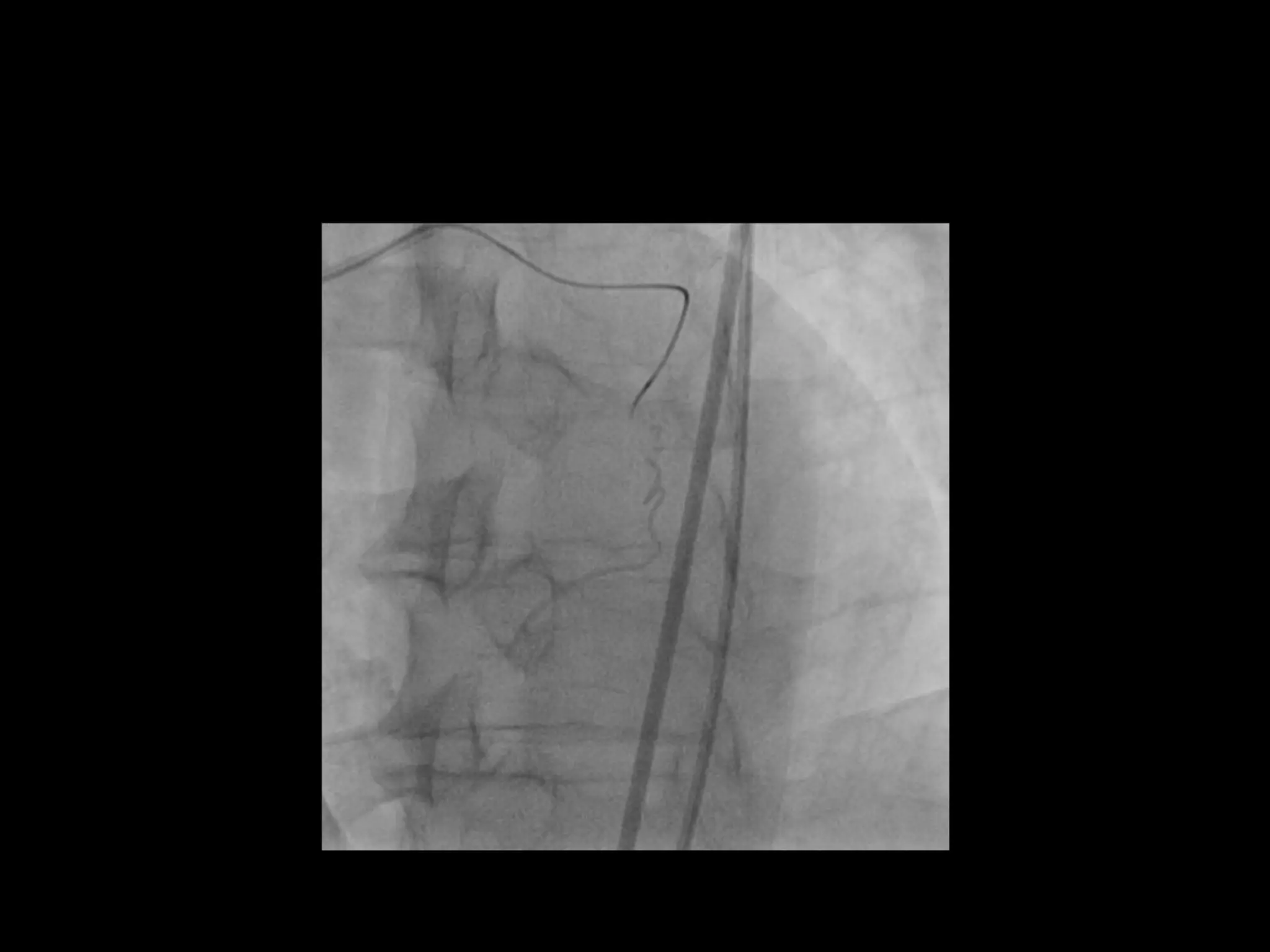
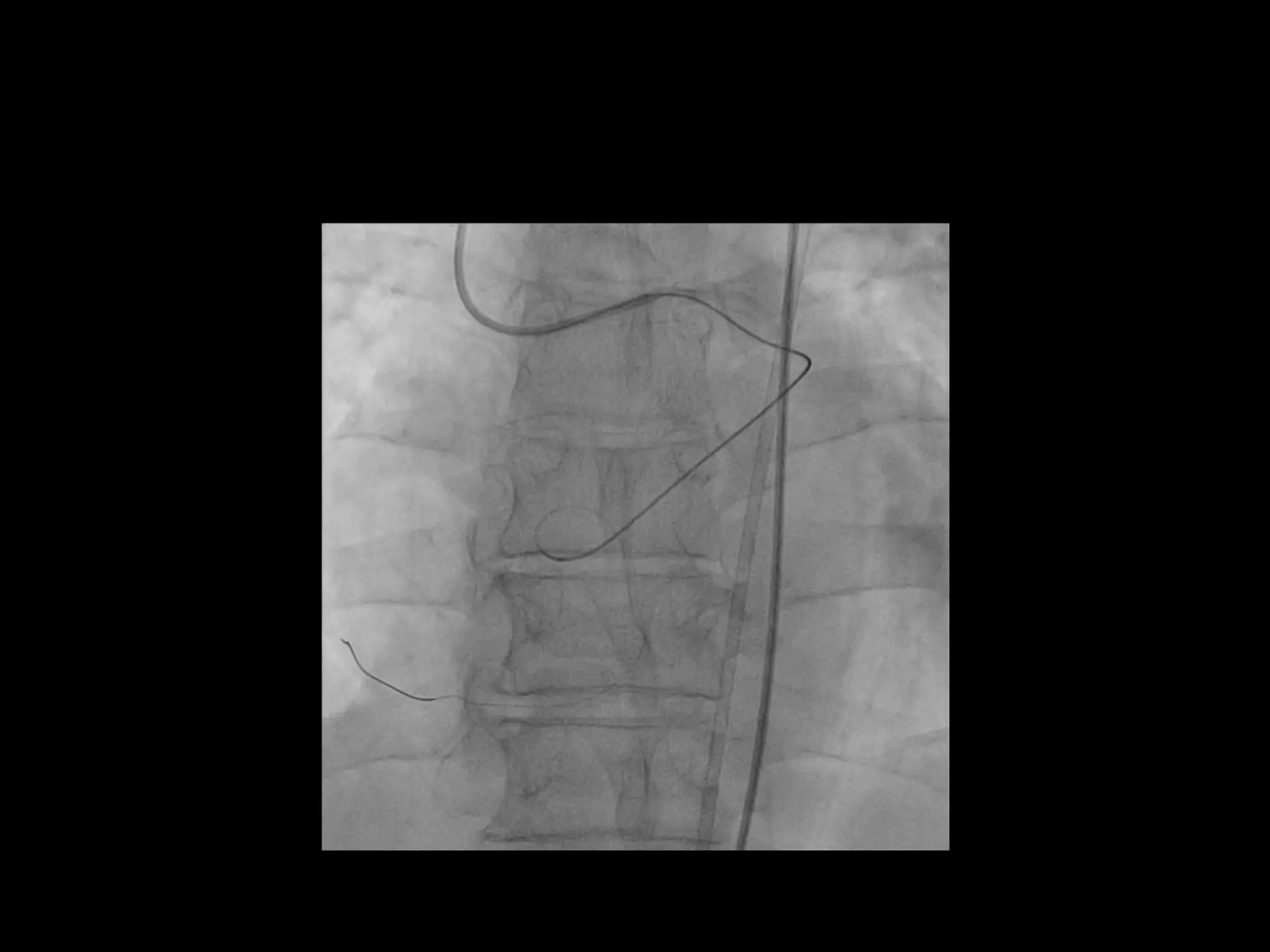
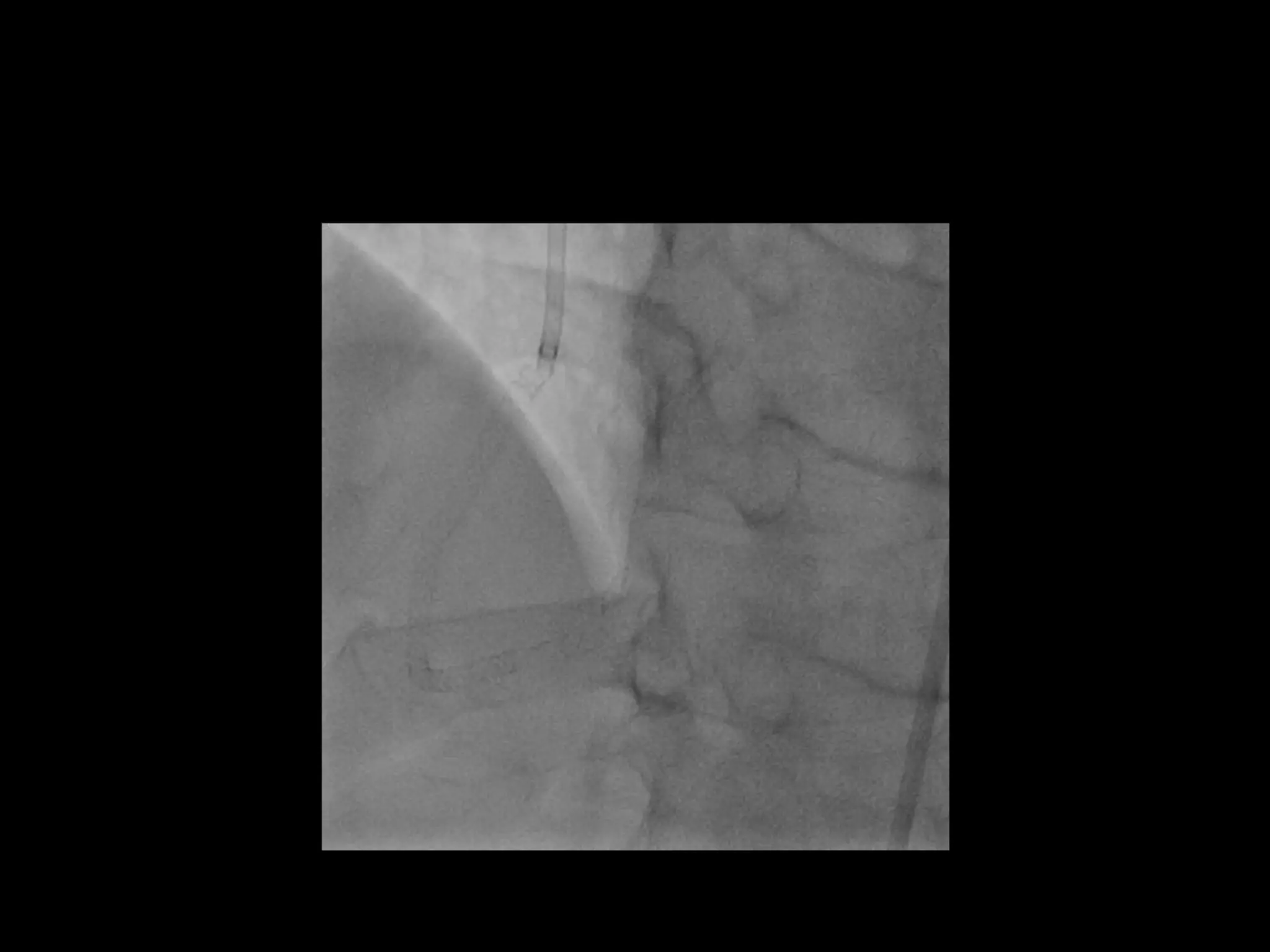
This document provides guidance on evaluating the feasibility of percutaneous coronary intervention (PCI) for a chronic total occlusion (CTO). Key factors to consider include: the patient's tolerance for a long procedure, contrast load, and radiation exposure; the CTO's proximal cap ambiguity, length, distal landing zone, and presence of interventional collaterals; and ensuring good quality angiography. With adequate planning and use of appropriate CTO techniques, feasibility is nearly always present for symptomatic patients. Success rates of CTO-PCI are reported to be 94% when using a planned approach.




























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















