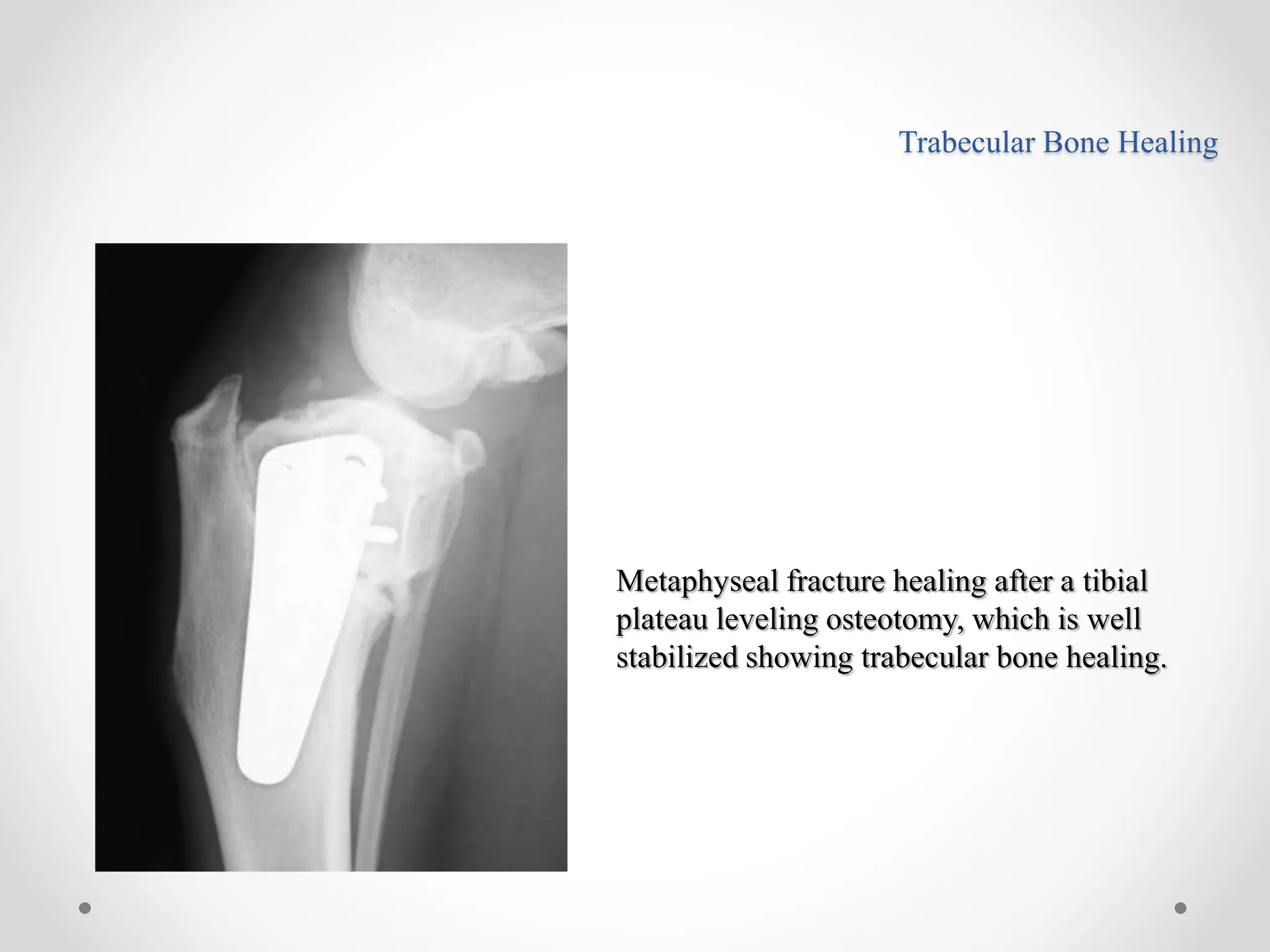
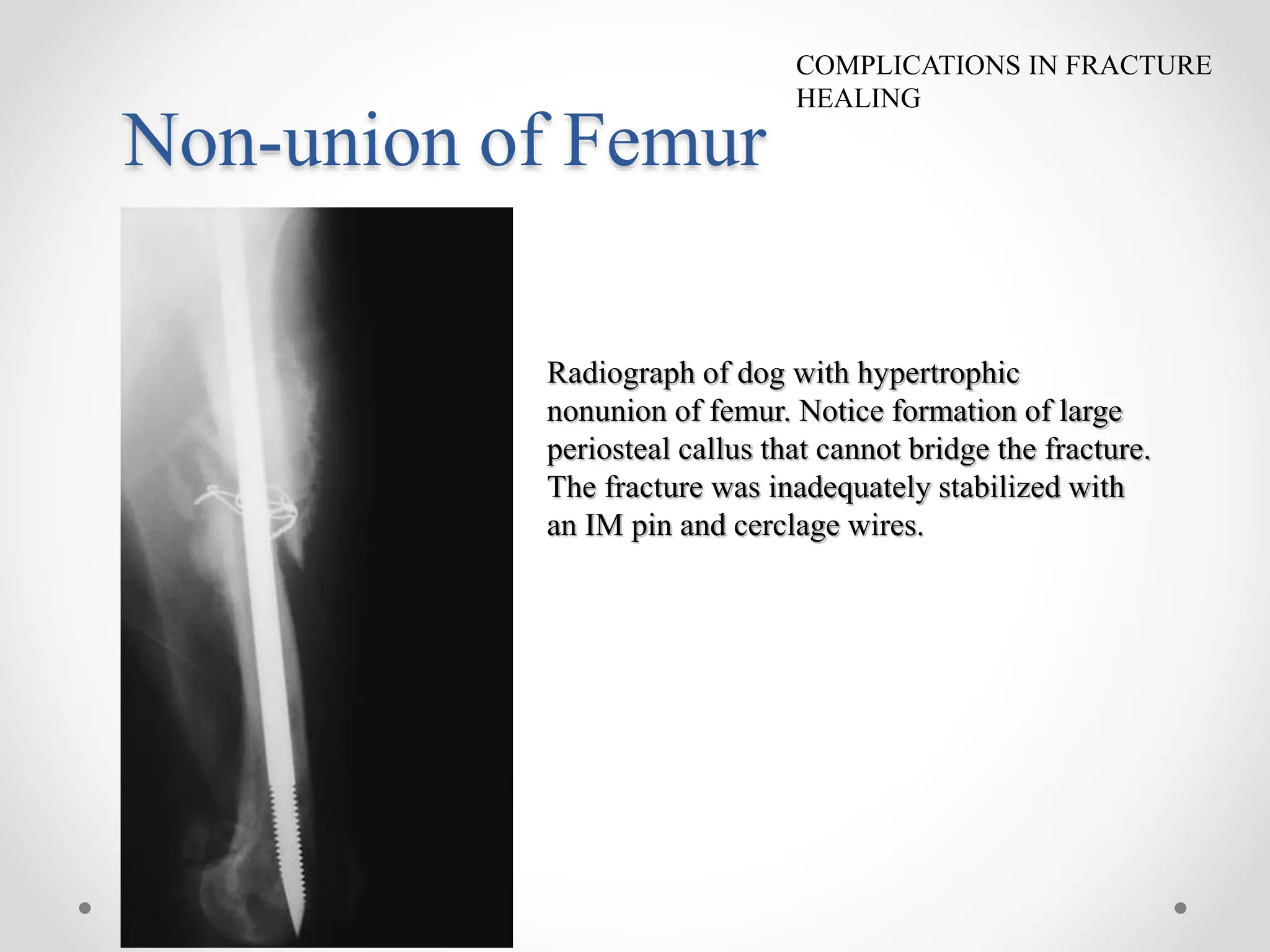
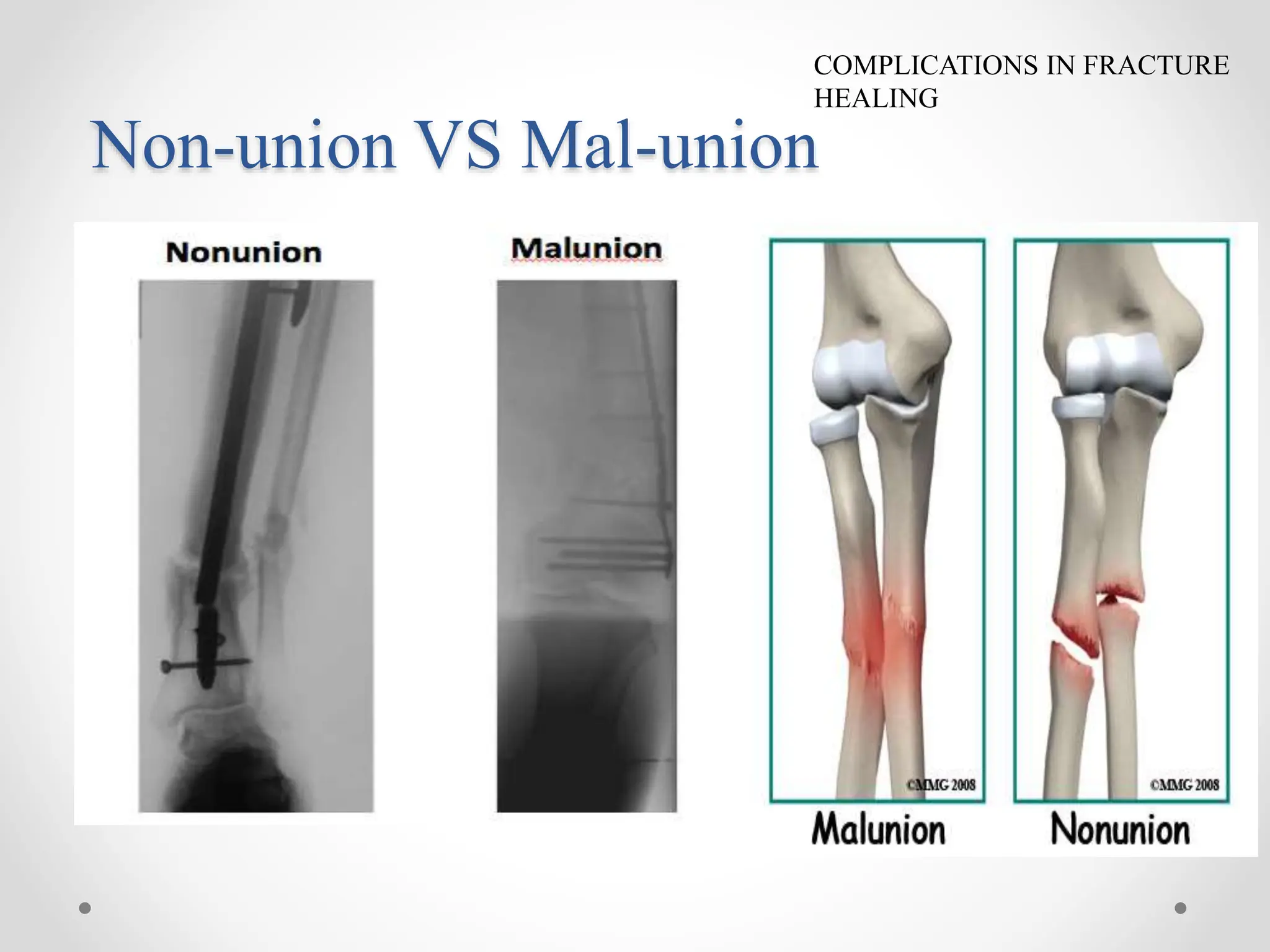
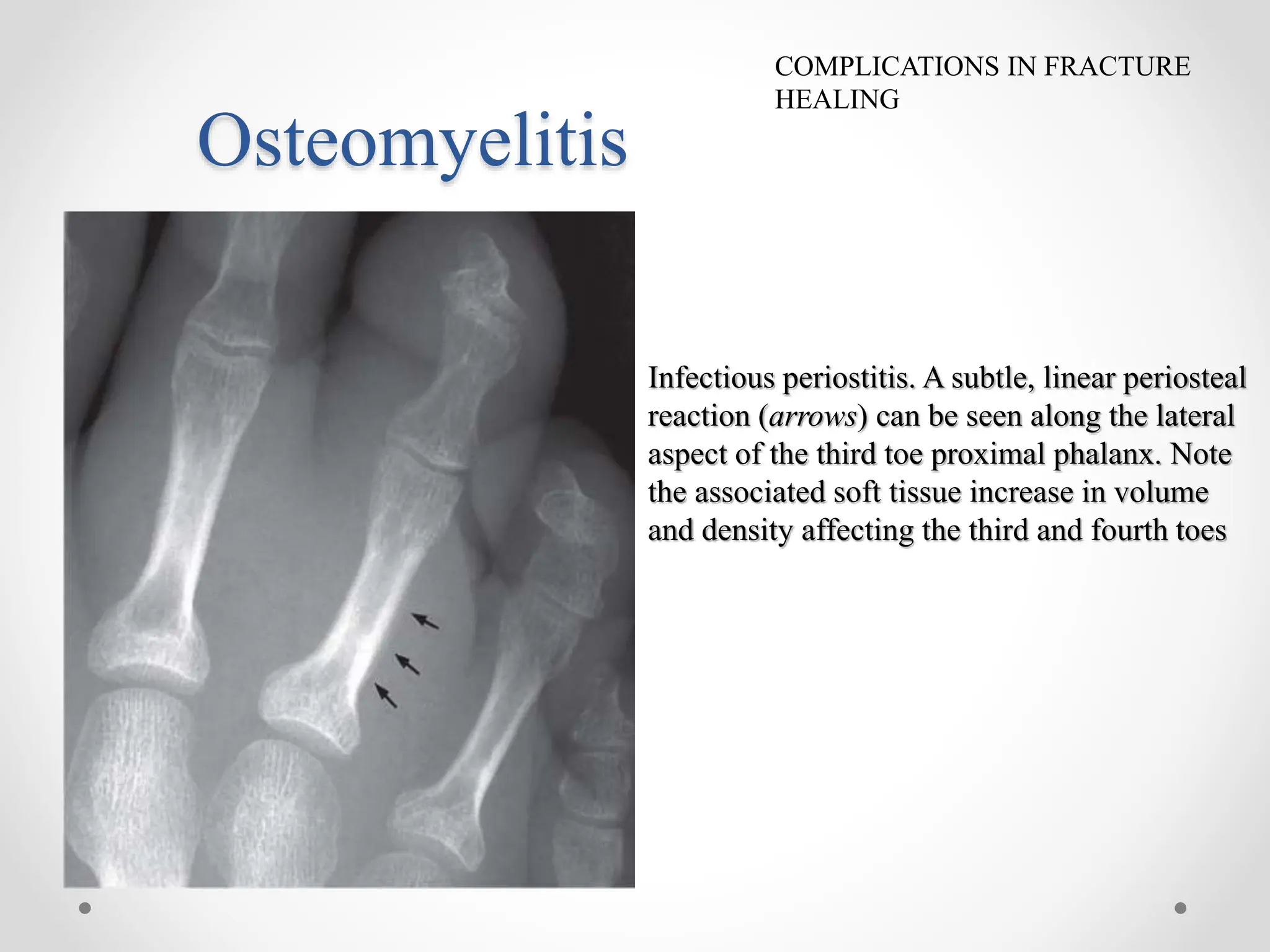
The document discusses the processes and phases of fracture healing, including the reactive, reparative, and remodeling phases, and highlights the impact of biological and mechanical factors on healing. Complications such as delayed union, non-union, osteomyelitis, and mal-union are examined, along with various factors that promote effective fracture healing, including hormones, nutrition, and immobilization. Suggested readings are provided for further exploration of fracture management and healing mechanisms in veterinary practice.













































![2 FRACTURE HEALING reloaded [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/2fracturehealingreloadedautosaved-250810162739-94b56093-thumbnail.jpg?width=640&height=640&fit=bounds)


























