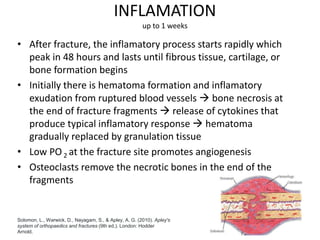
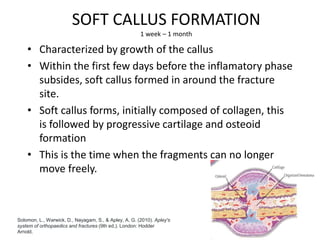
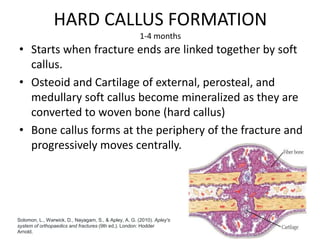
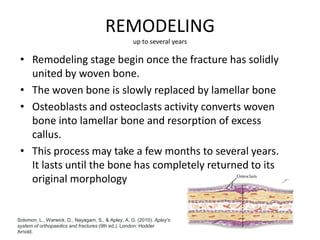
Fracture healing occurs through either primary or secondary bone healing. Primary healing involves direct bone formation without callus and requires perfect stability, while secondary healing involves callus formation over 4 stages - inflammation, soft callus formation, hard callus formation, and remodeling. Several internal and external factors can influence fracture healing, including blood supply, stability, bone stimulators, COX-2 levels, patient diet, diabetes, nicotine use, medications, and health conditions.








![2 FRACTURE HEALING reloaded [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/2fracturehealingreloadedautosaved-250810162739-94b56093-thumbnail.jpg?width=640&height=640&fit=bounds)













![Fracture Healing (Dr Arinze) [Autosaved].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/fracturehealingdrarinzeautosaved-230520154407-0e798837-thumbnail.jpg?width=640&height=640&fit=bounds)

























