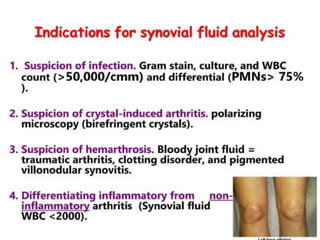
Index
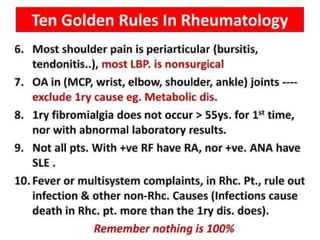
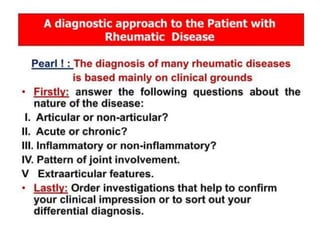
* Introduction anddescribing aim and objectives
* Chief compliant
* History of presenting illness
* Past medical and surgical history
* Drug history
* Social history
* Family history
* Systemic inquiry
* How to summarize a case to other doctors,
* Difficult situations
3.
Loading…
Importance of HistoryTaking
* Diagnosing the patient, or at least clues towards the diagnosis.
* There is 70% chance of diagnosing a patient based on hx alone,
* Know your patient,
* Gain confidence and respect,
4.
The art ofa successful hx
taking
* Introduce yourself,
* Listen to the patient,
* Respect the patient
5.
Loading…
General Approach
* Introduceyourself
* الكنية
* Deal with the patient in a friendly relaxed way
* Confidentiality and respect patient privacy.
* Try to see things from patient point of view. Understand patient
underneath mental status, anxiety, irritation or depression.
* Always be in a relaxed, respectful posture,
* Questioning: simple/clear/avoid medical.
* Summarizing.
* Patients concerns.
Personal history
* Name,
*Age,
* Address,
* Sex,
* Ethnicity,
* Occupation,
* Religion,
* Marital status,
9.
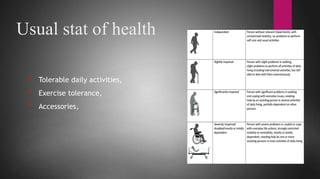
Complete History Taking
*Usual stat of health?
* Chief complaint
* History of present illness
* Past medical /surgical history
* Systemic review
* Family history
* Drug /blood transfusion history
* Social history
* Gyn/ob history.
Chief Complaint
* CC+ duration.
* The main reason push the pt. to seek for visiting a physician or for help
* Usually a single symptom, occasionally more than one complaints eg: chest
pain, palpitation, shortness of breath, ankle swelling etc
* The patient describe the problem in their own words.
* It should be recorded in pt’s own words.
* What brings your here? How can I help you? What seems to be the problem?
Since when you’ve been tired?
13.
History of PresentIllness
* Analysis of the chief complaint,
* In any symptom, always ask about
-> Onset, course, duration, aggravating factors, relieving factors.
* Each symptom has its own analysis,
-> Pain
-> Fever,
-> Vomiting,
-> SOB,
ETC….
14.
Pain ( SOCRATES)
S_ite:Somatic (Localised) Vs Visceral ( Diffuse)
O_nset : Speed of onset , abrupt or gradual.
C_haracter
– burning sharp, stabbing, crushing; also explain depth of pain – superficial or deep.
R_adiation: where moved to
A_ssociated symptoms
T_iming – mode of onset (abrupt or gradual), progression (continuous or
intermittent – if intermittent ask frequency/ nature.)
E_xacerbating and Relieving factors – any activities position , drug.
S_everity – how it affects daily work/physical activities. Wakes him up at night,
cannot sleep/do any work.
Past medical andsurgical history
* If relevant, should be mentioned in the beginning of the history
presentation,
* Components of each disease: Disease, how and when
diagnosed, treatment, controlled or not, compliance to meds,
known complications of the disease,
* Components of each surgery: when done?, elective or
emergency, possible complications of the surgery,
* These questions will elicit the key information in most patients:
* What illnesses have you seen a doctor about in the past?
* Have you been in hospital before or attended a clinic?
17.
* Have youhad any operations?
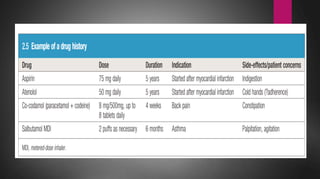
Drug history
* Always use generic name or put trade name in brackets with dosage, timing
&how long, ( morning or at night) ,( Before or after food )
* Example: Pantoprazole ( Pantovir) 40 mg OD PO, started one week ago,
before breakfast.
* Note: do not forget to mention: OTC/Vitamins/Traditional /Herbal medicine
& alternative medicine as cupping or cattery or acupuncture
19.
Family history
* Startwith open questions, such as ‘Are there any illnesses
that run in your family?’
* Follow up the presenting symptoms with a question like
‘Have any of your family had heart trouble
20.
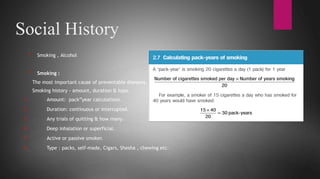
Social History
* Smoking, Alcohol
* Smoking :
The most important cause of preventable diseases.
Smoking history - amount, duration & type.
1. Amount: pack”year calculations.
2. Duration: continuous or interrupted.
3. Any trials of quitting & how many.
4. Deep inhalation or superficial.
5. Active or passive smoker.
6. Type : packs, self-made, Cigars, Shesha , chewing etc.
21.
Occupational history andhome
environment
* Work profoundly influences health. Unemployment is associated
with increased morbidity and mortality while some occupations
are associated with particular illnesses
* Ask all patients about their occupation. Clarify what the person
does at work, especially about any chemical or dust exposure.
If the patient has worked with harmful materials (such asbestos
or stone dust),
22.
home environment
Symptoms thatimprove over the weekend or
during holidays suggest an occupational disorder.
* In the home environment, hobbies may also be
relevant: for example, psittacosis pneumonia or
hypersensitivity pneumonitis in those who keep
birds, or asthma in cat or rodent owners.
System Review (SR)
*This is a guide not to miss anything. Any significant finding should be
moved to HPC or PMH depending upon where you think it belongs.
* Do not forget to ask associated symptoms of PC with the System
involved When giving verbal reports, say no significant finding on systems
review to show you did it.
* However when writing up patient notes, you should record the systems
review so that the relieving doctors know what system you covered
25.
System Review
General
* Weakness
*Fatigue
* Anorexia
* Change of weight
* Fever/chills
* Lumps
* Night sweats
Cardiovascular
* Chest pain
* Paroxysmal Nocturnal Dyspnoea
* Orthopnoea
* Short Of Breath(SOB)
* Cough/sputum (pinkish/frank blood)
* Swelling of ankle(SOA)
* Palpitations
System Review
Urinary SystemNervous System
Urinary System
* Frequency
* Dysuria
* Urgency/strangury
* Hesitancy
* Terminal dribbling
* Nocturia
* Back/loin pain
* Incontinence
Nervous System
* Visual/Smell/Taste/Hearing/Speech
problem
* Head ache
* Fits/Faints/Black outs/loss of
consciousness(LOC)
* Muscle weakness/numbness/paralysis
* Abnormal sensation
* Tremor
* Change of behaviour or psyche.
28.
* Character ofurine:color/ amount (polyuria)
System Review
Genital system
* Pain/ discomfort/ itching
* Discharge
* Unusual bleeding
* Sexual history
* Menstrual history – menarche/ LMP/ duration
& amount of cycle/ Contraception
* Obstetric history – Para/ gravida/abortion
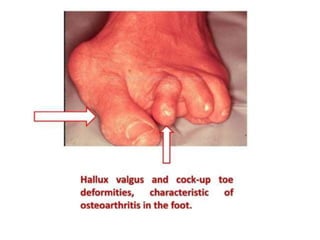
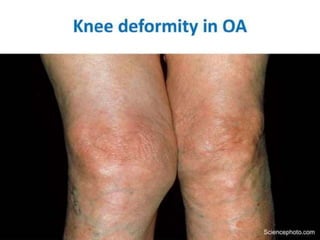
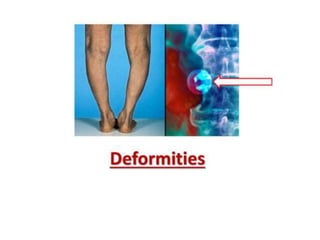
Musculoskeletal System
* Pain – muscle, bone, joint
* Swelling
* Weakness/movement
* Deformities
* Gait
29.
Loading…
Closing the interview
*Using simple language, briefly explain your interpretation of the
patient’s history and outline the likely possibilities.
* Be sensitive to their concerns and body language.
* Ask the patient if they already have ideas and concerns about the
diagnosis , so these may be addressed directly.
* Always give the patient a final opportunity to raise additional concerns
(‘Is there anything else you would like to ask?’).
* Make sure patients are involved in any decisions by suggesting possible
actions and encouraging them to contribute their thoughts.
* This way, you should be able to negotiate an agreed plan for further
investigation and follow-up.
* Tell them that you will communicate this plan to other professionals
involved in their care
Patients with communicationdifficulties
* If your patient does not speak your language, arrange to have an
interpreter, remembering to address the patient and not the interpreter.
* If your patient has hearing or speech difficulties such as dysphasia or
dysarthria, consider the following:
* • Write things down for your patient if they can read.
* • Involve someone who is used to communicating with your patient.
* • Seek a sign language interpreter for a deaf patient skilled in sign
language.
32.
Patients with cognitive
difficulties
*Be alert for early signs of dementia. Inconsistent or hesitant
responses from the patient should always prompt you to suspect
and check for memory difficulties.
* If you do suspect this, assess the patient using a cognitive rating
scale
* You may have to rely on a history from relatives or carers
33.
Sensitive situations
* Doctorssometimes need to ask personal or sensitive questions and
examine intimate parts.
* If you are talking to a patient who may be suffering from sexual
dysfunction, sexual abuse or sexually transmitted disease, broach
the subject sensitively.
* Indicate that you are going to ask questions in this area and make
sure the conversation is entirely private.
34.
Emotional or angrypatients
* Ill people feel vulnerable and may become angry and frustrated about
how they feel or about their treatment.
* Staying calm and exploring the reasons for their emotion often defuses
the situation.
* Although their behaviour may be challenging, never respond with anger
or irritation and resist passing comment on a patient’s account of prior
management.
* Recognise that your patient is upset, show empathy and understanding,
and ask them to explain why
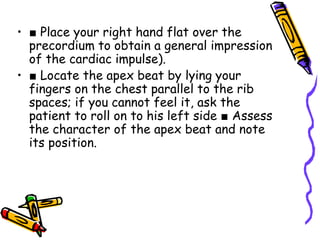
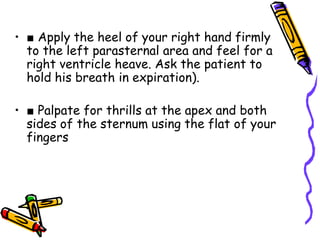
PREPARING FOR PHYSICALEXAMINATION
• The physical examination begins as soon as you see the patient.
• Always introduce yourself to the patient, shake hands and seek
permission to conduct the consultation.
• Relevant equipment
• Hand hygiene .
• Privacy , Chaperone.
• Warm room and well lit.
• Adjust the height of the examination couch or bed.
• Exposure
INITIAL OBSERVATIONS
• Firstimpression , Stable / Unstable
• Assessment of vital signs: pulse, BP, RR , oxygen saturations,
temperature, conscious level and pain score
• Do they look generally well or unwell? What is their
demeanour?
• Notice the patient’s attire. Are they dressed appropriately?
• Look for clues to the patient’s underlying medical condition
(subcutaneous insulin pump ,oxygen cylinder ,hearing aid,
inhaler device, and note any walking aid or wheelchair )
44.
Scars from deliberateself-harm
(cutting).
The linear marks of intravenous injection
at the right antecubital fossa.
45.
Loading…
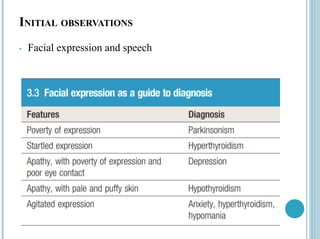
INITIAL OBSERVATIONS
Gait andposture :
• How they rise from a chair and walk towards you. Are they using a
walking aid? Is the gait normal ?
• Hemiplegic gait after stroke
• Ataxic gait of cerebellar disease
• The marche à petits pas (‘walk of little steps’) gait in a patient with
diffuse cerebrovascular disease or Parkinsonism
• Tremor ,dystonia ,or chorea
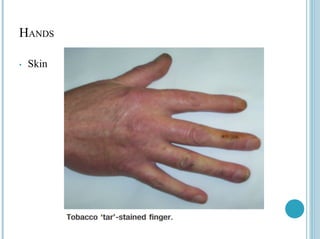
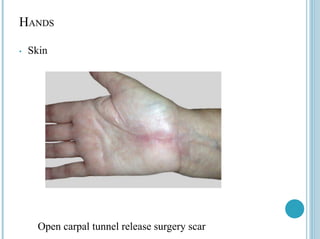
HANDS
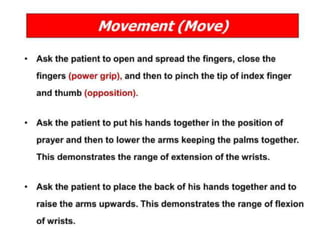
• Examination sequence: Look , Feel , Move
• Inspect the dorsal and then the palmar aspects of both
hands
• Note changes in the :
➢ Skin
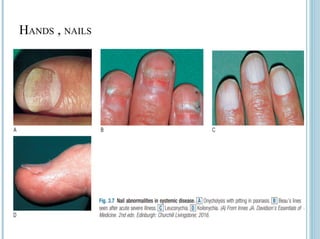
➢ Nails
➢ Soft tissue ( evidence of muscle wasting )
➢ Tendons
➢ Joints
• Assess temperature
• Assess pulse
48.
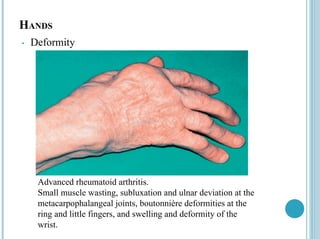
HANDS
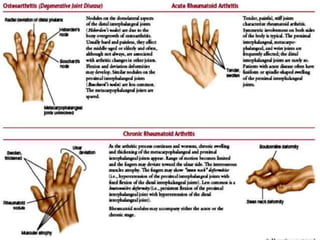
• Deformity
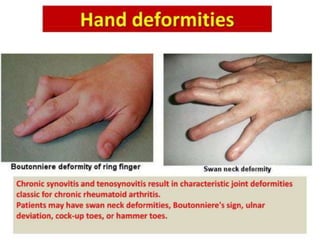
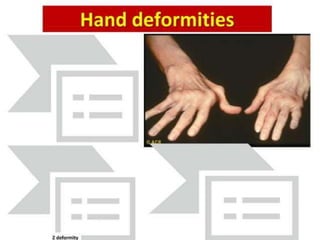
Advanced rheumatoidarthritis.
Small muscle wasting, subluxation and ulnar deviation at the
metacarpophalangeal joints, boutonnière deformities at the
ring and little fingers, and swelling and deformity of the
wrist.
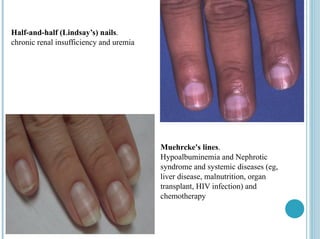
Half-and-half (Lindsay’s) nails.
chronicrenal insufficiency and uremia
Muehrcke's lines.
Hypoalbuminemia and Nephrotic
syndrome and systemic diseases (eg,
liver disease, malnutrition, organ
transplant, HIV infection) and
chemotherapy
SKIN
• The skincan provide insights into present and past medical disorders, as well
as information about the patient’s social or mental status.
Skin colour is determined by :
• Pigments in the skin – melanin, an endogenous brown pigment, and
carotene, an exogenous yellow pigment (mainly derived from ingestion of
carrots and other vegetables)
• The amount of oxyhaemoglobin (red) and deoxyhaemoglobin (blue)
circulating in the dermis.
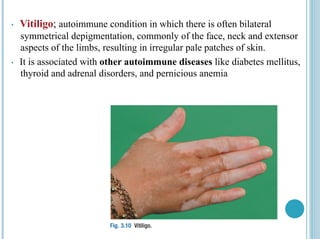
• Vitiligo; autoimmunecondition in which there is often bilateral
symmetrical depigmentation, commonly of the face, neck and extensor
aspects of the limbs, resulting in irregular pale patches of skin.
• It is associated with other autoimmune diseases like diabetes mellitus,
thyroid and adrenal disorders, and pernicious anemia
62.
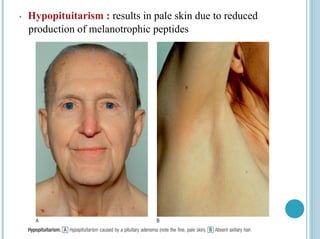
• Hypopituitarism :results in pale skin due to reduced
production of melanotrophic peptides
63.
Loading…
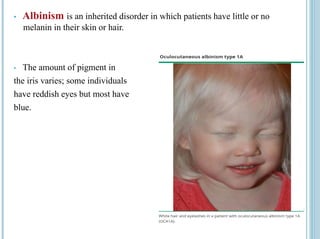
• Albinism isan inherited disorder in which patients have little or no
melanin in their skin or hair.
• The amount of pigment in
the iris varies; some individuals
have reddish eyes but most have
blue.
64.
SKIN
Hyperpigmentation :
• Excessof the pituitary hormone adrenocorticotrophic hormone
(ACTH), as in adrenal insufficiency (Addison’s disease)
• Pregnancy and oral contraceptives may also cause blotchy
hyperpigmentation on the face, known as chloasma, and
pregnancy may increase pigmentation of the areolae, axillae,
genital skin and linea alba (producing a dark line in the midline
of the lower abdomen, called a ‘linea nigra’).
65.
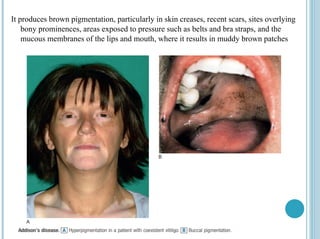
It produces brownpigmentation, particularly in skin creases, recent scars, sites overlying
bony prominences, areas exposed to pressure such as belts and bra straps, and the
mucous membranes of the lips and mouth, where it results in muddy brown patches
66.
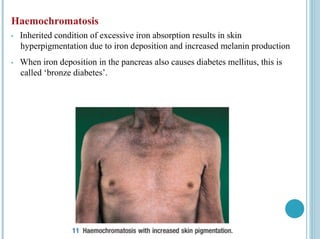
Haemochromatosis
• Inherited conditionof excessive iron absorption results in skin
hyperpigmentation due to iron deposition and increased melanin production
• When iron deposition in the pancreas also causes diabetes mellitus, this is
called ‘bronze diabetes’.
67.
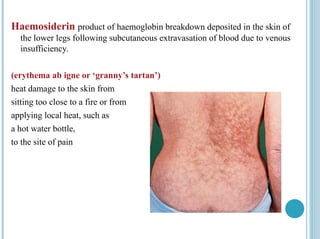
Haemosiderin product ofhaemoglobin breakdown deposited in the skin of
the lower legs following subcutaneous extravasation of blood due to venous
insufficiency.
(erythema ab igne or ‘granny’s tartan’)
heat damage to the skin from
sitting too close to a fire or from
applying local heat, such as
a hot water bottle,
to the site of pain
68.
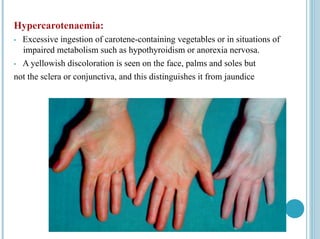
Hypercarotenaemia:
• Excessive ingestionof carotene-containing vegetables or in situations of
impaired metabolism such as hypothyroidism or anorexia nervosa.
• A yellowish discoloration is seen on the face, palms and soles but
not the sclera or conjunctiva, and this distinguishes it from jaundice
69.
• Skin discoloration
•Jaundice
• Pallor
• Facial flushing
• Cyanosis : central and peripheral
70.
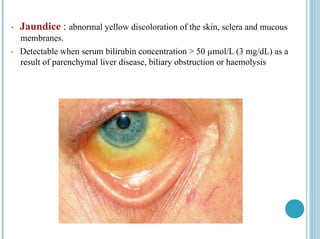
• Jaundice :abnormal yellow discoloration of the skin, sclera and mucous
membranes.
• Detectable when serum bilirubin concentration > 50 µmol/L (3 mg/dL) as a
result of parenchymal liver disease, biliary obstruction or haemolysis
71.
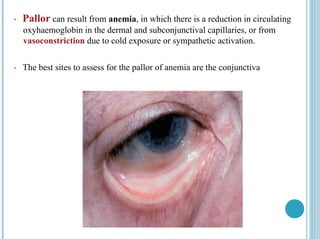
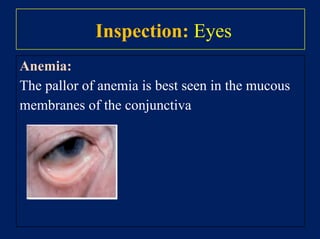
• Pallor canresult from anemia, in which there is a reduction in circulating
oxyhaemoglobin in the dermal and subconjunctival capillaries, or from
vasoconstriction due to cold exposure or sympathetic activation.
• The best sites to assess for the pallor of anemia are the conjunctiva
72.
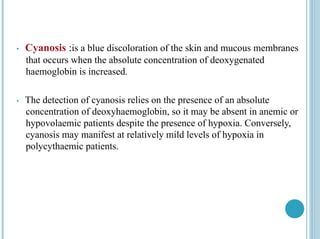
• Cyanosis :isa blue discoloration of the skin and mucous membranes
that occurs when the absolute concentration of deoxygenated
haemoglobin is increased.
• The detection of cyanosis relies on the presence of an absolute
concentration of deoxyhaemoglobin, so it may be absent in anemic or
hypovolaemic patients despite the presence of hypoxia. Conversely,
cyanosis may manifest at relatively mild levels of hypoxia in
polycythaemic patients.
73.
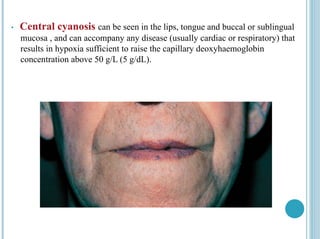
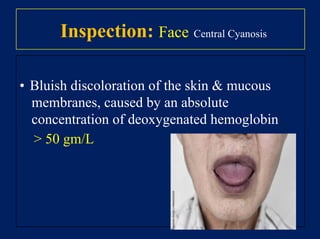
• Central cyanosiscan be seen in the lips, tongue and buccal or sublingual
mucosa , and can accompany any disease (usually cardiac or respiratory) that
results in hypoxia sufficient to raise the capillary deoxyhaemoglobin
concentration above 50 g/L (5 g/dL).
74.
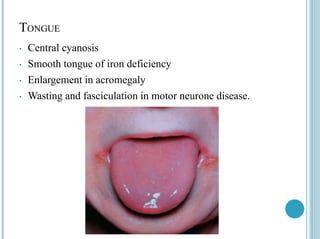
TONGUE
• Central cyanosis
•Smooth tongue of iron deficiency
• Enlargement in acromegaly
• Wasting and fasciculation in motor neurone disease.
75.
ODOURS
Odours can provideclues to a patient’s social or behavioural
habits :
• The smell of alcohol or tobacco
• Stale urine and anaerobic skin infections produce distinctive smells.
• Halitosis (bad breath) : poor dental hygiene, gingivitis, stomatitis, atrophic
rhinitis, tumours of the nasal passages or suppurative lung conditions such
as lung abscess or bronchiectasis.
• ketones: a sweet smell (like nail varnish remover) due to acetone in
diabetic ketoacidosis or starvation.
• Fetor hepaticus: the stale, ‘mousy’ smell of the volatile amine
dimethylsulphide in patients with liver failure.
76.
BODY HABITUS ANDNUTRITION
• Weight
• Obesity
• Weight loss
• Stature
• Short stature
• Tall stature
77.
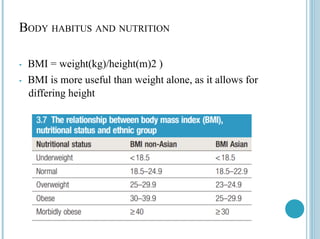
BODY HABITUS ANDNUTRITION
• BMI = weight(kg)/height(m)2 )
• BMI is more useful than weight alone, as it allows for
differing height
79.
Neck Exam
Ahmed Al-Jodi, MD
Surgical Oncologist, KHCC , AB.
Head of Surgical oncology Unit , HGH
Faculty of Medicine/ Al-Quds University
80.
Neck swellings
• Pt'sage, Clinical Course, Site & Consistency (solid/ cystic).
• It should be noted that the most common swellings of the neck are
swellings of LN s & thyroid, followed by those of the salivary glands.
81.
Loading…
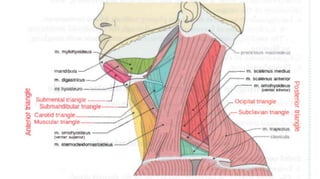
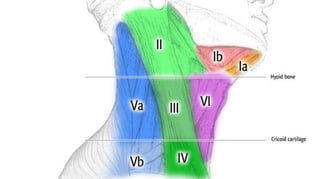
Anatomical Divisions ofthe Neck
● Triangles:
● Posterior.
● Anterior
● Further divided into:
Submandibular, Carotid & Muscular triangles.
● Compartments:
● The pre-vertebral fascia divides the neck into 2 compartments:
• 1. The muscular compartment -----posteriorly. ·
• 2. The visceral compartment --------Anteriorly.
1-Histrory
• Personal data:
• Age :
child ….. Mumps / adenitis
middle age ( around 40 ) …. Pleomorphic adenoma / thyroid.
old age ( > 60 ) …. Lymphoma or neck cancers.
• Sex :
neck swellings in general male > female except thyroid swelling s
• Duration :
•short ….. inflamation
• long ….. Neoplasm / congenital
• Site :
• uni or bi lateral
• Size : in cm .
• Pain : is it painfull or painless?
88.
•Pain :
• Onset
•Course : constant ( abscess ) … intermittent ( stone )
• Duration
• Character : throbbing ( abcess) … dull aching ( stone )
• Site : according to the triangle
• Radiation : to which part of the neck … shoulder / to the head
• Aggravating factors .. ( eating …sour food )
• Head andneck :thyroid and lymph nodes ( should be examined )
• Skin and extremities : oedema / skin changes
• Chest :
area of dullness : malignancy
symptoms of mediastinal L.N: 5D’s
Dilated veins …..Dull sternum…..Dyspnea…. Dysphagia …Despein
sign ( bronchial breathing below t4 )
94.
• Abdominal exam:
• Spleno-megaly
• Para-aortic lymph nodes ( may be felt around the umbilicus ) in thin
patients
• DRE : why … Virchow nodes associated with plumer-shelf
nodularity in gastric ca.
95.
Local examination :
•Site of chief complaint.
• Lymph nodes groups
• Thyroid
• Other salivary glands ( parotid / submandibular and sub linguial)
96.
Lymph nodes
• Examineall groups of lymph nodes ( cervical /axillary / inguinal )
• Rolling by tip of the finger
• A- cervical nodes :
• Examined from the front except post auricular / supraclavicular and
occipital
• super facial :
• submental /sub mandibular / pre and post auricular and occipital ( horizontal )
• Along internal and external jag. Vein ( vertical )
97.
• Supraclavicular nodes( Examined from the back )
• Scalene nodes ( between the tow heads of SCM )
• Deep :
• Waldeyr’s ring ( tonsils …NHL)
• Delphian nodes
• Along the int jag. Vein
99.
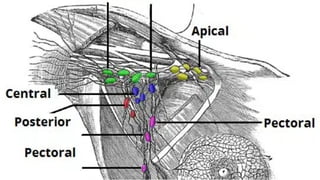
-Axillary nodes :
•5 groups :
• Central ( medial group) …chest wall…base of the axilla
•Apical
•Pectoral anterior
•Sub scapular ( posterior )
•Humeral lateral
101.
• Inguinal anodes: ( the patient is lying down )
• Superficial:
• horizontal….. along inguinal ligament
• vertical …. along the great saphenous vein 5 cm from the saphenous opening
• Deep : usually not palpated
102.
•Comments:
• By inspection:
• Symptoms of inflammation redness ( NHL)
• Pyogenic abscess
• By palpation :
• Number ……….site ( which region ?)
• Size …. The largest and thehsmallest ?
103.
• Shape:
• rounder…oval …. Regularity ?
• Edge:
• Discrete : infection …HL….
• Matted ( fused can be counted ) : malignant …radiotherapy
• Amalgamated ( fused cannot be counted ) : NHL
• Warmth
• Surface : smooth or irregular
104.
• Consistency :
•Solid / cystic …abscess
• Firm :acute lymph-adenitis
• Rubbery : HL
• Hard :malignancy
• Tenderness:
• non tender ( malignant )
• tender ( infection )
• Mobility : mobile or fixed to the surroundings
105.
•Thyroid :
• Itwill be discussed alone ( later on).
• But in general ( midline swelling moves up and down with swallowing ).
• But in general ( midline swelling moves up and down with swallowing ).
•Inspection
•Palpation
•Percussion
•Auscultation
106.
Salivary glands exam:
• Parotid :
• Examine the swelling or the pain as mentioned earlier in the parotid region
Infront of the ear.
• Examine the duct :
• By tip of the finger rolling against contracted masater muscle finger breadth
below the zygomatic arch.
• examine the duct orifice :
• opposite to the upper 2ed molar tooth:
107.
Loading…
• Submandibular gland:
•The same as for pain or swelling but in the submandibular triangle
• Examine for the swelling or the pain as earlier but also :
• Examine lymph nodes ….( how to differentiate )
• Lingual nerve : ( numbness in the ant 2/3 of the tongue )
• Examine the Wharton’s duct : inspect the floor of the mouth duct orifice on
both sides of the frenulum for redness or inflammation
108.
3-Images
• Neck us: gold standered
• Neck CT : to check for the extension ( L.N / RSG)
• Neck MRI : to delineate soft tissue relations
• Angiography : for carotid body tumors and major vessels
• PET scan / DOTATEC scan to R/O distant Mets.
109.
Sheet for theneck swellings :
• After doing the usual examination :
1- Unilateral or bilateral ?
2- Fluctuation test : solid / cystic ?
3- Impulse on cough and decreased by compression :
• complete : laryngeocele /pneumocele / zencker’s Diverticulum
• partially : cystic hygroma/ cavernous hemangioma
4-translumination : Brilliant …cystic hygroma
110.
Translucent ….ranula ..
5-mobility with swallowing and with tongue protrusion :
with swallowing :
thyroid / thyroglossal cyst / laryngeo-cele/ delphian L.N
Tongue protrusion :
thyroglossal cyst / subthyroid bursitis
111.
6- Below orabove SCM : Branchial cyst partially covered by SCM
7- pulsation : Expansile or transmitted ( Carotid body tumor )
8- Submandibular swelling : Rolling over the mandible
Bi-digitally
9-Carotid pulsation : displaced or equally felt
10-Cervical lymph nodes
11-Tracheal deviation
112.
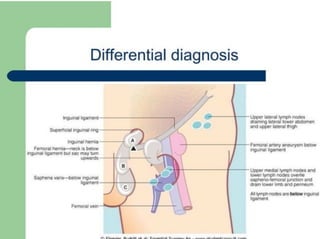
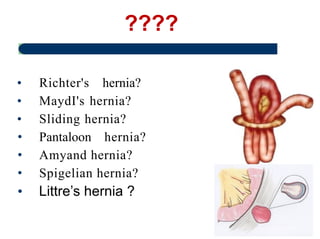
D.D. Of AMass In The Neck
• Mid line swellings
• Solid swellings:
• Submental LN enlargement.
• Nodule in the isthmus of thyroid gland.
• Cystic swellings:
1- Cold abscess : Rare in the midline.
2- Dermoid cyst: Sublingual or suprasternal.
3- Sub-hyoid bursitis: It is a rare, tender, oval swelling which lies transversely
beneath the hyoid bone. It moves up and down with deglutition & with
protrusion of the tongue .
4-Laryngocele: It occurs in musicians playing with air-blown instruments. - It
113.
is a herniationof laryngeal mucosa through the thyrohyoid membrane. . - The
Swellings in the Digastric ( sub mandibular )
triangle
• 1. Enlarged submandibular LNs: multiple, can be rolled over the edge
of the mandible & can’t be felt in the floor of the mouth.
• 2. Enlarged submandibular salivary gland.
114.
Swellings in theCarotid triangle
• Solid swellings:
• 1. Enlarged upper deep cervical LNs.
• 2. The upper part of an enlarged lateral lobe of the thyroid gland.
• 3. Carotid body tumor:
• It is a rare slowly growing malignant tumor arising from the chemoreceptors
present at the bifurcation of the carotid artery.
• It's usually smooth but may be lobular.
• The swelling moves from side to side but not vertically. It may be pulsating. _
• Investigations Angiography can prove the diagnosis.
• Treatment - By excision of the tumor with preservation of the ICA. - If
preservation of the ICA is impossible, it should be replaced by a graft.
• Cystic swellings:
115.
Swellings in thePosterior triangle
• Solid swellings:
• 1. Enlarged LNs.
• 2. Neurofibroma arising from the brachial plexus.
• 3. Cervical rib.
• Cystic swellings:
• 1. Cystic hygroma
• 2. Pharyngeal pouch
• 3. Cold abscess
• 4. Pneumatocele: This is a cystic swelling in the supraclavicular region, which
is resonant & compressible. It is due to herniation of the pleura in the base of
the neck.
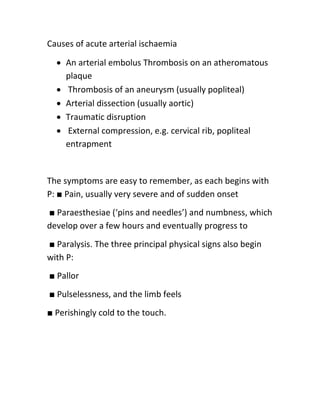
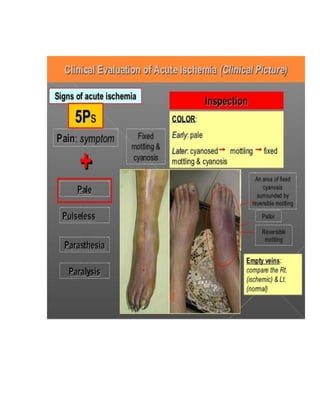
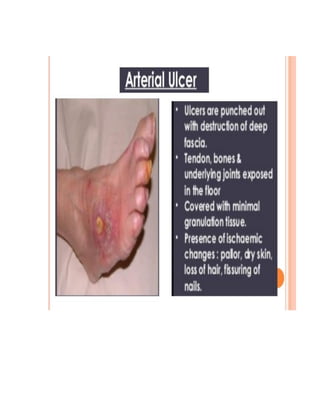
Causes of acutearterial ischaemia
An arterial embolus Thrombosis on an atheromatous
plaque
Thrombosis of an aneurysm (usually popliteal)
Arterial dissection (usually aortic)
Traumatic disruption
External compression, e.g. cervical rib, popliteal
entrapment
The symptoms are easy to remember, as each begins with
P: ■ Pain, usually very severe and of sudden onset
■ Paraesthesiae (‘pins and needles’) and numbness, which
develop over a few hours and eventually progress to
■ Paralysis. The three principal physical signs also begin
with P:
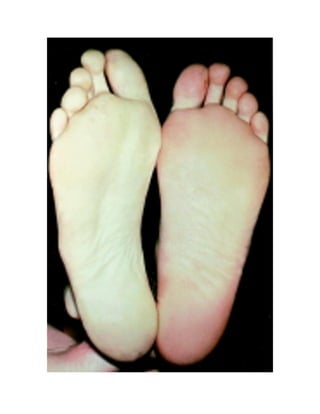
■ Pallor
■ Pulselessness, and the limb feels
■ Perishingly cold to the touch.
150.
The causes oflymphoedema
Primary Congenital genetic disorders causing dilatation,
incompetence, aplasia or obliteration of the lymphatics
Secondary Neoplastic infiltration of lymph glands by:
secondary carcinoma lymphomas (Hodgkin’s/non-
Hodgkin’s)
Infection
Filariasis
Lymphogranuloma inguinale
Tuberculosis
Recurrent non-specific infection Iatrogenic
Surgical excision of lymph glands Irradiation of lymph
glands
154.
الرحيم الرحمن )ابسم
Faculty Of Medicine And Health Science.
Surgical Department
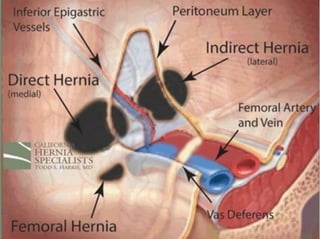
Inguino-Scrotal Conditions
Dr.Anas Asafrah
General surgeon
Aug-2024
History of presentation
•Age
— Infants.
— adolescents and young
adults.
— Old adults 40-60 years.
• Sex.
• Occupation:
Heavy object lifting, works in
a bakery, area of radiation.
158.
Loading…
History of presentation
•Local Symptoms:
— Swelling.
— Dragging sensation.
— pain.
• Ask about predisposing factors:
Chronic cough .
Chronic constipation .
Straining with micturition.
Loading…
Standing position
• Exposure(nipple to knee)
• Ask patient to stand up.
• Inspection:
— Site
• Right or left
• Above or below groin
cease
• Reaches the scrotum
or not
165.
• Size.
• Shape.
•Skin over it.
• Pulsatile or not.
• Is there any discharges.
• If it is apparent with cough?
• Can Patient reduce it or not?
• Any other swellings?
166.
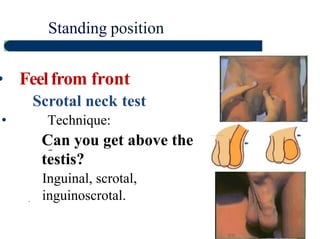
Standing position
• Feelfromfront
Scrotal neck test
• Technique:
Can you get above the
testis?
Inguinal, scrotal,
inguinoscrotal.
.
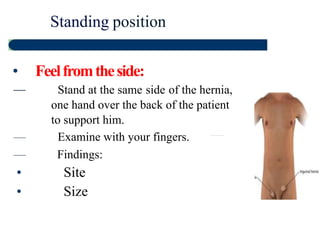
Standing position
• Feelfromtheside:
—Stand at the same side of the hernia,
one hand over the back of the patient
to support him.
— Examine with your fingers.
— Findings:
• Site
• Size
170.
• shape
• Temperature
•Tenderness.
• Composition.
• Reducibility.
• Expansile impulse with cough.
171.
Standing position
• Expansileimpulse with cough:
—
Technique.
-The swelling should become tense and expand
with coughing, not moves up and down only in one
direction.
• It is diagnostic for hernia but can be absent in
complicatecl ones.
Standing and supineposition
• Reducibility:
➢ Can be tried on standing position, if failed,
repeat in supine position.
➢ Technique:
Put the hand on the lump, lift it upward and backward
gently,
Slide your fingers upward and laterally towards the
internal ring. Controlled?
174.
➢ Do notreduce the hernia “ en
masse”, reduce the bowel with the
peritoneal sac.
➢ Findings:
• Reducible, irreducible
• Direction of reduction
• Difficulty in reduction
175.
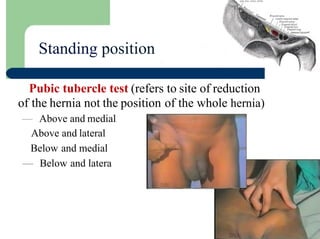
Standing position
Pubic tubercletest (refers to site of reduction
of the hernia not the position of the whole hernia)
— Above and medial
Above and lateral
Below and medial
— Below and latera
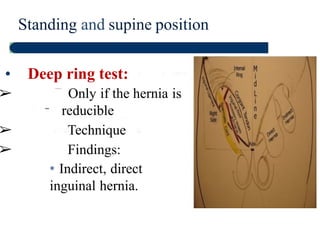
Standing and supineposition
• Deep ring test:
➢ Only if the hernia is
reducible
➢ Technique
➢ Findings:
* Indirect, direct
inguinal hernia.
181.
Standing and supineposition
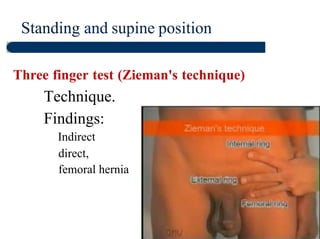
Three finger test (Zieman's technique)
• Technique.
Findings:
Indirect
direct,
femoral hernia
182.
Loading…
Standing or supineposition
• Percussion
— Intestinal or omental
contents.
• Auscultation
— Peristalsis.
183.
DO NOT FORGET
•To examine the contra-lateral side of
the groin region.
• To examine the scrotum.
• To examine the abdomen and PR
exam:
184.
For any causecan elevate the intra-
abdominal pressure ( enlarged
prostate, Ascites, Pregnancy, intra-
abdominal masses, Intestinal
Obstruction).
• Cardiovascular and respiratory
assessment.
185.
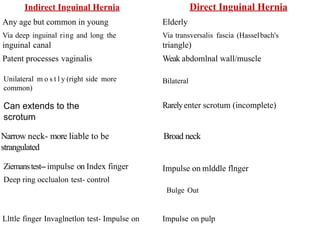
Indirect Inguinal HerniaDirect Inguinal Hernia
Any age but common in young
Via deep inguinal ring and long the
inguinal canal
Patent processes vaginalis
Elderly
Via transversalis fascia (Hasselbach's
triangle)
Weak abdomlnal wall/muscle
Unilateral m o s t l y (right side more
common)
Bilateral
Rarelyenter scrotum (incomplete)
Narrow neck- more liable to be
strangulated
Broad neck
Ziemanstest--impulse on Index finger
Deep ring occlualon test- control
Impulse on mlddle flnger
Bulge Out
Llttle finger Invaglnetlon test- Impulse on Impulse on pulp
Can extends to the
scrotum
186.
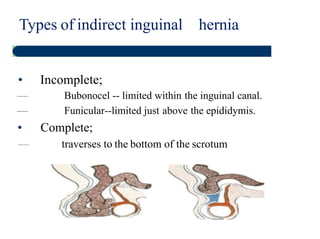
Types of indirectinguinal hernia
• Incomplete;
— Bubonocel -- limited within the inguinal canal.
— Funicular--limited just above the epididymis.
• Complete;
— traverses to the bottom of the scrotum
187.
• Right, Left.
•Site (inguinal, femoral).
• Direct or indirect.
• Complete or incomplete.
• Content (omentum or bowel).
• Uncomplicated (Reducible) or complicated
(irreducible, obstructed, strangulate},
• PPT factors.
How to make a definitive diagnosis
for hernia:
Loading…
History Taking
● Ahistory is the story of the patients illness
● It is the first step in determining the etiology of
a patient’s problem
● Let the patient describe his or her problem
● Be a medical detective to establish the diagnosis
198.
History Taking
● 80% of diagnosis may be made from history
alone
● Examination and investigations would either
confirm or refute the history based diagnosis
199.
Loading…
Skills Needed forhistory taking:
The ability to :
● Understand and be understood
● Obtain relevant information
● Interview logically
● Interrupt when necessary without inhibiting patient
● Look for non verbal clues
● Establish good relationship with patients
● Be able to summarize the information
200.
● The patientinitiates this by describing a
particular symptom which you would use for
additional questioning that will help identify
the cause of the problem
201.
Understanding the Pathophysiologyof
disease (Medical Knowledge) as well as
Increased Exposure to Patients and
disease will improve the skill of taking a
good history
202.
The Most ImportantSymptoms
are:
● Cough
● Sputum production
● Hemoptysis
● Breathlessness
● Wheeze
● Chest pain
203.
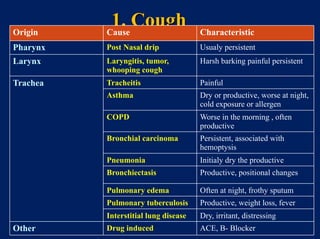
1. Cough
Origin CauseCharacteristic
Pharynx Post Nasal drip Usualy persistent
Larynx Laryngitis, tumor,
whooping cough
Harsh barking painful persistent
Trachea Tracheitis Painful
Asthma Dry or productive, worse at night,
cold exposure or allergen
COPD Worse in the morning , often
productive
Bronchial carcinoma Persistent, associated with
hemoptysis
Pneumonia Initialy dry the productive
Bronchiectasis Productive, positional changes
Pulmonary edema Often at night, frothy sputum
Pulmonary tuberculosis Productive, weight loss, fever
Interstitial lung disease Dry, irritant, distressing
Other Drug induced ACE, B- Blocker
204.
How To AssessCough ?
It is important to ask about :
● Frequency: Intermittent or Persistent
● Severity: Diurnal variation
● Character: dry or productive
● Associated symptoms: e.g chest pain
● What is responsible or triggered by:
• Sputum in the respiratory tract e.g. in acute infections
or Bronchiectasis
• Cigarette smoke
• Pungent smell
• Cold air
205.
Loading…
2.SPUTUM
TYPES:
● Mucoid asin Chronic Bronchitis
● Green or Yellow in Infection
● Bloody in bronchogenic carcinoma, T.B
● Rusty colour in Pneumonia
● Pink and frothy in Pulmonary oedema
● Foul smelling suggest anaerobic infection
● Clear watery, large volume (Bronchorrhea ) in alveolar cell
carcinoma
206.
How To AssessSputum ?
It is important to ask about:
● Color
● Amount OR Volume, fill a teaspoon, tablespoon,
eggcup, a sputum cup
● Positional changes
● Taste or Smell
● Viscosity
● Blood stained
How to assessHAEMOPTYSIS?
It Is Important To Ask About:
● Is it frank blood or associated with purulent sputum
● Is it frank blood or streaks of blood
● Amount ?
● Is it coughed up or vomited
● Previous respiratory illnesses e.g.Tuberculosis, Bronchiectasis
● DVT, connective tissue disease
BREATHLESSNESS
Pulmonary causes:
• COPD
•Pulmonary fibrosis.
• Pulmonary collapse due to
obstructing bronchial
carcinoma
• Pneumonia
• Asthma
• Airway occlusion by FB,
laryngeal Edema
• Spontaneous Pneumothorax
• Acute pulmonary embolism
Others:
● Psychogenic
● Anemia
● Pleural effusion
● Pulmonary embolism
● Acute pulmonary edema due
to left heart failure, MI,
arrhythmia
Days-
Weeks
Hours
M
in
ut
es
211.
How To AssessA Patient With
Breathlessness?
1. Onset progression:
• Acute , sudden Or Gradual over a prolonged
period or time
• Progression the time period over which
breathlessness developed
2. Timing
• Early morning: severe asthma and LVF
• During the week: Occupational asthma
• Winter: Bronchitis
• Spring: Atopic asthma
212.
3. Severity orGrade:
How far the patient can walk on the flat without stopping
How many steps can be climbed without stopping
Do you feel breathless when washing or dressing
Do you feel breathless at rest
4. Variability:
Episodic ( intermittent) or persistent
Worse at night and early morning (morning dippers in asthma)
Lying flat (orthopnea) in heart failure and severe airway
obstruction
5. AGGREVATING RELIEVING FACTORS:
Exercise, cold exposure, Excitement, Drugs
213.
5. WHEEZE
● Musicalsound best heard on expiration
● Common in patients with airways obstruction caused by
Asthma or COPD
May be present only:
● At night or early morning, on exposure to cold air or
allergen and on exercise
● Diffuse expiratory wheezes may occur in SEVERE
LEFT HEART FAILURE
214.
STRIDOR
● Noisy respiration,always inspiratory
● Indicates central large airway obstruction
● Causes:
Carcinoma Larynx
Tracheal stenosis
Extrinsic compression
215.
6. CHEST PAIN
CausesOf Central Chest Pain
● Tracheitis and bronchitis
● Angina
● Massive pulmonary embolism
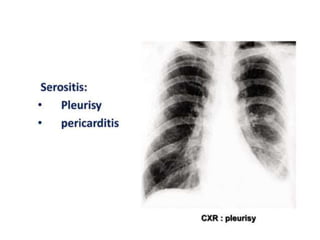
● Pericarditis
● Acute aortic dissection
● Esophagitis
● Large central tumor
216.
Causes Of LateralChest Pain:
Pleural Pain:
● Sharp and stabbing in character
● Localized or referred to shoulder tip if diaphragmatic
pleura is involved
● Worse on deep inspiration or cough, if severe,
shallow breathing, avoidance of movement, and
cough suppression
● Results from inflammatory or malignant involvement
of the parietal pleura e.g. Pneumonia, Pulmonary
infarction, Malignancy, Lung abscess, Rheumatoid
arthritis
217.
SUMMARY
CAUSES OF CHESTPAIN
STRUCTURE Possible CAUSE of pain
Pleura Inflammation, infarction
Muscle Strain from coughing
Bone Rib fracture or Tumour
Costochondral junction Tietze’s syndrome
Nerves Herpes zoster, Pancoast tumor
Heart and great vessels Cardiac ischemia, Infarction,
aortic dissection, aneurysm
Esophagus Spasm reflux
218.
How To AssessA Patient With Chest
Pain
Enquire about:
● Site
● Mode of onset
● Character
● Radiation
● Intensity
● Precipitating , Aggravating and relieving factors.
● Relationship to breathing, coughing or movement
219.
Co-existing Symptoms
● Fever
●Hoarseness of voice
● Ankle swelling
● Poor appetite and weight loss
● Snoring and day time sleepiness
Loading…
University Question:
A 32-year-oldpatient was found to have a large, free-
layering, transudative pleural effusion at the right
hemithorax. All of the following are expected findings
on
physical examination; except:
A. Absent or decreased breath sounds at the right
hemithorax
B. Increased vocal fremitus at the right hemithorax
C. Lag on chest wall motion at right hemithorax
D. Normal percussion at left hemithorax
224.
University Question:
A 32-year-oldpatient was found to have a large, free-
layering, transudative pleural effusion at the right
hemithorax. All of the following are expected findings
on
physical examination; except:
A. Absent or decreased breath sounds at the right
hemithorax
B. Increased vocal fremitus at the right hemithorax
C. Lag on chest wall motion at right hemithorax
D. Normal percussion at left hemithorax
225.
Loading…
Introduction:
● Wash hands
●Introduce your self to the patient using your
full name
● Confirm you have the correct patient
● Explain what you would like to do
● Gain verbal consent
● Ensure privacy
● Ask the patient to undress from the waist
upwards
226.
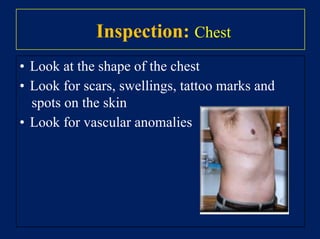
Inspection: Bed area
Statethat you would look for:
● Oxygen supply
● Nebulizers
● Inhalers
● Sputum pot
● Peak flow meter
227.
Inspection: The patient
•Do they look ill? If so; in what way?
• Weight loss
• Breathlessness
• Pursed lips breathing
• Cyanosis
• Use of accessory muscles
228.
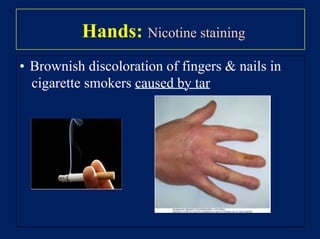
Inspection: Hands
• Nicotinestaining
• Peripheral cyanosis
• Clubbing
• Wasting of small muscles of the hands
• Tremor Bronchiectasis
Lung abscess
Empyema
Lung cancer
Mesohelioma
Idiopathic pulmonary fibrosis
Asbestosis
Cystic fibrosis
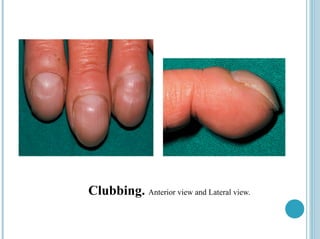
Clubbing:
229.
Inspection: Hands
Peripheral cyanosis
•Hands feel warm and peripherally cyanosed
c/w cold hands in circulatory failure
• Usually due to circulatory disorders but occurs
in patients with severe central cyanosis
Loading…
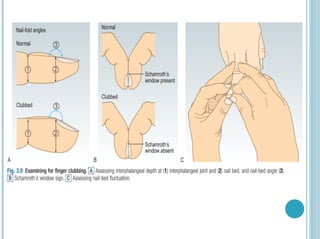
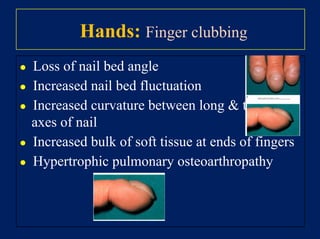
Hands: Finger clubbing
●Loss of nail bed angle
● Increased nail bed fluctuation
● Increased curvature between long transverse
axes of nail
● Increased bulk of soft tissue at ends of fingers
● Hypertrophic pulmonary osteoarthropathy
232.
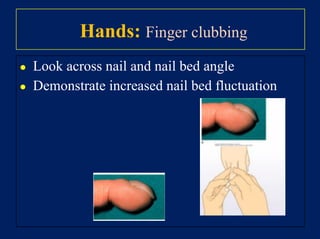
Hands: Finger clubbing
●Look across nail and nail bed angle
● Demonstrate increased nail bed fluctuation
233.
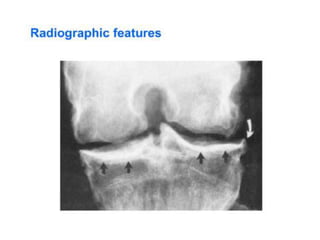
HPOA:
• Clubbing +arthralgia with joint swelling of
wrists and ankles
• X-rays show subperiosteal new bone formation
Right ankle
radiograph
demonstrating
periosteal
reaction along
distal tibial
and fibular
diaphysis
(arrows).
234.
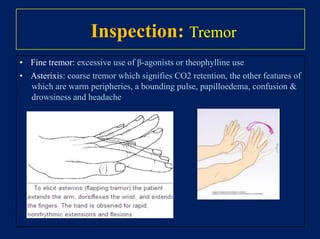
Inspection: Tremor
• Finetremor: excessive use of β-agonists or theophylline use
• Asterixis: coarse tremor which signifies CO2 retention, the other features of
which are warm peripheries, a bounding pulse, papilloedema, confusion
drowsiness and headache
Inspection: Face CentralCyanosis
• Bluish discoloration of the skin mucous
membranes, caused by an absolute
concentration of deoxygenated hemoglobin
50 gm/L
238.
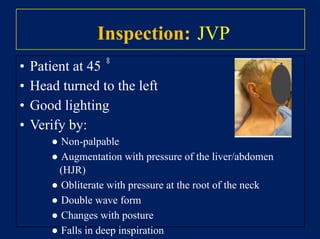
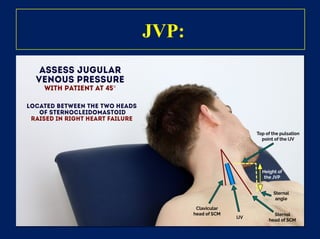
Inspection: JVP
• Patientat 45 ̊̊
• Head turned to the left
• Good lighting
• Verify by:
● Non-palpable
● Augmentation with pressure of the liver/abdomen
(HJR)
● Obliterate with pressure at the root of the neck
● Double wave form
● Changes with posture
● Falls in deep inspiration
239.
JVP:
• Measure fromthe sternal angle to the top of
pulsation
• Raised JVP if 4 cm:
– Pulmonary embolism
– Cor-pulmonale
– SVC obstruction “ NON-PULSATILE”
– Tension pneumothorax
– Acute asthma
240.
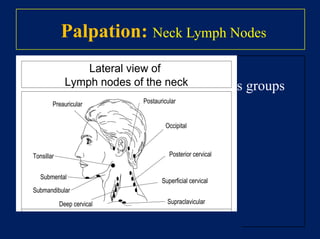
Palpation: Neck LymphNodes
• Examine from behind
• Check for enlargement of neck nodes groups
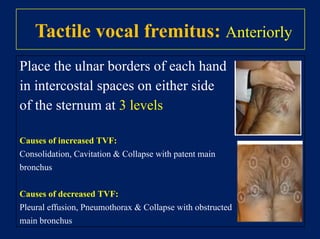
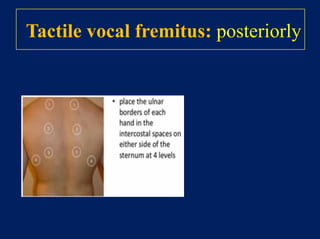
Tactile vocal fremitus:Anteriorly
Place the ulnar borders of each hand
in intercostal spaces on either side
of the sternum at 3 levels
Causes of increased TVF:
Consolidation, Cavitation Collapse with patent main
bronchus
Causes of decreased TVF:
Pleural effusion, Pneumothorax Collapse with obstructed
main bronchus
254.
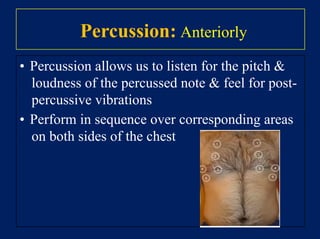
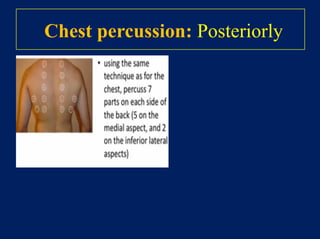
Percussion: Anteriorly
• Percussionallows us to listen for the pitch
loudness of the percussed note feel for post-
percussive vibrations
• Perform in sequence over corresponding areas
on both sides of the chest
255.
Percussion Note:
• Resonant:Normal lung
• Dull: Over liver heart, pulmonary
consolidation some cases of collapse and
pleural thickening
• Impaired: Junction of the liver heart with the
lung, pulmonary fibrosis, pulmonary
consolidation some cases of collapse
• Stony dull: Pleural effusion
• Hyper-resonant: Pneumothorax emphysema
• Tympanic: Hollow viscus (empty stomach)
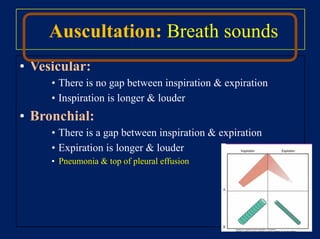
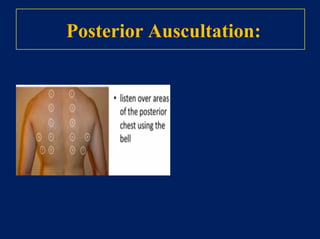
Auscultation: Breath sounds
•Vesicular:
• There is no gap between inspiration expiration
• Inspiration is longer louder
• Bronchial:
• There is a gap between inspiration expiration
• Expiration is longer louder
• Pneumonia top of pleural effusion
258.
Decreased breath sounds:
•Reduced conduction:
• Obesity, thick chest wall
• Pleural effusion or thickening
• Pneumothorax
• Reduced air flow:
• Generalized, e.g. COPD
• Localized, e.g. collapsed lung due to occluding lung
cancer
259.
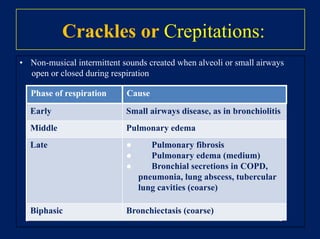
Crackles or Crepitations:
•Non-musical intermittent sounds created when alveoli or small airways
open or closed during respiration
Phase of respiration Cause
Early Small airways disease, as in bronchiolitis
Middle Pulmonary edema
Late ● Pulmonary fibrosis
● Pulmonary edema (medium)
● Bronchial secretions in COPD,
pneumonia, lung abscess, tubercular
lung cavities (coarse)
Biphasic Bronchiectasis (coarse)
260.
Wheezes:
• They havemusical quality usually occur in
expiration and indicate narrowing of an airway
• The smaller the airway, the higher the pitch of the
wheeze
High pitched: Asthma COPD
Low pitched: Bronchial cancer
261.
Pleural rub:
• Creakingsound due to two inflamed layers of
pleural membrane rubbing against each other
during inspiration expiration
• Patient may also have pleuritic chest pain at the
same site
• Causes: pneumonia, pulmonary embolism
vasculitis
262.
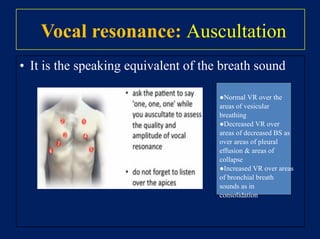
Vocal resonance: Auscultation
•It is the speaking equivalent of the breath sound
●Normal VR over the
areas of vesicular
breathing
●Decreased VR over
areas of decreased BS as
over areas of pleural
effusion areas of
collapse
●Increased VR over areas
of bronchial breath
sounds as in
consolidation
Finishing Up YourExamination
Thank the patient, explain that the
examination is now over and invite him to
dress
271.
I would also……
•I would also like to examine for ankle and
sacral edema
• Examine the sputum
• Look at the temperature chart
• Perform a peak expiratory flow test
272.
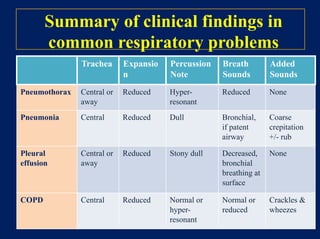
Summary of clinicalfindings in
common respiratory problems
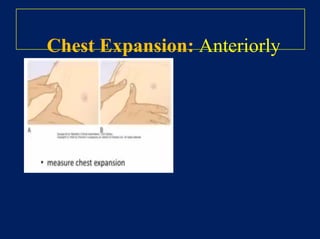
Trachea Expansio
n
Percussion
Note
Breath
Sounds
Added
Sounds
Pneumothorax Central or
away
Reduced Hyper-
resonant
Reduced None
Pneumonia Central Reduced Dull Bronchial,
if patent
airway
Coarse
crepitation
+/- rub
Pleural
effusion
Central or
away
Reduced Stony dull Decreased,
bronchial
breathing at
surface
None
COPD Central Reduced Normal or
hyper-
resonant
Normal or
reduced
Crackles
wheezes
Liver disease
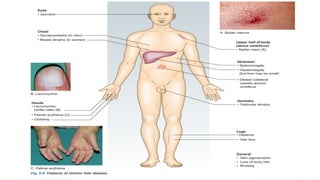
• Palmarerythema and spider naevi:
Spider naevi are isolated telangiectasias that characteristically fill from a
central vessel and are found in the distribution of SVC (upper trunk, arms
and face).
• Women may have up to five spider naevi in health; palmar erythema and
numerous spider naevi are normal during pregnancy.
• In men, these signs suggest chronic liver disease.
280.
Liver disease
• Gynaecomastia(breast enlargement in males), with loss of body hair and
testicular atrophy, may occur due to reduced breakdown of oestrogens.
• Leuconychia, caused by hypoalbuminaemia.
• Finger clubbing is found in liver cirrhosis, IBD, and malabsorption
syndromes.
282.
Abdominal examination
• Examinethe patient in
1-good light
2-warm surroundings
3-positioned comfortably supine with the head resting on only one or two pillows
• Use extra pillows to support a patient with kyphosis or breathlessness.
284.
Loading…
Skin
• Seborrhoeic warts,ranging from pink to brown or black.
• Haemangiomas (Campbell de Morgan spots)
• They are common and normal in older patients.
• Note any striae, bruising or scratch marks.
285.
Visible veins
• Abnormallyprominent veins on the abdominal wall suggest
portal hypertension or vena cava obstruction.
• In portal hypertension:
recanalisation of the umbilical vein along the falciform ligament produces
distended veins that drain away from the umbilicus: the ‘caput medusae’.
286.
Continued
• Dilated tortuousveins with blood flow superiorly are collateral veins
caused by obstruction of the inferior vena cava.
• Rarely, superior vena cava obstruction gives rise to
similarly distended abdominal veins, but these all flow inferiorly.
287.
Abdominal swelling
• Diffuseswelling could be due to ascites or intestinal obstruction.
• Localized swelling could be to urinary retention, a mass or an enlarged
organ such as the liver.
• The umbilicus is usually sunken in obesity;
in ascites, it is flat or, more commonly, everted.
• Look tangentially across the abdomen and from the foot of the bed for
any asymmetry suggesting a localized mass.
288.
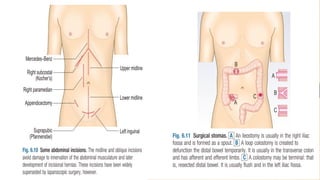
Abdominal scars andstomas
• Note any surgical scars or stomas and clarify what operations have been
undertaken (Figs 6.10 and 6.11).
• A small infraumbilical incision usually indicates a previous laparoscopy.
Puncture scars from laparoscopic surgical ports may be visible.
• An incisional hernia at the site of a scar is palpable as a defect in the
abdominal wall musculature and becomes more obvious as the patient
raises their head off the bed or coughs.
292.
Tenderness
• Discomfort duringpalpation may vary and may be accompanied by
resistance to palpation.
• Consider the patient’s level of anxiety when assessing the severity of pain
and degree of tenderness elicited.
• Tenderness in several areas on minimal pressure may be due to
generalised peritonitis but is more often caused by anxiety.
293.
Continued
• Voluntary guardingis the voluntary contraction of the abdominal
muscles when palpation provokes pain.
• Involuntary guarding is the reflex contraction of the abdominal muscles
when there is inflammation of the parietal peritoneum.
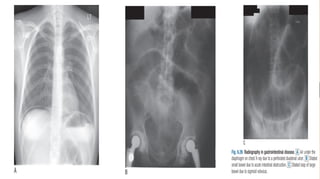
• If the whole peritoneum is inflamed (generalised peritonitis) due to a
perforated viscus, the abdominal wall no longer moves with respiration;
breathing becomes increasingly thoracic and the anterior abdominal wall
muscles are held rigid (board-like rigidity).
294.
Continued
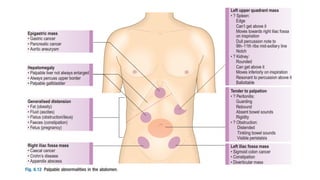
• The siteof tenderness is important. (Fig. 6.12).
• Specific abdominal signs are shown in Box 6.9.
• Ask the patient to cough or gently percuss the abdomen to elicit any pain
or tenderness ‘Rebound tenderness’, when rapidly removing your hand
after deep palpation increases the pain, is a sign of intra-abdominal disease
but not necessarily of parietal peritoneal inflammation (peritonism).
• Typical findings may be masked in patients taking glucocorticoids,
Enlarged organs
• Examinethe liver, gallbladder, spleen and kidneys in turn during deep
inspiration.
• Keep your examining hand still and wait for the organ to move with
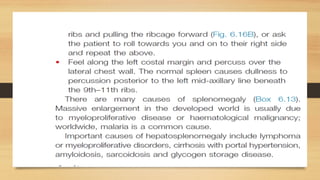
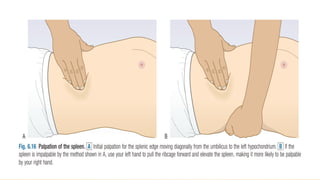
breathing.
• Do not start palpation too close to the costal margin, missing the edge of
the liver or spleen.
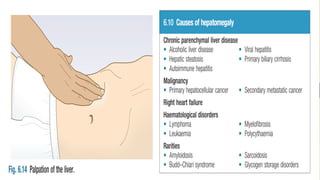
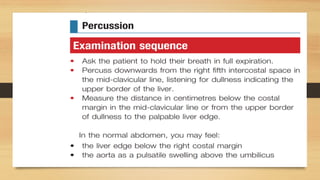
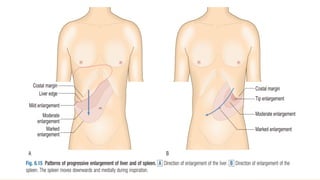
Continued
• Hepatic enlargementcan result from chronic parenchymal liver disease from
any cause (Box 6.10).
• The liver is enlarged in early cirrhosis but often shrunken in advanced
cirrhosis.
• Fatty liver (hepatic steatosis) can cause marked hepatomegaly.
• Hepatic enlargement due to metastatic tumour is hard and irregular.
306.
Continued
• An enlargedleft lobe may be felt in the epigastrium or even the left hypochondrium.
• In right heart failure, the congested liver is usually soft and tender; a pulsatile liver
indicates tricuspid regurgitation.
• A bruit over the liver may be heard in acute alcoholic hepatitis, hepatocellular cancer
and arteriovenous malformation. The most common reason for an audible bruit over
the liver, however, is a transmitted heart murmur.
307.
Continued
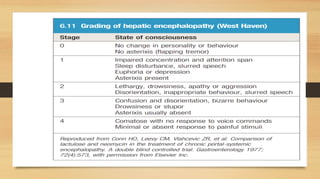
• Liver failureproduces additional symptoms of encephalopathy,
which can be graded (Box 6.11).
• Resonance below the 5th ICS suggests hyperinflated lungs or
occasionally the interposition of the transverse colon between
the liver and the diaphragm (Chilaiditi’s sign).
308.
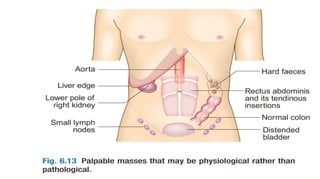
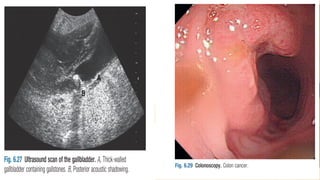
Gall Bladder
• Palpabledistension of the GB is rare and has a characteristic globular
shape. It results from either obstruction of the cystic duct, or obstruction
of the common bile duct with a patent cystic duct, as in pancreatic cancer.
• In a jaundiced patient a palpable gallbladder is likely to be due to
extrahepatic obstruction, such as from pancreatic cancer or, very rarely,
gallstones (Courvoisier’s sign).
• In gallstone disease the gallbladder may be tender but impalpable because
of fibrosis of the gallbladder wall.
322.
Continued Ascultation
• Absenceof bowel sounds implies paralytic ileus or peritonitis.
• In intestinal obstruction, bowel sounds occur with increased frequency
and volume, and have a high-pitched, tinkling quality.
• Bruits suggest an atheromatous or aneurysmal aorta or superior
mesenteric artery stenosis.
• An audible splash more than 4 hours after the patient has eaten or drunk
323.
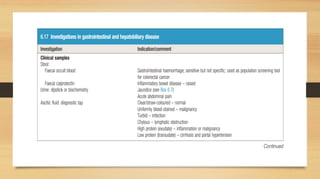
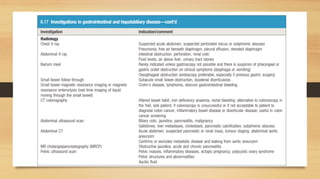
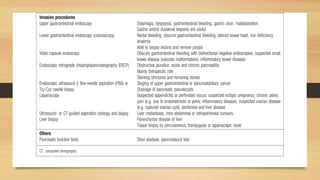
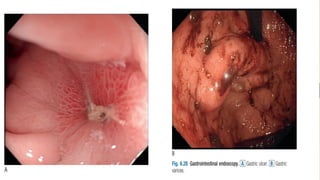
Investigations
• Selecting therelevant investigation depends on the clinical problem
revealed on history and examination.
• Investigations are costly and many carry risks.
• So choose tests capable of distinguishing the likely diagnoses and
prioritize the most decisive ones (Box 6.17 and Figs 6.26–30).
331.
BREAST Hx PE
AREF OMAR, MD ,
GENERAL SURGEON
(AVH)
332.
Opening the consultation
•Introduce yourself name/role
• Confirm patient details – name/DOB
• Explain the need to take a history Gain
consent
• Ensure the patient is comfortable
333.
Presenting complaint
• It’simportant to use open questioning to elicit the patient’s
presenting complaint
• “So what’s brought you in today?” or “Tell me about your
symptoms”
• Allow the patient time to answer
• trying not to interrupt or direct the conversation.
• Facilitate the patient to expand on their presenting complaint if
required.
• “Ok, so tell me more about that” “Can you explain what that
pain was like?”
334.
History of presentingcomplaint
• Questions to ask about the lump
• Onset – When did they first notice the lump?
• Size – Has it changed? / Over what duration?
• Is the lump’s size or discomfort related to the
menstrual cycle in any way?
• Is the lump painful? – ask SOCRATES
335.
Pain
• if painis a symptom, clarify the details of the pain
using SOCRATES
• Site – where is the pain
• Onset – duration? / sudden vs gradual?
• Character – sharp / dull ache / burning
• Radiation – does the pain move anywhere else?
• Associations – other symptoms associated with the
pain (e.g. fever)
• Time course – worsening / improving / fluctuating
• Exacerbating / Relieving factors – does anything make
the pain worse or better?
• Severity – on a scale of 0-10 how severe is the pain?
336.
Local associated symptoms
•Nipple discharge or bleeding?
• Nipple inversion? – Is this new or has it always
been the case?
• Skin changes overlying the lump or elsewhere
on the breast?
• Eczema
• Dimpling
• Ulceration
If any ofthe above symptoms are
present, gain further details
• Onset – When did the symptom start? / Was the onset
acute or gradual?
• Duration – Days / Weeks / Months / Years
• Severity – i.e. How much is the given symptom impacting
on their life?
• Course – Is the symptom worsening, improving, or
continuing to fluctuate? Intermittent or continuous? – Is
the symptom always present or does it come and go?
• Precipitating factors – Are there any obvious triggers for
the symptom?
• Relieving factors – Does anything appear to improve the
symptoms?
• Previous episodes – Has the patient experienced this
symptom previously?
340.
Ideas, Concerns andExpectations
• Ideas – what are the patient’s thoughts
regarding their symptoms?
• Concerns – explore any worries the patient
may have regarding their symptoms
• Expectations – gain an understanding of what
the patient is hoping to achieve from the
consultation
Relevant past medicalhistory:
• Recent breast trauma – fat necrosis
• Previous breast disease – malignant or
benign?
• Any other previous malignancies?
• Other significant medical problems?
Drug history
• Relevantprescribed medication:
• Oral contraceptive pill
• Hormonal replacement therapy
• Other regular medications
• Over the counter drug
Social history
• Smoking– How many cigarettes a day? How
many years have they smoked for?
• Alcohol – How many units a week? –
type/volume/strength Recreational drug use?
347.
Systemic enquiry
• Systemicenquiry involves performing a brief screen for
symptoms in other body systems.
• This may pick up on symptoms the patient failed to
mention in the presenting complaint.
• Some of these symptoms may be relevant to the
diagnosis (e.g. back pain in metastatic breast cancer).
• Choosing which symptoms to ask about depends on
the presenting complaint and your level of experience
find the mainsymptom
analyse
and then
you must ask about the other three
directly
350.
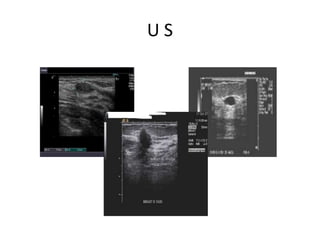
Triple assessment
1. Historyand Clinical examination
2. Radiological: Mammography
or ultrasound
3. Pathology : Cyto or Histology
351.
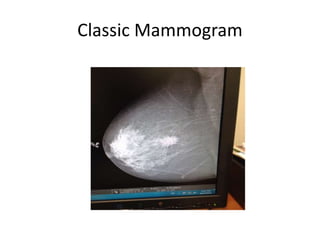
Radiology
• Mammogram
• forover 30
• good for screening
• but cannot differentiate between cystic and solid lesions.
• Ultrasound
• is suitable for the young breast
• can differentiate cystic and solid lesions
• is good at assessing sizes and may complement a
mammographically detected abnormality.
352.
Assessment of theaxilla with US is
Mandatory if cancer is suspected and,
at least FNA (if not core) of any
abnormal looking node is good
practice
MRI
• MRI: ifextent of disease cannot be
assessed.
• If there is discrepancy between clinical
and imaging findings
• If Invasive Lobular Ca and the patient
wants Breast Preserving Surgery (BPS)
358.
Why we shouldget a
CORE needle biopsy FIRST
• One can never conclude the true
nature without a biopsy.
• Management is very different
between malignant and benign
lesions.
• Many benign lesions DO NOT
need surgical intervention.
• Malignant tumors are not all the
same and surgical management
can really be too different.
Fibroadenoma
• is afairly common disease of the young, 15-30
years
• quite often multiple with a dominant one.
• Called the mouse of the breast
• In under 25 with clear cut clinical and US
examination, FNAc or Core biopsy could be
omitted.
• Over 25, core biopsy is mandatory
Atypical Ductal Hyperplasia
(ADH):
•there are more cells than usual in the lining of the
breast duct
• is not a form of breast cancer.
• Rather, it is a marker for women who may have a risk
factor for developing breast cancer in the future.
It is MANDATORY to be excised as it could be just the
edge of a more sinister pathology
367.
Radial scar
• isa growth that looks like a scar when the tissue
is viewed under a microscope.
• It has a central core containing benign ducts.
Growing out of this core are ducts and lobules
that show evidence of unusual changes such as
cysts and epithelial hyperplasia (overgrowth of
their inner lining)
• as diagnosed on radiology and core biopsy has to
be wire localized and excised to get the full
picture
368.
Intraduct papillomas
• Arebenign (non-cancerous), wart-like tumors
that grow within the milk ducts of the breast.
• They are made up of gland tissue along with
fibrous tissue and blood vessels (called
fibrovascular tissue).
• EXCISE if:
• Multiple
• Repeated blood stained discharge
• Core biopsy cannot differentiate between benign
and, the rare, malignant papilloma
369.
Giant fibroadenomas /Benign
Phylloides
• fibroadenoma larger than 5 cm, usually
presenting unilaterally and manifesting as
breast asymmetry or deformity of the breast.
• have to be completely excised
370.
Sclerosing Adenosis
• Isa proliferative lesion that is commonly found in
benign breast biopsies .
• It is a histologically complex entity that consists of
enlarged and distorted lobules, containing
duplicated and crowded acini, with prominent
myoepithelium and stromal fibrosis.
• has to be excised for full histological assessment
to avoid missing a more sinister pathology or very
close monitoring
371.
Summary
• Any benignmass in over 25 years old females has to
be fully assessed
• Even if it proves benign in over 30s, it has to be
removed
• Phylloides have to be excised
• Sclerosing adenosis and Radial scars have to be
excised
• Atypical Ductal Hyperplasia have to be excised
• Major duct excision is to be performed for recurrent
mastistis, repeated blood stained discharge or if the
discharge is so much that it causes social upset to
the patient
THE ANGINAL PAIN
•Typical qualities of anginal pain
• Quality
• − Angina is usually characterized more as
a discomfort rather than pain .
390.
•
Terms frequently usedby patients include
squeezing, tightness, pressure,
constriction, strangling, burning, heart
burn, fullness in the chest, band-like
sensation, knot in the center of the chest,
lump in throat, ache, heavy weight on
chest (elephant sitting on chest), like a bra
too tight, and toothache (when there is
radiation to the lower jaw
)
391.
•
In some cases,the patient cannot qualify
the nature of the discomfort, but places his
or her fist in the center of the chest, known
as the Levine sign
.
392.
•
It is generallynot described as sharp, dull-
aching, knife-like, stabbing, or pins and
needles-like
•
The following additional characteristics are
typically seen
•
. :
393.
•
Angina is typicallygradual in onset and
offset, with the intensity of the discomfort
increasing and decreasing over several
minutes. In contrast, noncardiac pain is
often of greatest intensity at its onset and
often has an abrupt onset and offset
.
394.
•
Angina is aconstant discomfort that does
not change with respiration or position. It is
also not provoked or worsened with
palpation of the chest wall. However, the
presence of a change in pain with
respiration (or position) or pain elicited by
palpation does not exclude angina as the
cause
.
395.
Location and radiation
•
Asnoted above, angina is a referred pain
due to involvement of a neural reflex
pathway via the thoracic and cervical
nerves. As a result, it is not felt in a
specific spot, but is usually a diffuse
discomfort that may be difficult to localize
.
396.
•
Angina is referredto the corresponding
dermatomes (C5-6 and T1-T6) that supply
afferent nerves to the same segments of
the spinal cord as the heart
397.
•
Thus, angina oftenradiates to other parts
of the body, including the upper abdomen
(epigastric), shoulders, arms (upper and
forearm), wrist, fingers, neck and throat,
lower jaw and teeth (but not upper jaw),
and rarely to the back (specifically the
interscapular region
)
398.
•
Radiation to botharms is a stronger
predictor of acute myocardial infarction.
The location and radiation of angina is
usually the same each time. Occasionally,
the location and radiation, but not quality,
may be different after bypass surgery due
to the disruption of the neural innervation
of the heart
.
399.
Provoking factors
•
Angina isoften elicited by activities and
situations that increase myocardial oxygen
demand, including physical activity, cold,
emotional stress, sexual intercourse,
meals, or lying down (which results in an
increase in venous return and increase in
wall stress
)
400.
Pericarditis and pericardialpain
•
Acute pericarditis is diagnosed by the
presence of at least two of the following
criteria
•
Typical chest pain (sharp and pleuritic,
improved by sitting up and leaning
forward
.)
401.
•
Pericardial friction rub(a superficial
scratchy or squeaking sound best heard
with the diaphragm of the stethoscope
over the left sternal border
)
402.
•
Suggestive changes onthe ECG (typically
widespread ST-segment elevation
•
New or worsening pericardial effusion
•
These diagnostic criteria are consistent
with the 2015 European Society of
Cardiology guidelines on pericardial
diseases
) .
403.
•
In atypical presentations,additional
supporting findings include the evidence of
systemic inflammation (eg, elevation of C-
reactive protein) or pericardial
inflammation on an imaging technique
such as pericardial contrast-enhancement
on computed tomography or pericardial
edema and late gadolinium enhancement
on cardiac magnetic resonance imaging
404.
• Patients shouldbe questioned about the
use of cocaine or other recreational drugs,
as they may trigger myocardial ischemia .
405.
• Postprandial painis generally considered
to be gastrointestinal in origin. However, it
may also be anginal, especially in patients
with severe ischemia (eg, left main or
three vessel coronary disease)
406.
•
Timing − Anginaoccurs more commonly
in the morning due to a diurnal increase
in sympathetic tone.
407.
•
Duration and relief− Classic angina is often
relieved with termination of the provoking factor.
Angina generally lasts for two to five minutes. It
is not a fleeting discomfort, which lasts only for a
few seconds or less than a minute, and it
generally does not last for 20 to 30 minutes,
unless the patient is experiencing an acute
coronary syndrome, especially myocardial
infarction.
408.
• Factors thatreduce oxygen demand or
increase oxygen supply will result in relief
of angina. These include cessation of
activity or termination of the provoking
factor, use of nitroglycerin (which is a
venodilator, reducing venous return, and a
coronary artery vasodilator that increases
coronary blood flow), and sitting up (which
reduces venous return and preload).
409.
• Specific chestpain characteristics can be
used to help differentiate cardiac from
noncardiac causes
410.
Associated symptoms
Dyspnea inthe setting of angina may reflect pulmonary congestion due to an
elevation in left ventricular end diastolic pressure related to failure of the
myocardium to relax normally in diastole (as relaxation or lusitropy is energy
dependent
.)
412.
Dyspnoea (breathlessness
)
•
This isan awareness of increased drive to
breathe and is normal on exercise
•
It is pathological if it occurs at a
significantly lower threshold than
expected. Breathlessness is a non-specific
symptom and may be caused by cardiac,
respiratory, neuromuscular and metabolic
conditions, or by toxins or anxiety
413.
ANGINA EQUEVALENT
•
Dyspnoea maybe caused by myocardial
ischaemia and is known as ‘angina
equivalent
•
It may occur instead of, or with, chest
discomfort, especially in elderly and
diabetic patients
.
’
414.
orthopnea and platypnea
•
Orthopnoeais dyspnoea on lying flat and
is a sign of advanced heart failure
•
Lying flat increases venous return and in
patients with left ventricular impairment
may precipitate pulmonary oedema. The
severity can be graded by the number of
pillows used at night, e.g. ‘three-pillow
orthopnoea
’
415.
Paroxysmal nocturnal dyspnoea
•
Paroxysmalnocturnal dyspnoea is sudden
breathlessness waking the patient from sleep It
is caused by accumulation of alveolar fluid
•
Patients may choke or gasp for air, sit on the
edge of the bed and open windows in an attempt
to relieve their distress. It may be confused with
asthma, which can also cause night-time
dyspnoea, chest tightness, cough and wheeze
,
416.
Platypnoea
•
Platypnoea is breathlessnesson sitting
upright. It is much rarer than orthopnoea
and is usually associated with
deoxygenation (platypnoea–orthodeoxia
syndrome). It requires both anatomical
and functional abnormalities
.
417.
•
The anatomical componentis usually an
intracardiac communication, e.g. atrial
septal defect. Platypnoea then develops
when a right-to-left shunt occurs because
of the functional component
.
418.
Palpitation
•
Palpitation is anunexpected awareness of
the heart beating in the chest
•
.
It may be rapid, forceful or irregular, and
described as thumping, pounding,
fluttering, jumping, racing or skipping. The
patient may be able to mimic the rhythm
by tapping it out
.
419.
•
Palpitation may occurin sinus rhythm with
anxiety, with intermittent irregularity of the
heart beat, e.g. extrasystoles, or with an
abnormal rhythm (arrhythmia). Not all
patients with arrhythmia experience
palpitation, e.g. atrial fibrillation often
occurs in the elderly but rarely causes
palpitation
•
Excess fluid inthe interstitial space causes
oedema (tissue swelling). It is usually
gravity-dependent and so especially seen
around the ankles, or over the sacrum in
patients lying in bed. The most common
causes of lower limb swelling are chronic
venous disease and lymphoedema
.
Causes of pittingedema
•
Heart failure •
•
Chronic venous insufficiency
•
• Hypoproteinaemia, e.g. nephrotic syndrome,
kwashiorkor, cirrhosis
•
• Drugs, e.g. NSAIDs, nifedipine, amlodipine,
fludrocortisone • Inferior vena caval obstruction •
Thiamine (vitamin B1) deficiency (wet beriberi) •
Milroy’s disease (unexplained lymphoedema
which appears at puberty; more common in
females
•
Estrogen
)
425.
Syncope
•
Syncope is aloss of consciousness due to
cerebral hypoperfusion. Dizziness may be
due to vertigo or lightheadedness Vertigo
is rarely caused by heart disease.
Lightheadedness, syncope or a feeling of
impending loss of consciousness
(presyncope) may be cardiovascular in
origin.
.
426.
•
The main causesare:
•
• postural hypotension
•
• neurocardiogenic syncope
•
• arrhythmias
•
• mechanical obstruction to cardiac output
427.
•
Mechanical obstruction tocardiac output,
including severe aortic stenosis and
hypertrophic cardiomyopathy, can obstruct
left ventricular outflow causing syncope or
presyncope, especially on exertion when
cardiac output cannot meet the increased
metabolic demand
428.
•
Pulmonary embolism canobstruct outflow
from the right ventricle, and is a frequently
overlooked cause of recurrent syncope.
Cardiac tumours, e.g. atrial myxoma, and
thrombosis or failure of prosthetic heart
valves are rare causes of syncope
.
429.
•
Neurocardiogenic syncope isa group of conditions
caused by abnormal autonomic reflexes. A simple faint
occurs in healthy people forced to stand for a long time
in a warm environment or subject to painful or emotional
stimuli, e.g. the sight of blood. It results from sudden
slow heart rate (bradycardia) and/or vasodilatation.
There may be a prior history of fainting with a prodrome
of lightheadedness, tinnitus, nausea, sweating and facial
pallor and a darkening of vision from the periphery as the
retinal blood supply (the most oxygensensitive part of the
nervous system) is reduced
,
431.
•
Frequent fainting causedby minor stimuli
may be due to malignant vasovagal
syndrome or hypersensitive
•
carotid sinus syndrome (HCSS). In
patients with HCSS, gentle pressure over
the carotid sinus may reproduce the
symptoms by triggering bradycardia
.
432.
•
Arrhythmias can causesyncope or
presyncope. The most common cause is
bradyarrhythmia, due to sinoatrial disease
or to atrioventricular block, i.e. Stokes–
Adams attacks. Drugs, including digoxin,
beta-blockers and rate-limiting calcium
channel blockers, e.g. verapamil, diltiazem
are a common cause of bradyarrhythmia
433.
•
Supraventricular tachyarrhythmias, e.g.
atrialfibrillation, rarely cause syncope.
Ventricular tachycardia often causes
syncope or presyncope, especially in
patients with impaired left ventricular
function
.
434.
•
Postural hypotension isa fall of 20
mmHg in systolic BP on standing. It can
be caused by hypovolaemia,
antihypertensive drug therapy, especially
diuretics and vasodilators (Box 6.7), and
autonomic neuropathy. Postural
hypotension is common in the elderly,
affecting up to 30% of individuals aged
65 years
.
General examination
• Keepprivacy , light , place
your pt to the right hand.
• Look at the patient’s general
appearance.
• Does he look: unwell?
• breathless or cyanosed?
• frightened or distressed?
• Radial pulseExamination and
causes of absent radial pulse .
• ■ Place the pads of your index
and middle fingers over the
right radial artery.
439.
• ■ Assessrate, and rhythm
• ■ Count the pulse rate over
30 seconds; multiply by 2
to obtain the beats per
minute (bpm).
440.
• ■ Todetect a collapsing pulse:
first, check that the patient has no
shoulder or arm pain or restriction
on movement. Feel the pulse with
the base of your fingers, then raise
the patient’s arm vertically above
the patient’s head).
• ■
441.
• Palpate bothradial pulses
simultaneously, assessing any
delay between the two, and any
difference in pulse volume.
• ■ Palpate the radial and femoral
pulses simultaneously, again
noting any timing and volume
differences.
442.
• Use thelarger (brachial, carotid or
femoral) pulses to assess the pulse
volume and character When taking a
pulse, assess:
• • Rate
• • Rhythm
• • Volume
• • Character.
443.
• Record individualpulses as:
• Normal +
• Reduced ±
• Absent –
• Aneurysmal + +
If you are in any doubt about
whose pulse you are feeling,
palpate your own pulse at the
same time. If it is not
synchronous with yours, it is
the patient’s
444.
• Hands andskin Examination sequence
• ■ Look for signs of tobacco staining
• ■ Look for peripheral cyanosis.
• ■ Feel the temperature.
• ■ Check for clubbing
• ■ Look at the nails for splinter haemorrhages
(linear, reddishbrown marks along the axis of the
finger and toenails, thought to be due to
circulating immune complexes.
445.
• ■ Lookat the palmar aspect of the hands for:
• ■ Janeway lesions – painless red spots, which
blanch on pressure, on the thenar/hypothenar
eminences of the palms, and soles of the feet.
• ■ Osler’s nodes – painful raised erythematous
lesions which are rare but found most often
on the pads of the fingers and toes.
446.
• ■ Lookat the palmar and
extensor surfaces of the hands
for xanthomata (yellow skin or
tendon nodules from lipid
deposits).
• ■ Look at the entire skin surface
for petechiae.
447.
The face andeyes Examination
sequence Look:
■ in the mouth for central
cyanosis.
■ at the eyelids for
xanthelasmata (soft yellowish
plaques periorbitally and on
the medial aspect of the
eyelids associated with
hyperlipidaemia).
■
448.
• at theiris for a corneal arcus.
• ■ at the conjunctivae for
petechiae.
• ■ Examine the fundi for
features of hypertension,
diabetes and Roth’s spots
(flame-shaped retinal
haemorrhages with a ‘cotton-
wool’ centre .
449.
• Jugular venouspressure and waveform
• Estimate the JVP by observing the level
of pulsation in the internal jugular vein.
The normal waveform has two main
peaks per cycle, which helps to
distinguish it from the carotid arterial
pulse .The JVP level reflects right atrial
pressure (normally
The precordium
• Examinationsequence
• ■ Explain that you wish to examine the
chest and ask the patient to remove all
clothing above the waist. Keep a female
patient’s chest covered with a sheet as
far as possible.
452.
• ■ Inspectthe precordium with
the patient sitting at a 45°
angle with shoulders
horizontal. Look for surgical
scars, visible pulsations and
chest deformity.
453.
• ■ Placeyour right hand flat over the
precordium to obtain a general impression
of the cardiac impulse).
• ■ Locate the apex beat by lying your
fingers on the chest parallel to the rib
spaces; if you cannot feel it, ask the
patient to roll on to his left side ■ Assess
the character of the apex beat and note
its position.
454.
• ■ Applythe heel of your right hand firmly
to the left parasternal area and feel for a
right ventricle heave. Ask the patient to
hold his breath in expiration).
• ■ Palpate for thrills at the apex and both
sides of the sternum using the flat of your
fingers
455.
auscultation
• Examination sequenceMake sure the room is quiet when you
auscultate. Your stethoscope should fit comfortably with
the earpieces angled slightly forward. The tubing should be
~25 cm long and thick enough to reduce external sound.
• ■ Listen with your stethoscope diaphragm at the:
• ■ apex
• ■ lower left sternal border
• ■ upper right and left sternal borders.
• ■ Listen with your stethoscope bell at the:
• ■ apex
• ■ lower left sternal border.
456.
• ■ Listenover the carotid
arteries (ejection systolic
murmur of aortic stenosis)
and in the left axilla
(pansystolic murmur of mitral
regurgitation).
457.
• At eachsite identify the S1
and S2 sounds. Assess their
character and intensity; note
any splitting of the S2.
Palpate the carotid pulse to
time any murmur. The S1
barely precedes the upstroke
of the carotid pulsation, while
the S2 is clearly out of phase
with it.
458.
• ■ Concentratein turn on systole
(the interval between S1 and S2)
and diastole (the interval
between S2 and S1). Listen for
added sounds and then for
murmurs. Soft diastolic murmurs
are sometimes described as the
‘absence of silence’.
459.
• ■ Rollthe patient on to his left side.
Listen at the apex using light pressure
with the bell, to detect the mid-
diastolic and presystolic murmur of
mitral stenosis
460.
• ■ Askthe patient to sit up and lean
forwards, then to breathe out fully
and hold his breath). Listen over the
right second intercostal space and
over the left sternal edge with the
diaphragm for the murmur of aortic
regurgitation.
461.
• ■ Notethe character and intensity
of any murmur heard.
• ■ Develop a routine for auscultation
so that you do not overlook subtle
abnormalities. Identify and describe
the following:
• ■ the first and second heart sounds
(S1 and S2)
• ■ extra heart sounds (S3 and S4)
• ■ additional sounds, e.g. clicks and
snaps
• ■ pericardial rubs
• ■ murmurs in systole and/or diastole.
463.
Cardiac Apex association
Anabsent apical impulse
• The apex may be impalpable in the
following :
• Obesity.
• Right pneumonectomy with
displacement.
• Pericardial effusion.
• Dextrocardia (palpable on right side of
chest.
464.
Apex association
• Heavingcauses LVH and all its causes
sometimes with fourth heart sound.
• Thrusting / hyperdynamic high left
ventricular volume MR , AR , PDA , VSD .
• Tapping : palpable first heart sound
:MS.
• Displaced and difuse /diskinetic
displaced : MI , dilated cardiomyopathy.
465.
• Double impulse: whith diskinasia
left ventricular aneurysm . without
diskinasia : HOCM.
• Pericardial knock : constrictive
pericarditis .
• Parasternal heave : right
ventricular hypertrophy ASD,
pulmonary HTN , COPD.
• Palpable third heart sound : heart
failure , Severe MR
466.
• MURMURS
• Heartmurmurs are produced by
turbulent flow across an abnormal valve,
septal defect or outflow obstruction.
‘Innocent’ murmurs caused by increased
volume or velocity of flow through a
normal valve occur when stroke volume is
increased, e.g. during pregnancy, in
athletes with resting bradycardia or
children with fever
467.
• Timing Identifythe S1 and S2 sounds.
It may help to palpate the patient’s
carotid pulse while listening to the
precordium.
468.
• Determine whetherthe murmur is systolic or
diastolic:
• ■ Systole begins with the S1 (mitral and tricuspid
valve closure). This occurs when left and right
ventricular pressures exceed the corresponding atrial
pressures. For a short period all four heart valves are
closed (pre-ejection period). Ventricular pressures
continue to rise until they exceed those of the aorta
and pulmonary artery, causing the aortic and
pulmonary valves to open. Systole ends with the
closure of these valves, producing the S2.
469.
• ■ Diastoleis the interval between S2 and S1.
Physiologically it is divided into three phases: ■ early
diastole (isovolumic relaxation): the time from the
closure of the aortic and pulmonary valves until the
opening of the mitral and tricuspid valves ■ mid-
diastole: the early period of ventricular filling when
atrial pressures exceed ventricular pressures ■ pre-
systole: coinciding with atrial systole. Murmurs of
aortic (and pulmonary) regurgitation start in early
diastole and extend into mid-diastole. The murmurs
of mitral or tricuspid stenosis cannot start before
mid-diastole. Likewise, S3 occurs in mid-diastole and
S4 in pre-systole.
470.
• Duration Themurmurs of mitral and
tricuspid regurgitation start with S1,
sometimes muffling or obscuring it, and
continue throughout systole (pansystolic)
(Fig. 6.27). The murmur produced by
mitral valve prolapse does not begin until
the mitral valve leaflet has prolapsed
during systole, producing a late systolic
murmur. The ejection systolic murmur of
aortic or pulmonary stenosis begins after
S1 reaches maximal intensity in mid-
systole, then fades, stopping before S2
471.
• Character andpitch The quality of a
murmur is subjective, but terms such as
harsh, blowing, musical, rumbling, high-
or low-pitched can help. High-pitched
murmurs often correspond with
highpressure gradients, so the diastolic
murmur of aortic regurgitation is
higher-pitched than that of mitral
stenosis
472.
• Intensity Describeany murmur according to
its grade of intensity. Diastolic murmurs are
rarely louder than grade 3. The intensity of a
murmur does not correlate with severity of
valve dysfunction; for instance, the murmur
of critical aortic stenosis can be quiet and
occasionally inaudible. Changes in intensity
with time are important, as they can denote
progression of a valve lesion. Rapidly changing
murmurs can occur with infective endocarditis
because of valve destruction.
473.
• Location Recordthe site(s) where you
hear the murmur best. This helps to
differentiate diastolic murmurs (mitral
stenosis at the apex, aortic
regurgitation at the left sternal edge),
but is less helpful with systolic
murmurs, which are often loud over all
the precordium
474.
• Radiation Murmursradiate in the direction of
the blood flow to specific sites outside the
precordium. Differentiate this from location.
The pansystolic murmur of mitral
regurgitation radiates towards the left axilla,
the murmur of ventricular septal defect
towards the right sternal edge, and that of
aortic stenosis to the aortic area and the
carotid arteries.
475.
• Benign flowmurmurs : innocent murmur
• Effect of posture on murmurs : standing
increases the murmur of MVP and HCM .
• Squatting and passive leg raising decrease the
murmur of MVP and HCM , whilst increasing
most other murmurs VSD , AR ,AS, MR and
pulmonary regurge
• Effect of respiration on mumurs :
accentuates right sided murmurs where as
held expiration accentuates left sided
murmurs