History
1 Personal details(Identification)
2 Chief Complaint
3 History of present illness
4 Past Medical/surgical history
5family History
6-Personal
7 Social History
8 Treatment
History. 9- Misc.
Respiratory Examination-symptom
--Duration:- Afew days---May be due to
common cold
-Several weeks:- Some serious
illness
-- Timing/Diurnal variation:-
-Dry cough in night(2-4am)-May be
early symptom of Asthma
-Bouts of cough lasting for
several minutes---- ?
Asthma
--Aggravating factor:- Dust, Pollen, Cold air, Viral
infection etc
--Character:- Bovine cough---- Vocal cord palsy
Respiratory Examination- Symptoms
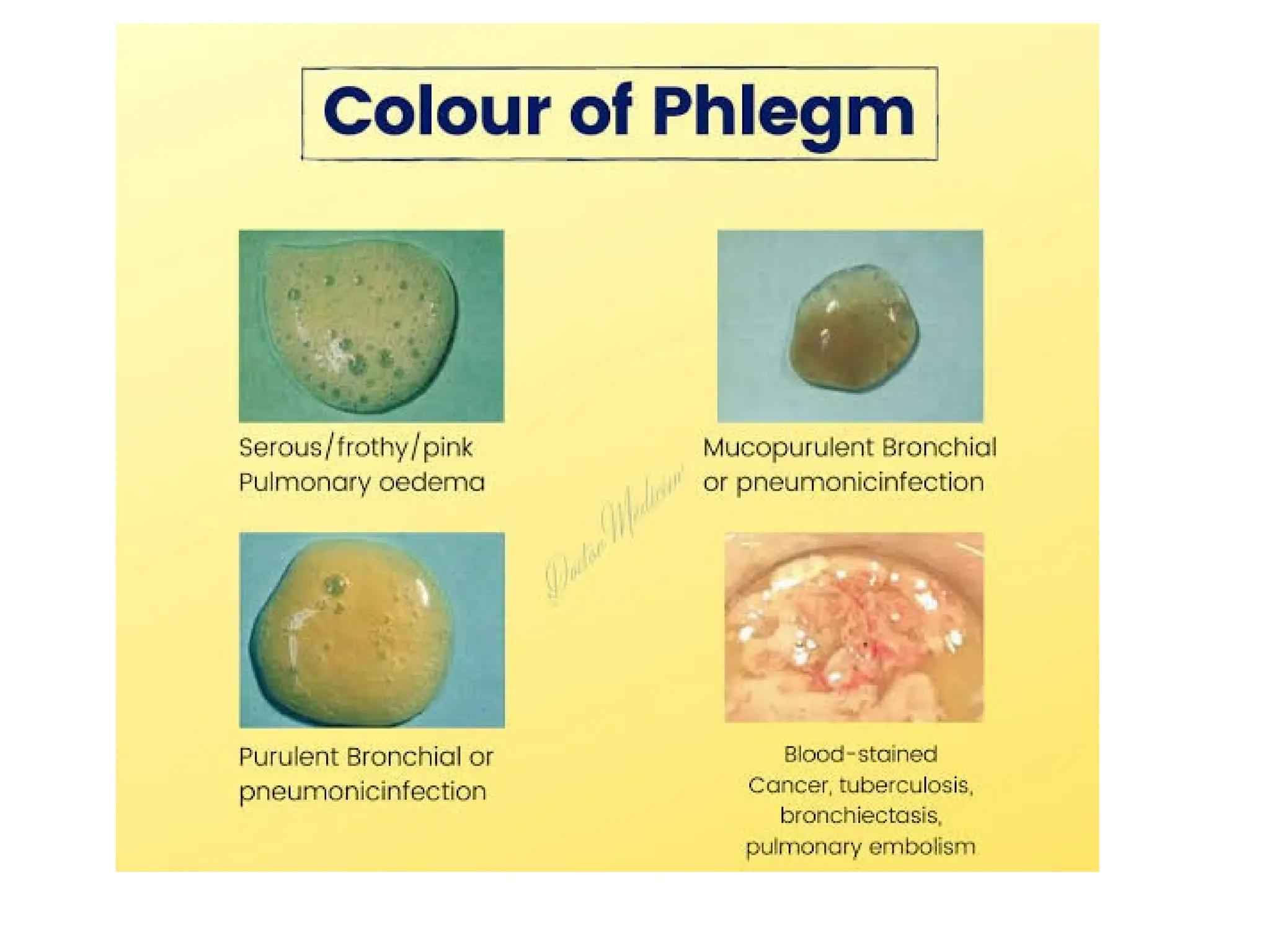
Characterof sputum:-
Mucoid (clear & white):-Bronchitis, Asthma,
COPD
- Black particles in sputum---These are black
inhaled soot.
-Purulent or mucopurulent (Yellow, green or
brown)- Indicates bacterial infection. Some times
eosinophillia may give a purulent appearance to
the sputum without any infection
-Rusty- Pneumococcal pneumonia.
Smell:- Foul smell- Bronchiactasis, Lung
abscess.
Respiratory Examination- Symptoms
Dyspnoea:-Uncomfortable awareness of
breathing.
Pathological Dyspnoea:- Uncomfortable
awareness of breathing which is
disproportionate to the degree of exertion.
Severity:-
16.
Respiratory Examination-Symptoms
Grading ofDyspnoea:-The MRC Dyspnoea scale
Grade Impact (related activity)
Grade-1 Not troubled by breathlessness except on strenuous
exercise
Grade-2 Short of breath when hurrying on the level or
walking up a slight hill.
Grade-3 Walks slower than most people on the level. Stops
after a mile or so, or stops after 15 minute walking
at own pace
Grade-4 Stops for breath after walking about 100 yards or
after a few minutes on leveled ground
Grade-5 Too breathless to leave the house, or breathless
while undressing.
19.
Respiratory Examination- Symptoms
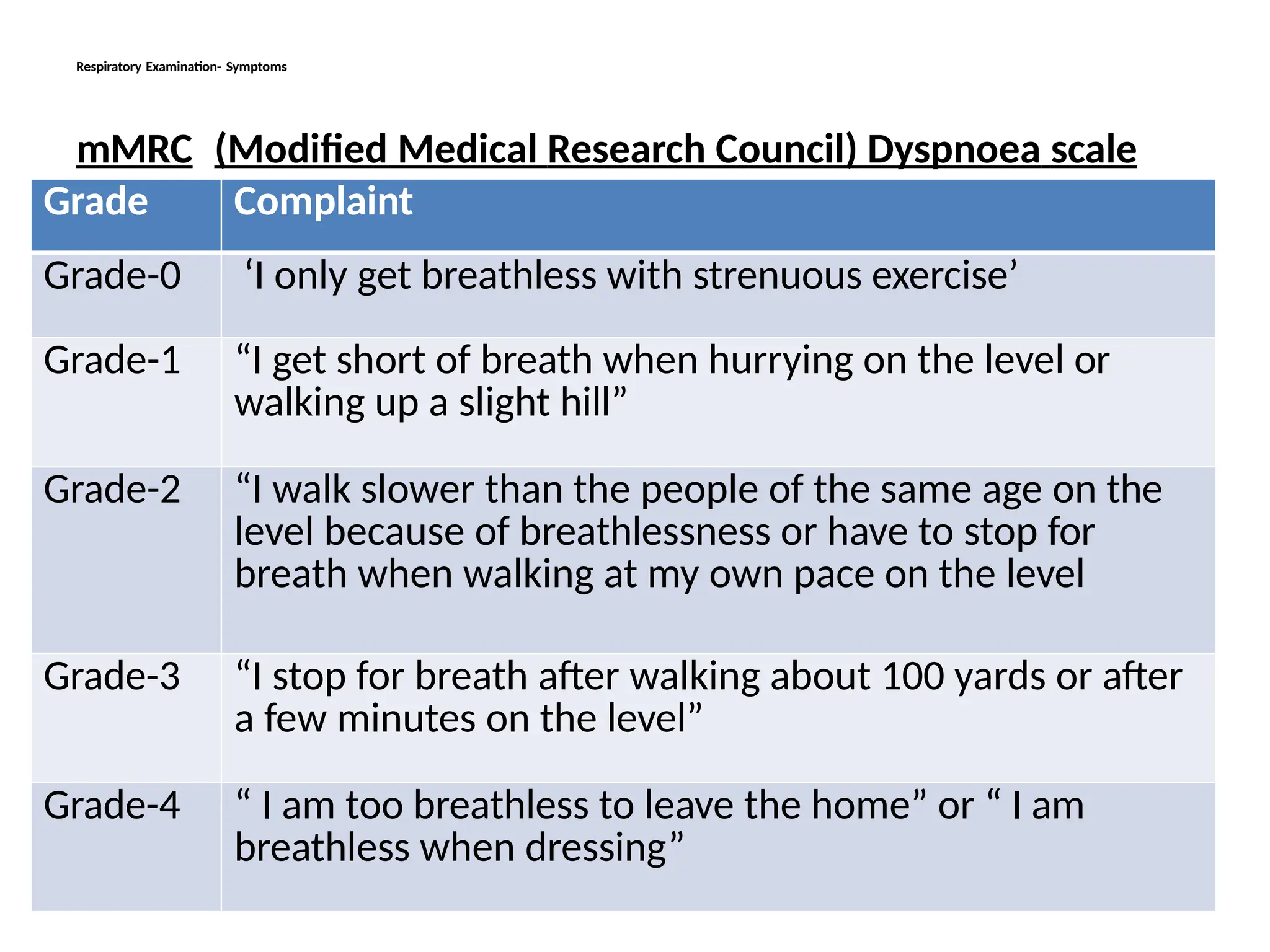
mMRC(Modified Medical Research Council) Dyspnoea scale
Grade Complaint
Grade-0 ‘I only get breathless with strenuous exercise’
Grade-1 “I get short of breath when hurrying on the level or
walking up a slight hill”
Grade-2 “I walk slower than the people of the same age on the
level because of breathlessness or have to stop for
breath when walking at my own pace on the level
Grade-3 “I stop for breath after walking about 100 yards or after
a few minutes on the level”
Grade-4 “ I am too breathless to leave the home” or “ I am
breathless when dressing”
20.
Respiratory Examination- Symptoms
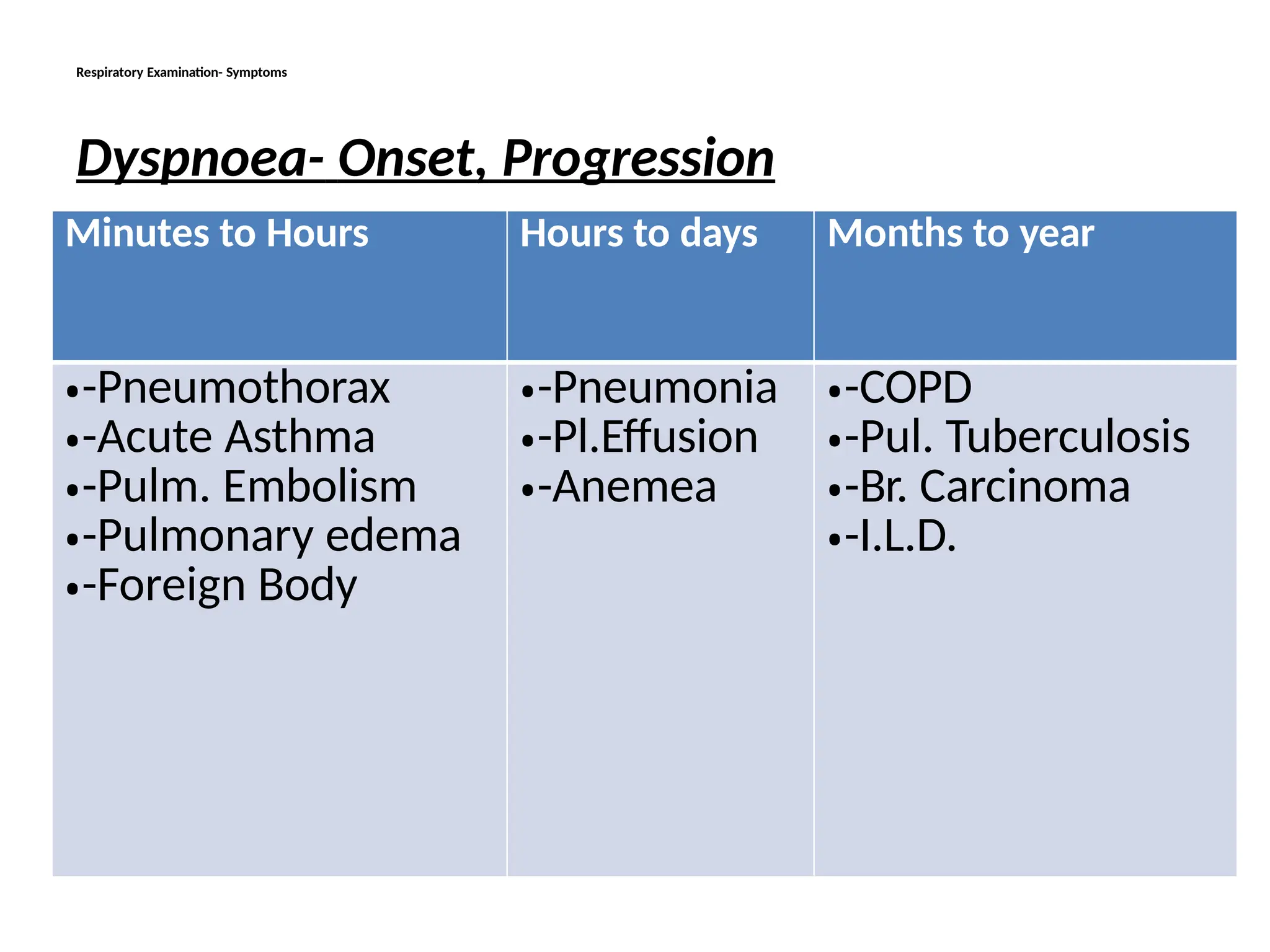
Dyspnoea-Onset, Progression
Minutes to Hours Hours to days Months to year
•-Pneumothorax
•-Acute Asthma
•-Pulm. Embolism
•-Pulmonary edema
•-Foreign Body
•-Pneumonia
•-Pl.Effusion
•-Anemea
•-COPD
•-Pul. Tuberculosis
•-Br. Carcinoma
•-I.L.D.
21.
Respiratory Examination-Symptoms
Dyspnoea- Variability,Aggrevating/ Relieving factors:-
-Good days & Bad days:- Improves on weekend
and holidays- Occupational Asthma
-Time of aggravation:-At night or early morning----
Asthma
- Awakens the patient from sleep:-
Asthma, Pulmonary edema, Severe COPD
-Brought by lying down position (Orthopnoea)
– Heart failure, Severe COPD
-Precipitated by- Exercise, exposure to dust, smoke,
pollen etc:- Asthma
22.
Respiratory Examination-Symptoms
Dyspnoea:- Associatedproblem:-
A-With Chest Pain
Central(Retrosternal) &
non pleuritic pain
Non Central
with Pleuritic
pain
•Myocardial Infarction
• Massive
Pulmonary
embolism
•Trauma
•Pleurisy
•Pneumo thorax
•Pneumonia
•Pulmonary Infarction
Respiratory Examination-symptoms
Non centralchest pain:-
-Costo condritis
-Bornholm disease- Pleurisy & myalgia
due to Coxsackie B virus infection
-Spinal nerve root involvement-
Vertebral disease, Herpes zoster
-Pleurisy –due to Tuberculosis,
Pneumonia, Malignant invasion, Pulmonary
infarction
- Pneumothorax
-Muscular
27.
Respiratory Examination-symptoms
Any partof Chest:-
-Trauma
-Cellulites
-Abscess
C-Character Of Pain/ Aggravating & relieving
factors-
Pleural Pain:- Localized, sharp, stabbing
& aggravated by Deep breathing & coughing
Pain due to chest wall disorders- Pain
may be similar to Pleural pain but is also
aggravated by movement & there is local
tenderness.
28.
Respiratory Examination-symptoms
Central ChestPain:- May be sharp,
Stabbing, piercing, compressing, severe or
constant dull aching. Pain of trachiatis and
pericarditis are exaggerated by deep
breathing. Esophageal pain may be related to
food. Myocardial pain may aggravate by
exertion.
D-Radiation of pain:- cardiac pain radiates to
neck, jaw, arm, back or upper abdomen. Pain
of diaphragmatic pleurisy radiates to tip of
shoulder
29.
Respiratory Examination-symptoms
5- Hemoptysis:-Coughing up of blood.
A- Duration
B-Amount
C-Character of blood- fresh/Altered
D-Association- Epistaxis, Malena
Important causes of hemoptysis:- Tuberculosis,
Bronchial carcinoma, Pulmonary infarction,
Bronchiactasis, Mitral stenosis, Acute
bronchitis, Pulmonary embolism, Good
pasture syndrome.
30.
Respiratory Examination-symptoms
B- Amountof Blood:- Streaks of blood with
sputum can came from upper airway disease
Massive hemoptysis:- 100-600ml blood in
24 hours (According to different literatures)
31.
Respiratory examination-symptoms
C &D- to differentiate between hemoptysis &
hematemesis
Feature Hemoptysis Hematemesis
Preceded by Cough Nausea
History of Cough Abdominal discomfort
Color Bright red , frothy Altered, Coffee colored
Melena Absent Present (Requires more than
50ml bleeding proximal to
Cecum
Food particle Absent May be present
pH Alkaline Acidic
32.
Respiratory Examination-symptoms
• BrightRed Blood is also present if bleeding is
from Pharynx & esophagus
• Dark red blood with clot may be present in
case of Profuse bleeding from esophagus
& peptic ulcer
6-Fever:- It indicates infection.
-High fever is present in
pneumonia
-Evening/night fever with sweating is
found in tuberculosis.
33.
Respiratory Examination-symptoms
7-Wheeze :-Audible ronchi- some times patient
complain that musical sound comes from
his/her breath
8- Stridor:- noisy breathing due to large air way
narrowing (Larynx, Trachea or main bronchus)
usually during inspiration.
34.
Respiratory System-General Exam
Importantpoints to be noted during General
Examination
1-Pallor/ Polycythemia
2-Cynosis
3-Clubbing
4-Edema
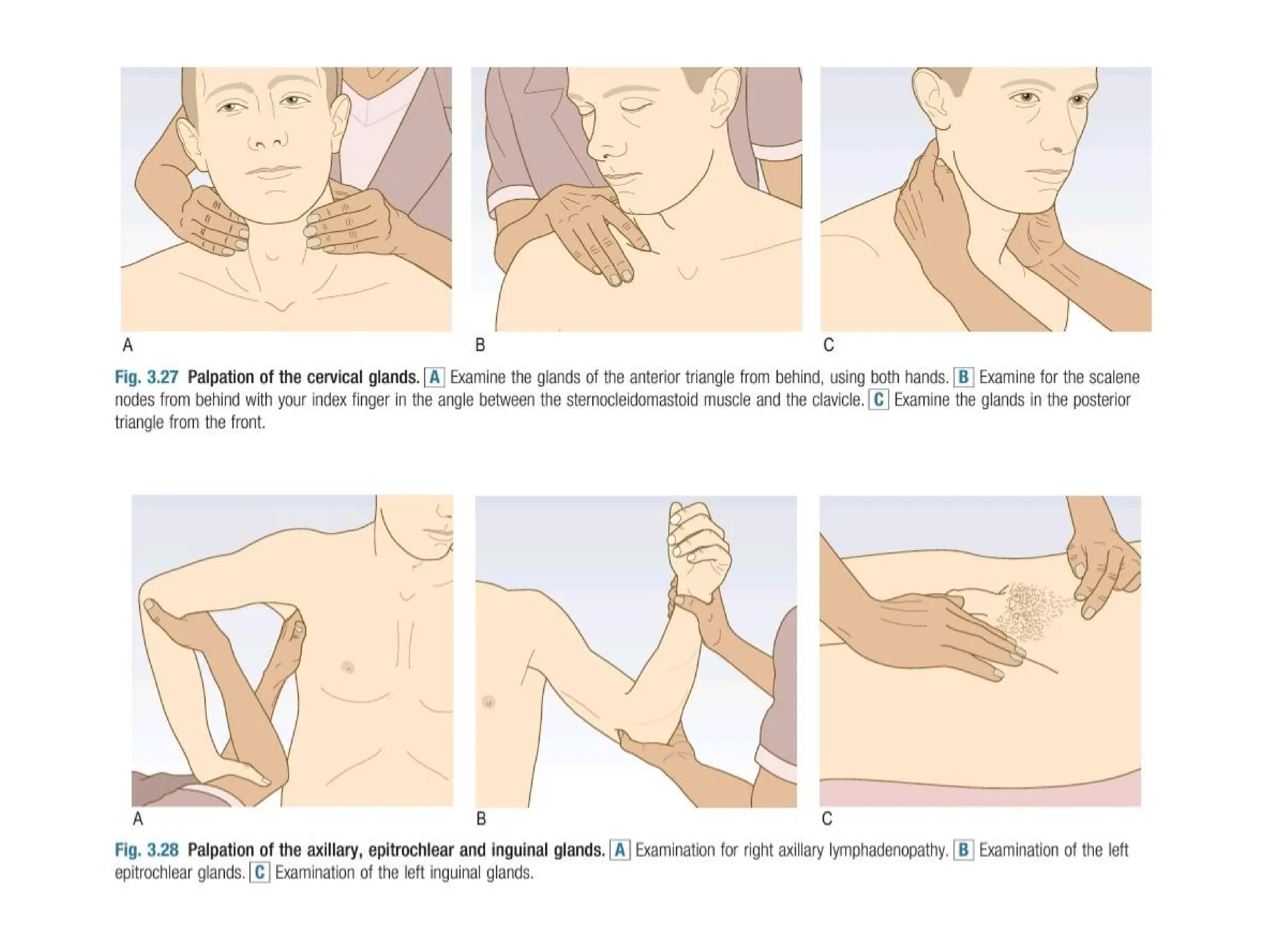
5-Cervical
lymph
adenopat
Respiratory System-Inspection
1- Inspection:-
A-Dyspnoea:- whether the patient is Dyspneic or
not ?
-Patient is said to be dyspnoec if accessory
muscles of respiration are in action
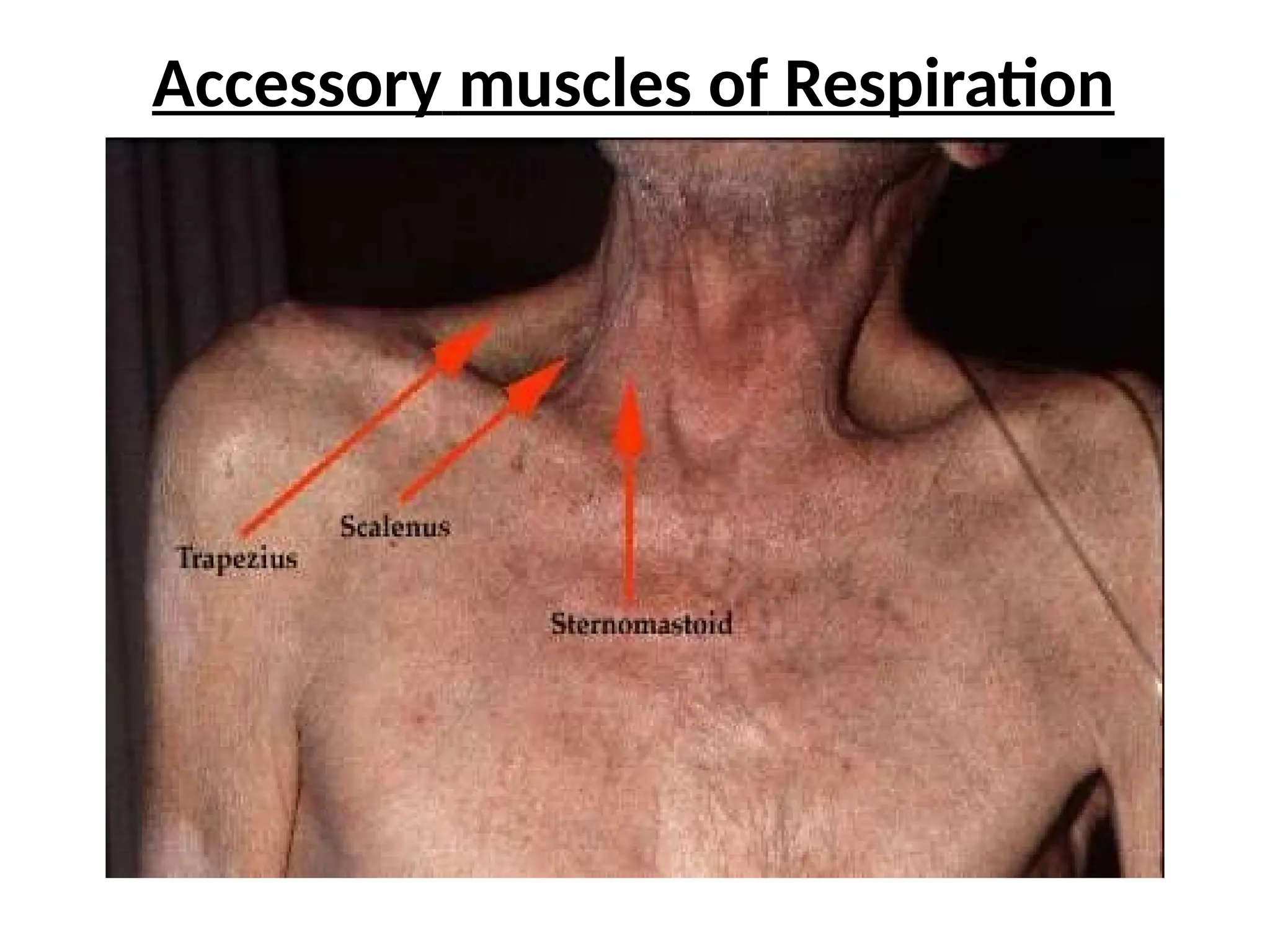
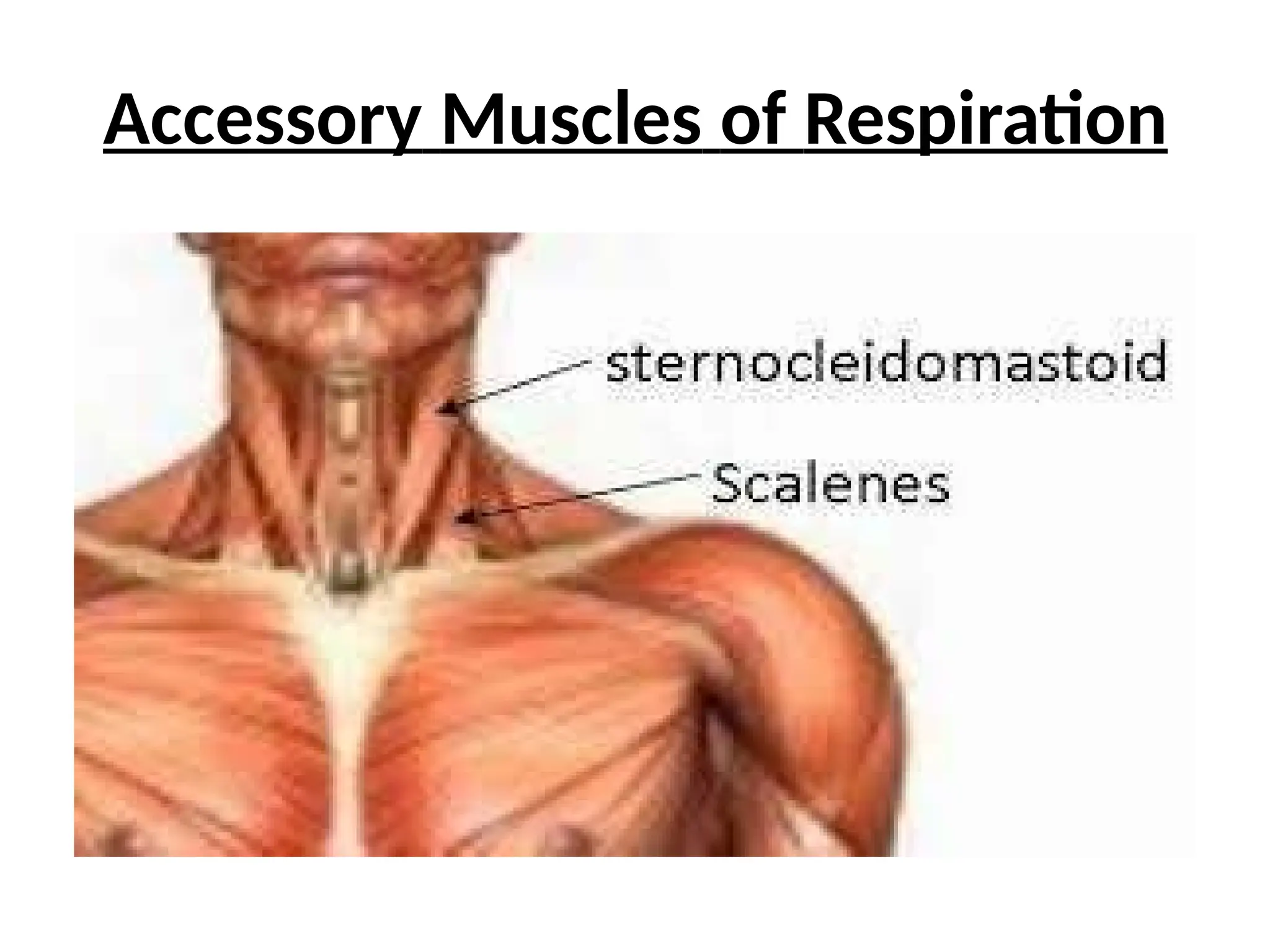
Accessory muscles of Respiration:-
- Ala nasi
-Sternocleidomastoid
-Scalene
- Trapezeous
B-Respiratory Rate &Rhythm
The normal respiratory rate in adult during rest is
12-20/ minute The respiration :pulse ratio is 1:4.
Tachypnoea:- Increased respiratory rate
above 20/ minute.
Hyperventilation:- Increased rate of
breathing at rest so that body eliminates more
carbon dioxide than it produces. This leads to
hypocapnia leading to respiratory alkalosis
Cause- Psychological stress, anxiety, panic
disorder, high altitude and respiratory illness like
Asthma, Pneumonia etc,
49.
--
Hyperpnoea:- Increase inrate of
respiration which is proportional to the
increase in metabolic rate.
Cheyne Stoke Respiration:- There is cyclic
increase & decrease in respiratory effort and
rate with a short period of complete apnea.
Causes:- Severe Heart failure
- Narcotic poisoning
-Neurological disorder
- Elderly during sleep
50.
--
Kussmaul Breathing:-Deep and
laboredbreathing. It is respiratory
compensation for a metabolic acidosis
Cause:- Severe
metabolic acidosis
-Diabetic keto
acidosis
- Renal
Failure (Uremia)
52.
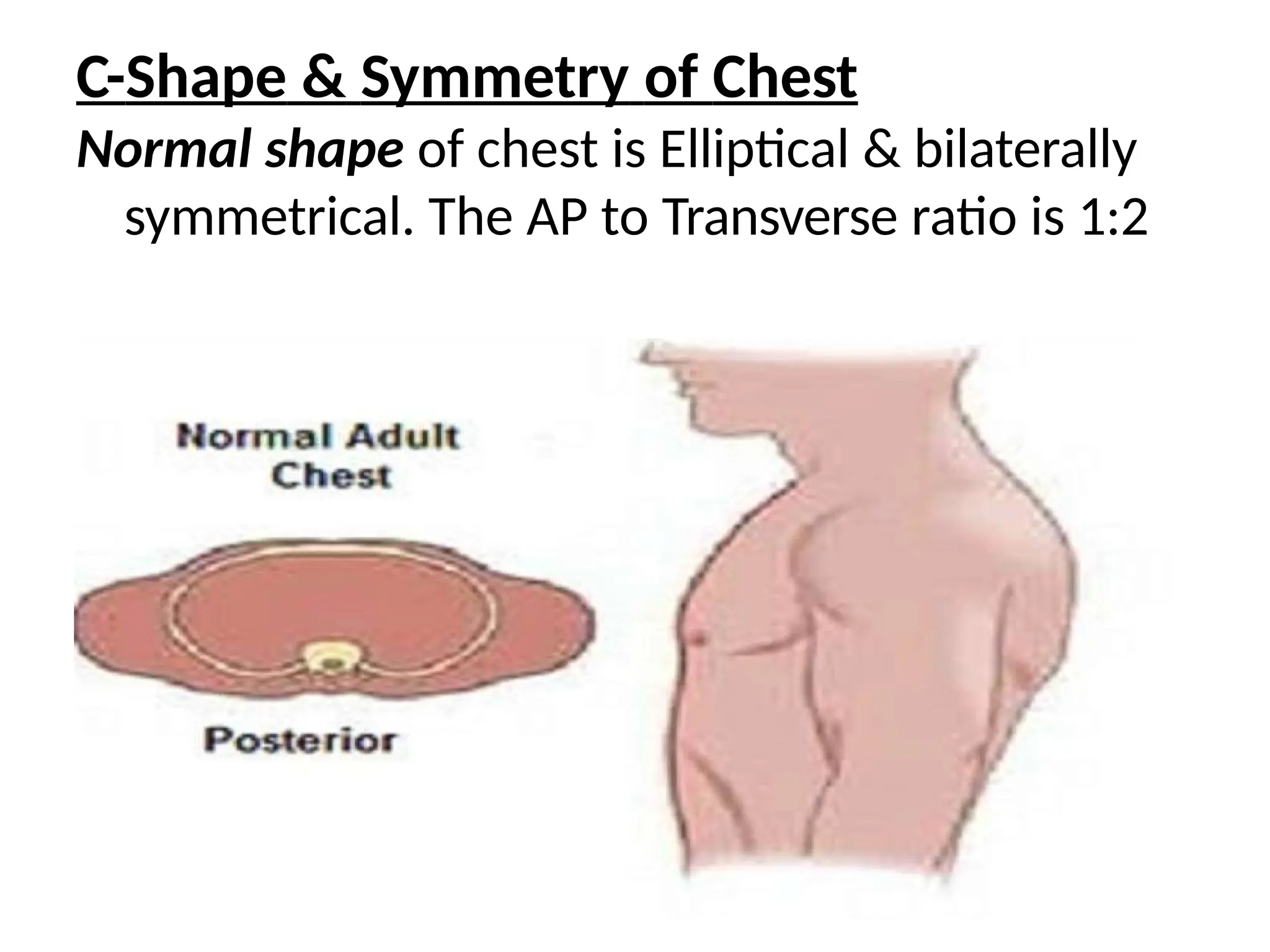
C-Shape & Symmetryof Chest
Normal shape of chest is Elliptical & bilaterally
symmetrical. The AP to Transverse ratio is 1:2
53.
Abnormal shape &symmetry of chest
Barrel Chest:-AP diameter of chest increases
and the shape of chest becomes barrel like
from normal elliptical.
Found in Emphysema, COPD
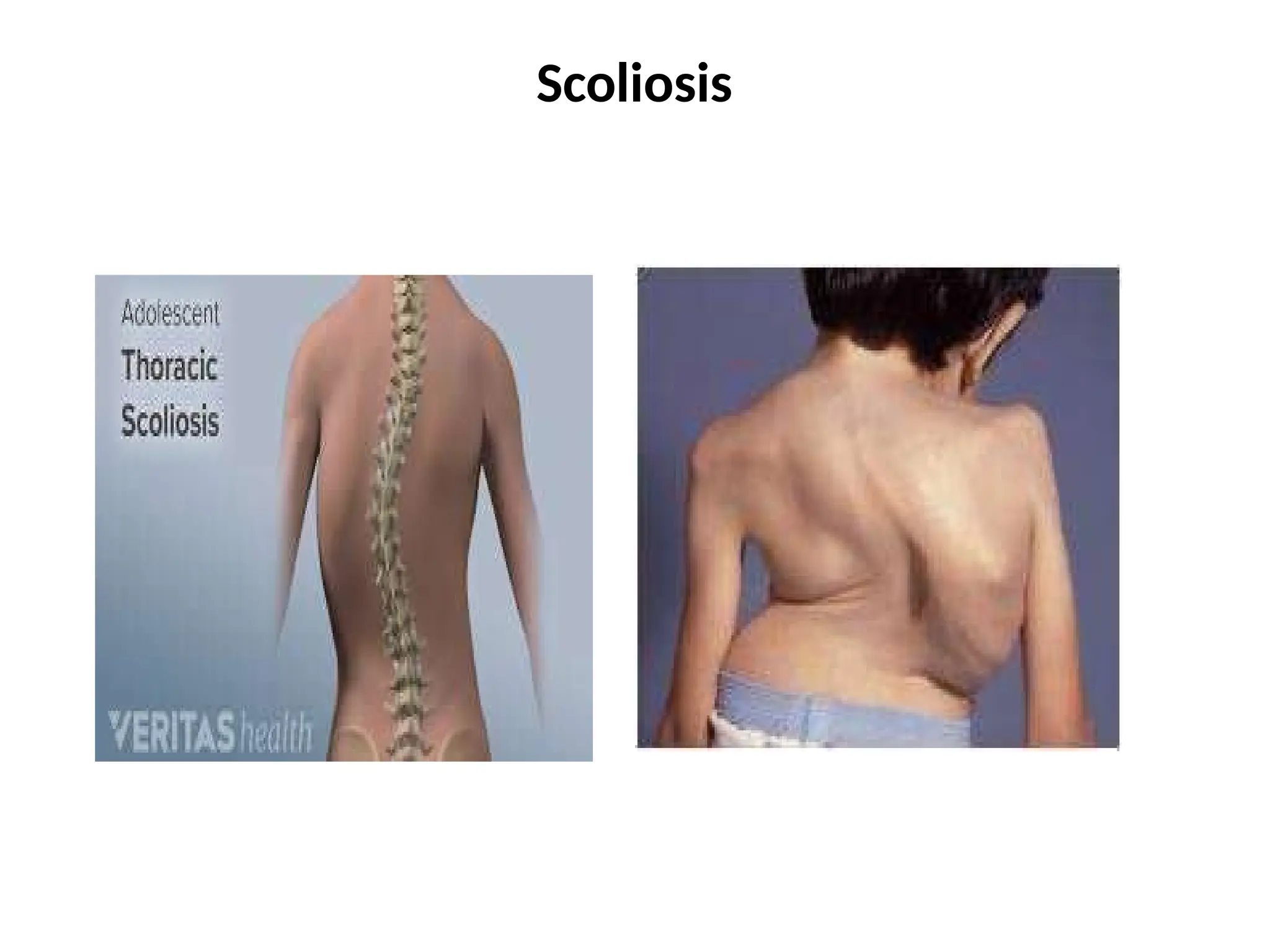
Kyphosis, Lordosis, Scoliosis
-Theseare primarily deformity of vertebral
column
-They may reduce ventilatory capacity of lung
and increase work of breathing
-The position of trachea and Apex beat may
change without any abnormality
--
Harrisons Sulcus:- SymmetricalHorizontal groove
above the costal margin which are themselves
usually everted
Cause:- in drawing of ribs due to respiratory
diseases in child hood
--
I-Movement of chest:-Normally the movement
of chest is bilaterally symmetrical. If the
movement appears to be diminished on one
side, that side is likely to be the side of chest
pathology
- Paradoxical Respiration:- Thorax &
abdomen moves in opposite direction
( Normally the move in same direction)
Cause:- Paralysis of Diaphragm
68.
--
Flail Chest:- Infracture of multiple
ribs, there in a paradoxical movement of the
fractured part( Inwards during inspiration &
outwards during expiration)
J-Visible pulsations:- Apex Beat
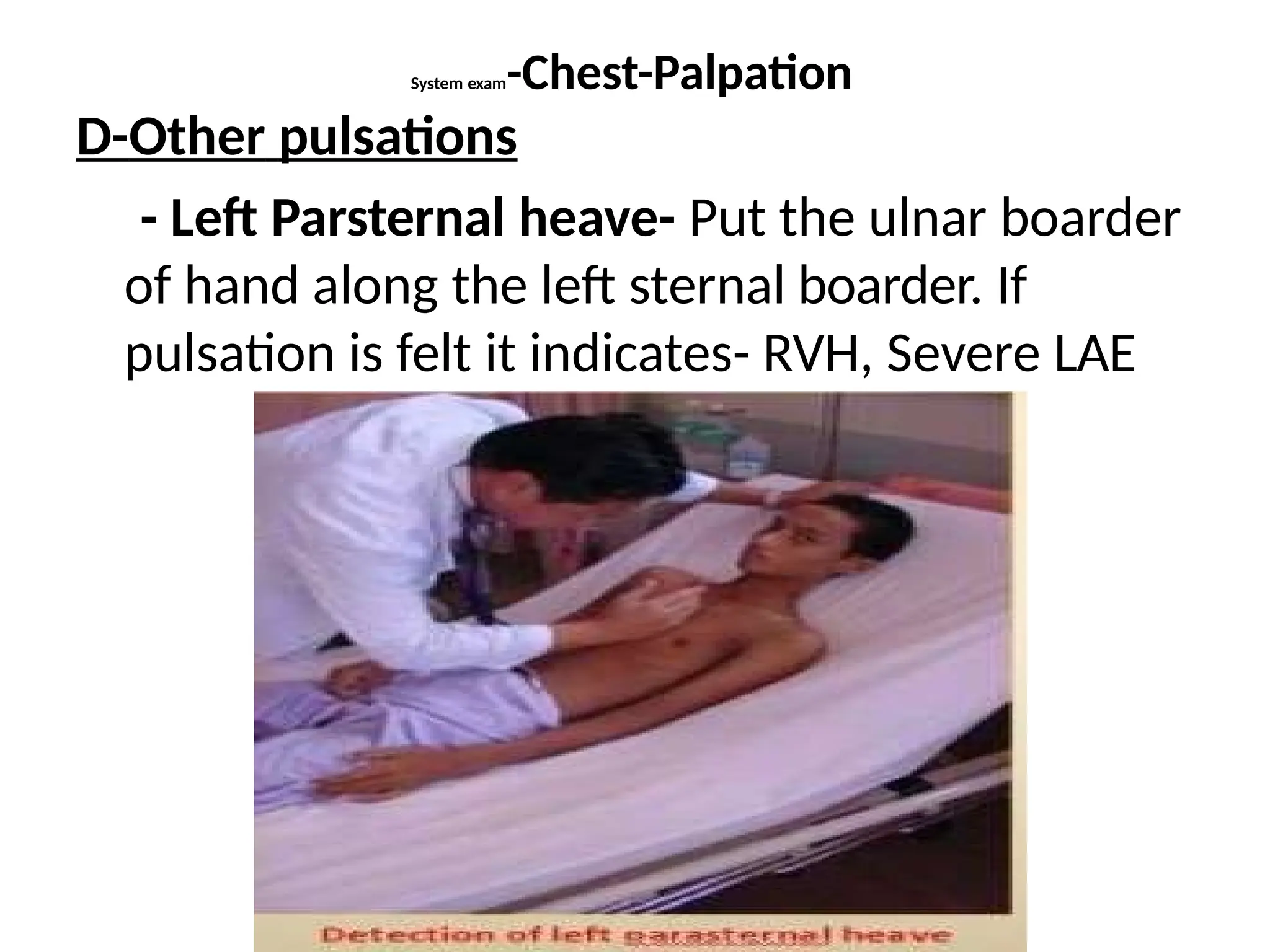
- Left Parasternal
area
-Epigatrium
--
Apex beat:- Thisis the outmost and down most point of
definite cardiac pulsation . In normal situation it is
visible in left 5th intercostal space just medial to mid
clavicular line.
Left parasternal pulsation:- pulsation just to the left of
sternum. It is found in cases of Right Ventricular
hypertrophy.
Epigastric pulsation: Pulsation in epigastric region of
abdomen
-Causes:- Pulsation of Aorta in thin person
- Aneurism of Abdominal aorta
-Right Ventricular Hypertrophy.
- Pulsatile liver in Tricuspid
Regurgitation
71.
System Examination -Chest
2-Palpationof Chest
Confirm the findings of Inspection
A-swelling & Tenderness
B-Lymph Nodes
C- Position of Trachea & Apex beat
D-Other Pulsations- Left parasternal, Epigastric
E-Chest Movement
F-Chest Expansion
G-tactile vocal Fremitus
72.
System exam-Chest-Palpation
A-Swelling andtenderness-
- Local mass
-Abscess
-Musculo skeletal tenderness
B- Lymph nodes:- Spread of malignancy,
Tuberculosis
-Cervical
-Supraclavicur
-Axillary
73.
System exam-Chest-Palpation
C-Trachea &Apex Beat:-( Position)
Normal Trachea:- Slightly deviated to Right.
Normal apex beat:- Left 5th intercostal space
just medial to mid clavicular line.
System exam-Chest-Palpation
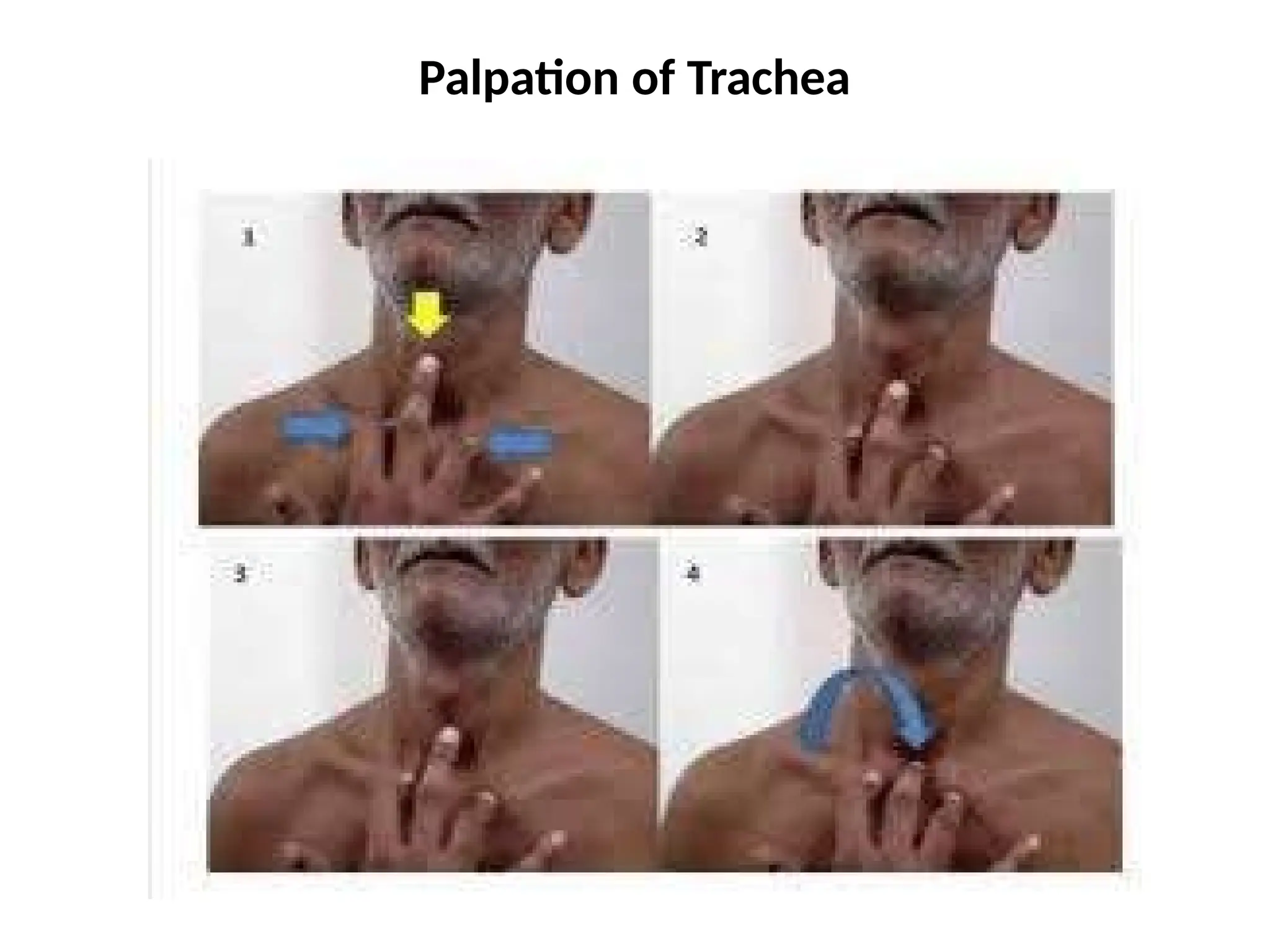
Method ofpalpation of Trachea:-
-Keep the head of patient slightly flexed
-Put index & ring fingers on sternal ends of
clavicles
- Palpate Trachea with middle finger. Try to
insinuate the middle finger on both sides of
trachea alternately. It will be difficult to
insinuate the finger on the side of deviation of
trachea where as it can be easily insulated on
the opposite side
76.
System exam-Chest-Palpation
Method ofPalpation of Apex beat:-
-First place the palm over precordium. It will
give idea about the intercostal space in which
there is apical pulsation
- Now put the ulnar boarder of hand in that
intercostal space
- Finally locate the apex by finger tip
- While keeping the finger tip on the apex from
other hand count the intercostal space in
which it is located .
System exam-Chest-Palpation
Causes ofshift of Trachea & Apex Beat:-
Only Trachea- Fibrosis or Collapse on the same side
Only Apex:- Thoracic deformity, Left or Right
ventricular hypertrophy, Dextrocardia, Small
pleural effusion on opposite side.
Sift of both Trachea & Apex:-
On the same side:- - Fibrosis of lungs
- Collapse of lungs
On the opposite side:- Pleural effusion
- Pneumo thorax
- Hydro
Pneumothorax
System exam-Chest-Palpation
- Ifthe pulsation is felt on the tip of the finger
as something is pushing down-cause-RVH
- If pulsation is felt on the pulp of finger as some
thing is pushing upwards- Cause- Aortic
pulsation. (May be either the person is lean &
thin or there is an aneurism of abdominal
aorta.)
System exam-Chest-Palpation
Chest movementis compared on both side in
upper & lower part of chest both anteriorly
and posteriorly
There in no cause of increase of
chest movement
If chest movement is decreased on
any side & area ,than that side or area of
chest is likely to be pathological
88.
System exam-Chest-Palpation
F-Chest Expansion:-It is expansion of the total
chest and is measured by measuring tape at
the level of 4th ICS in males and just below
breasts in females during full expiration & full
inspiration
89.
System exam-Chest-Palpation
Normal chestexpansion is 5-8cm. Below 2 cm. it
is definitely abnormal.
Causes of decreased expansion:- Any
diffuse broncho pulmonary disease like-
-Emphysema
-Bronchial asthma
-Ankylosing spondylitis
-Diffuse pulmonary
fibrosis
90.
Chest-Exam-Palpation
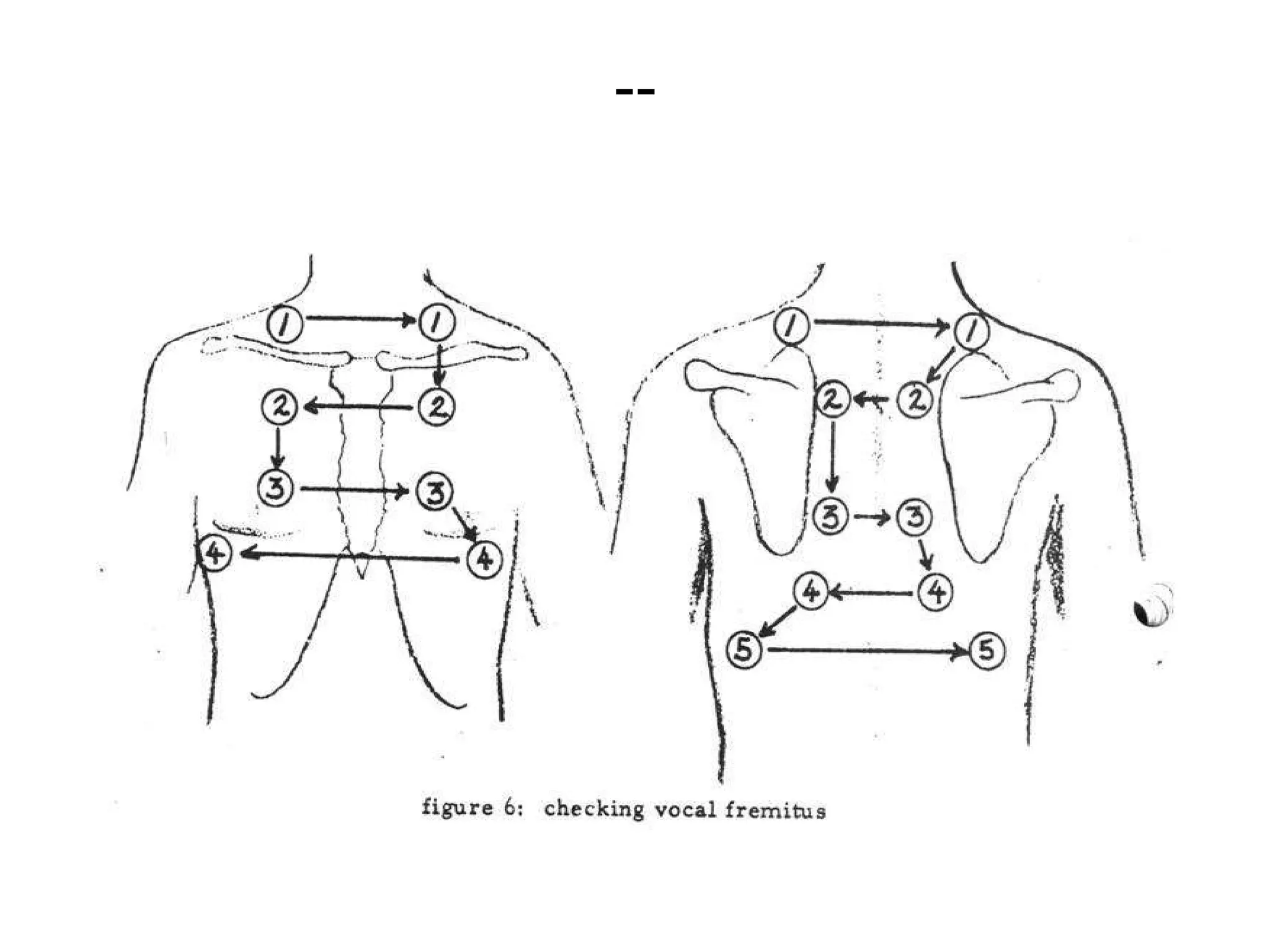
G-Tactile vocal fremitus:- It is the vibration
transmitted to the chest wall from the vocal
cord.
-The patient is asked to say one-one-one
or ninety nine- ninety nine and vibration on
the chest wall is felt by the ulner boarder of
hand. The vibration is compared in
corresponding areas of two sides of chest
Chest Exam-Palpation
Causes ofIncreased Vocal fremitus:-
Localized:- -Consolidation
-Large Empty Cavity with patent
bronchus
-Open type of Pneumothorax
( Broncho pleural fistula)
- Collapse with patent
bronchus
- Fibrosis pulling the major
bronchus near the chest wall
- Above the level of Pleural
effusion
95.
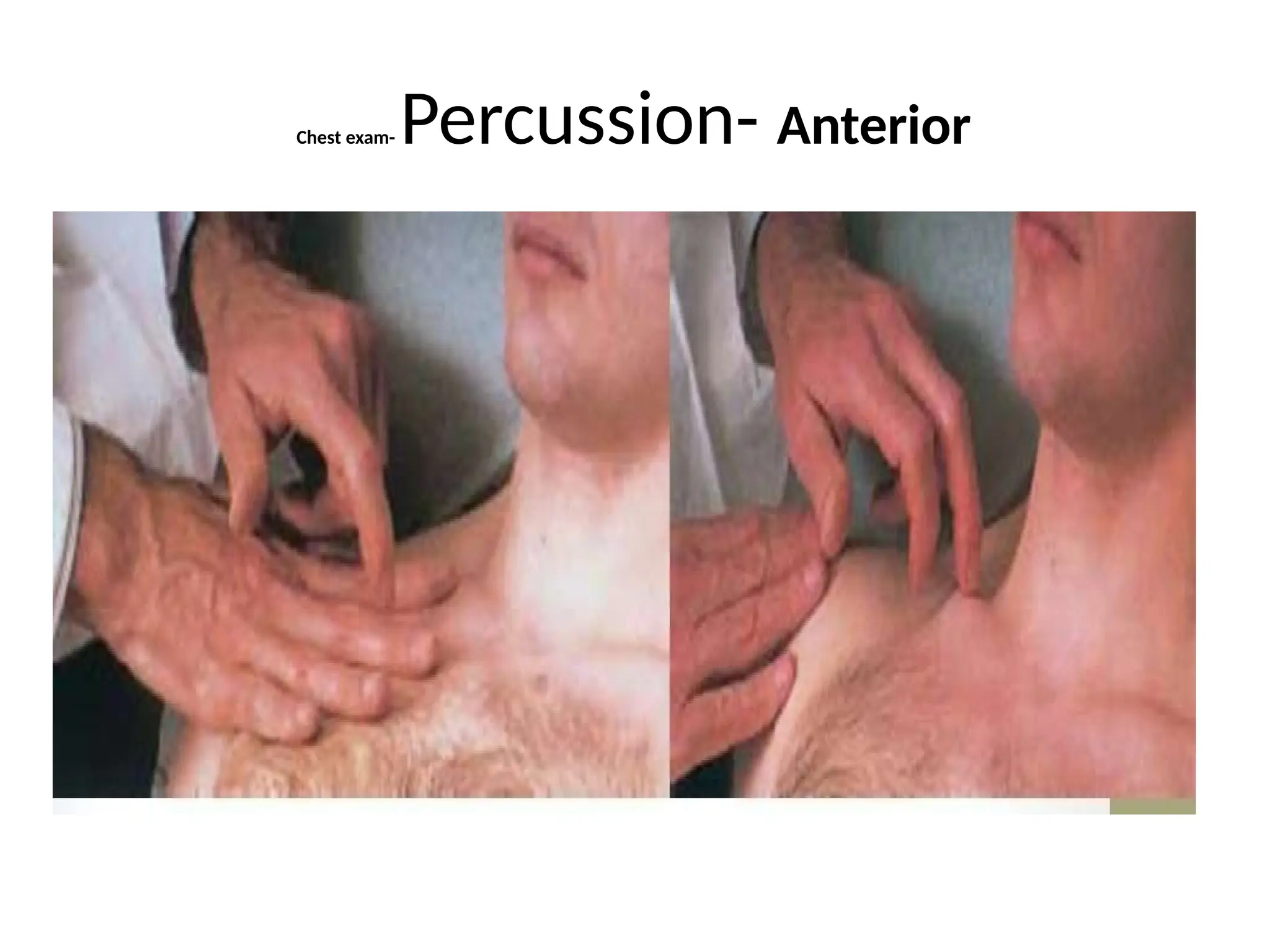
3-Percussion
Percussion is amethod of tapping on a surface to
determine the underlying structure. If air is
present under the surface it gives a resonant
note. If there is solid or liquid, Dull or stony dull
note is produced.
- On bone like clavicle direct percussion (Without
placing pleximeter) is done.
- On other areas middle finger of one hand is placed
firmly in contact of the surface (called
pleximeter) and is tapped by middle
finger (Plexor) of the other hand by action of
wrist)
96.
Chest Exam- Percussion
Areasof percussion:-
Anterior- Clavicle (Direct Percussion)
-Below clavicle:- 2nd to 6th ICS
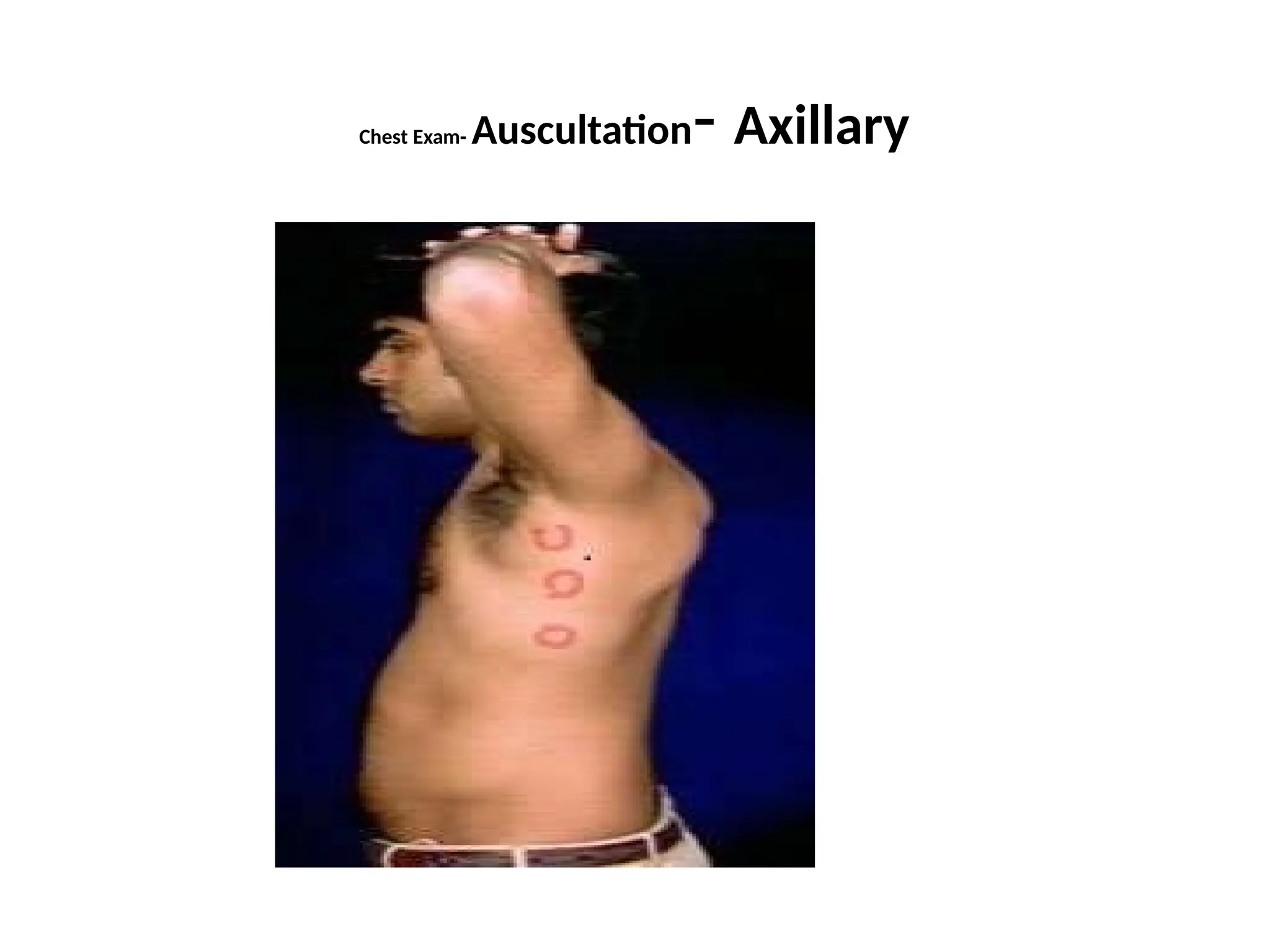
Lateral (Axillary)- 4th to 7th ICS
Posterior- on Trapezius
- Supra scapular
- Inter scapular
-Infra scapular- up to 9th ICS
Chest Examination- Percussion
Observationin percussion:-
-Percussion note on normal Lungs- Resonant.
- Liver dullness starts- 5th ICS in front, 7th ICS in
axilla and 9th ICS posteriorly
- Cardiac dullness is present in 3rd to 5th ICS
anteriorly
Chest Examination-percussion
Tidal Percussion:-percuss down the back of
chest till the liver dullness starts. Percuss with
full expiration & full inspiration. Normally during
inspiration the dullness goes down. This is
because of downward movement of diaphragm
during inspiration
- Loss of tidal percussion:-
-Paralysis of diaphragm
-Supra diaphragmatic pathology
like pleural effusion
Chest Examination- Auscultation
Positionof Patient:-
-It is better to examine the patient in sitting or
standing position
-A full phase of breathing ( full inspiration + full
expiration should be heard.
Anterior Chest Examination:- Keep both arm on side
of patient
Axillary Examination:- Keep both hand of the
patient on his/her head
Posterior Chest Examination- Place right hand of the
patient on left shoulder and left hand on right
shoulder of the patient
Chest examination- Auscultation
A-BreathSound:- (Production)- Breath sound is
produced by vibration of vocal cords due to
turbulent flow of air through the
larynx(Bronchial Sound). As this sound passes
through the lung tissue, some of the higher
frequencies are selectively filtered out and the
sound becomes quieter. We hear this modified
sound as vesicular breath sound through the
stethoscope placed on the chest wall
Chest Examination- Auscultation
Characterof Breath Sound:-
Auscultation within 2-3 cm from midline should
be avoided as stethoscope may pick up sound
transmitted directly from trachea or main
bronchus. Here a mixed quality of sound ( bronco
vesicular or bronchial)may be heard in normal
condition.
Main Types of Breath Sound:-
a) Vesicular
b) Bronchial
c)Broncho vesicular. (Mixed
Character. Usually near midline of chest)
Chest Exam- Auscultation
VesicularBreath Sound Bronchial Breath Sound
1-The Expiratory phase is
shorter than the inspiratory
phase (1/2)
The Expiratory phase is as long
as and as loud as inspiratory
phase
2-There is no gap between
inspiratory & expiratory phase
There is a definite gap between
inspiratory & expiratory Phase
3- The character of the sound is
Rustling and low pitched
The character of sound is harsh
& aspirate & high pitched.
4-At the site of auscultation the
Vocal resonance is normal
At the site of auscultation the
vocal resonance is increased.
116.
Chest Exam- Auscultation
Vesicularbreath sound:- Is normal breath sound
heard over normal lungs
Bronchial Breath sound:- Normally heard over
trachea, may be heard in midline of chest.
-On chest wall
bronchial breath sound is heard when the lung
tissue between the airway and chest wall
becomes firm or solid. The sounds are
transmitted more readily and the filtering
effect of lung parenchyma is lost.
118.
Chest Exam- Auscultation
CommonCauses of Bronchial Breath Sound :-
- Consolidation
-Large, Empty cavity
- Open type of pneumo
thorax (Broncho Pleural
Fistula)
-Collapse of lungs with patent bronchus
(Compression Collapse)
-Localized fibrosis when bronchus is pulled
near chest wall
- Above the level of pleural effusion
119.
Chest Exam-Auscultation
B- AddedSounds:-
a) Ronchi (Wheeze):- It is continuous, musical sound
produced due to passage of air through narrowed
airways, usually more pronounced during
expiration
Polyphonic Ronchi:- It is common type of
wheeze, heard widespread over the chest particularly
during expiration
- It is
characteristic of
diffuse airway obstruction like-
- Bronchial Asthma
-COPD
- Chronic Bronchitis
-Pulmonary Edema
120.
Chest Exam- Auscultation
MonophonicRonchi:- Localized
ronchi due to localized narrowing of single
bronchus. It may be inspiratoty or expiratory
or both & may change in intensity in different
position.
Causes:-
- Tumor
-Foreign body
121.
Chest Examination-Auscultation
b) Crepitation(Crackles,Rales):- Intermittent, crackling
or bubbling sound produced due to passage of air
through fluid filled airways or opening up of previously
closed alveoli. Commonly heard during inspiration
Found in may pulmonary and cardiac diseases:-
- Bronchitis.(Acute, Chronic)
-Tuberculosis
-Bronchiactasis
-Interstitial lung disease
-Fibrosis
-Consolidation (Early & Resolution)
- Heart failure
-Pulmonary edema
122.
Chest Examination-Auscultation
Fine crepitationare late inspiratory and coarse are
usually early inspiratory.
Fine crepitation suggest an interstitial process and
are found in pulmonary fibrosis, interstitial lung
disease, heart failure etc.
Post tussive crepitation:- Crepts which persists
after coughing. It indicate Infiltration like early
Tuberculosis, Heart failure, Interstitial lung
disease etc.
Velcro Crepts:- Crepitation heard in cases of
interstitial pulmonary fibrosis
.
123.
Chest Exam-Auscultation
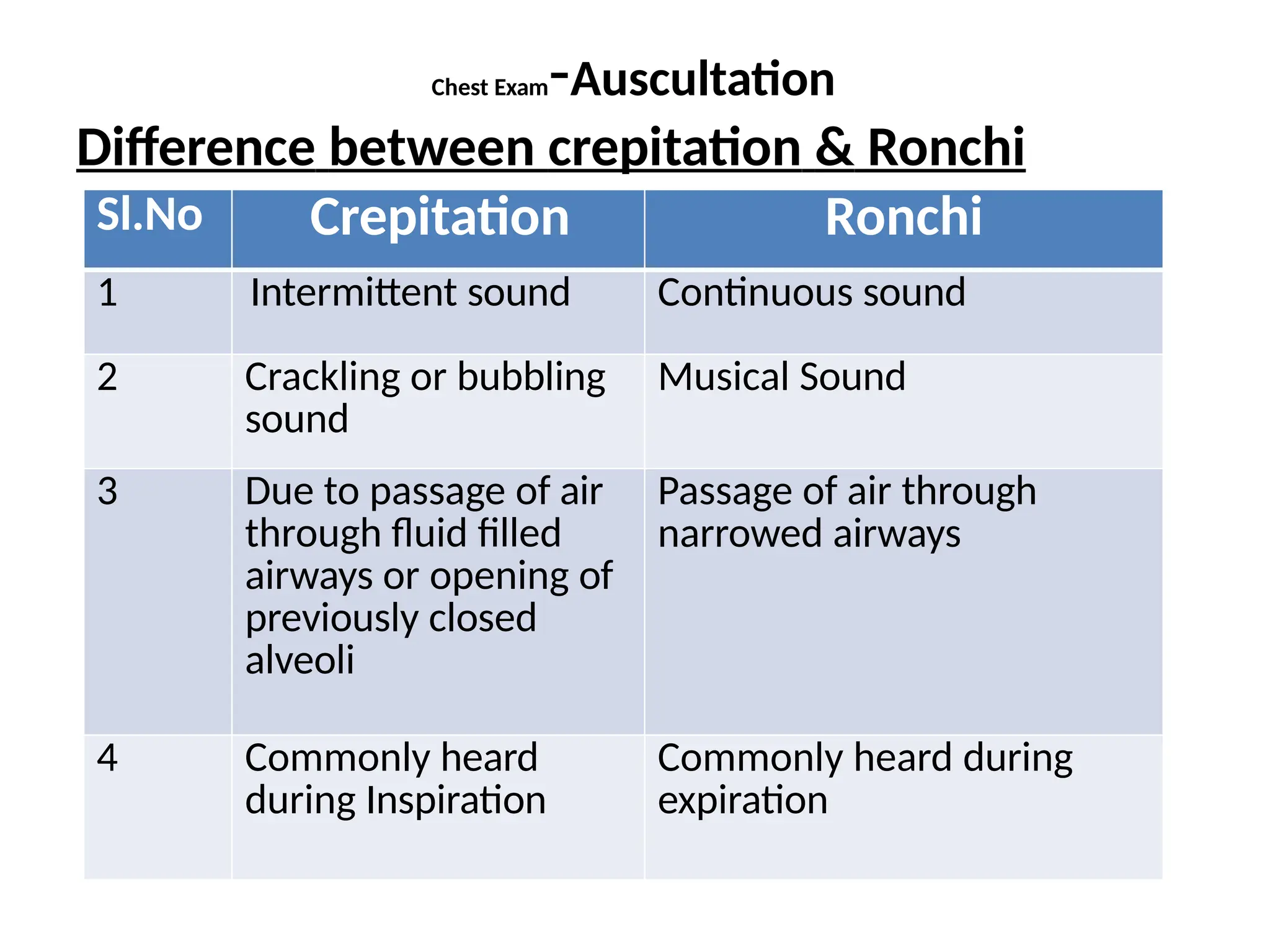
Difference betweencrepitation & Ronchi
Sl.No Crepitation Ronchi
1 Intermittent sound Continuous sound
2 Crackling or bubbling
sound
Musical Sound
3 Due to passage of air
through fluid filled
airways or opening of
previously closed
alveoli
Passage of air through
narrowed airways
4 Commonly heard
during Inspiration
Commonly heard during
expiration
124.
Chest Exam-Auscultation
c)- Pleuralfriction rub:- A superficial Leathery or
creaking/ rubbing ,usually localized sound
produced by movement of two layers of inflamed
pleura. It is best heard towards the end of
inspiration and just after the beginning of
expiration.- Heard in cases of pleurisy in cases of:-
-Tuberculosis
- Lodar Pneumonia
-Pulmonary infarction
-Malignant infiltration
125.
Chest Exam-Auscultation
Diff. betweencrepts and pleural friction
Rub:-
Sl. No. Crepitation Pleural Friction Rub
1 No pain at the site Pain at the site
2 Best heard during inspiration Best heard during end inspiration
and just after beginning of
expiration
3 Changes on coughing Do not change on coughing
4 Do not change on change of
posture
Change on change of posture
5 Deep sound Superficial sound
6 No change on increase the
pressure of stethoscope
Changes on increasing the
pressure of the stethoscope
126.
Chest Exam- Auscultation
PleuralRub, Pleuro-pericardial rub &Pericardial
Rub
Pleural Rub- Not audible on holding breath
Pleuro-Pericardial Rub:- Character & intensity
changes on holding breath
Pericardial friction rub:- No change on holding
breath
127.
Chest Examination- Auscultation
d)HippocraticSuccussion Splash:- In case of
hydropneumothorax put the Stethoscope at
the junction of Hyper resonance & stony
dullness & shake the patient vigorously. A
splashing sound is heard due to splashing of
fluid within the pleural space
Other condition where splashing sound is
heard:-- Gastric outlet obstruction
128.
Chest examination- Auscultation
e)Posttussive suction:- It is heard in case of
empty cavity having elastic wall and
communicating with bronchus . Stethoscope is
put on chest above the cavity and patient is
asked to cough vigorously. After coughing
when the patient inspires a hissing sound is
heard due to suction of air in to the cavity.
Not a common finding, but if present, is
diagnostic of cavity.
129.
Auscultation
C) Vocal Resonance:-It is resonance of
sound on the chest made by the voice.
-Same thing is palpated as Vocal fremitus and
auscultated as vocal resonance.
-The patient is asked to say one-one-one or
ninety nine- ninety nine and vibration on the
chest wall is heard through the stethoscope.
- On normal lungs the sound is muffled and
indistinct.
130.
Chest Examination- Auscultation
-Ifvocal resonance decreases the
intensity decrease or may not be
audible at all
-If vocal resonance is increased the sound is heard
more clearly.(Bronchophony)
-Whispering pectoriloquy:- The patient is asked to
whisper one-one-one or ninety nine-ninety nine
repeatedly. The sound is heard very clearly as
some one is whispering in your ear.
-Aegophony:- The sound gets a nasal tone. This is an
unusual physical finding.
131.
Auscultation
Causes of DecreasedVocal Resonance:-
(Same as causes of decreased Vocal fremitus )
- Emphysema
-Thickened Pleura
-Pleural Effusion
-Pneumothorax (Except open)
-Collapse (bronchus not patent)
132.
Chest Examination-Auscultation
Causes ofincreased vocal Resonance:-
(same as causes of increased Vocal fremitus)
-Consolidation
-Large Empty Cavity with patent
bronchus
-Open type of Pneumothorax
( Broncho pleural fistula)
- Collapse with patent
bronchus
- Fibrosis pulling the major
bronchus near the chest wall
- Above the level of Pleural
effusion
Write 3 causes/points for each
1 Sudden Dyspnoea
2 Dyspnoea with chest pain
3 Central (Retrosternal) Chest Pain
4 Causes of Hemoptysis
5 Accessory muscles of Respiration
138.
-
6 causes ofShift of Trachea
7 Causes of Increased Vocal fremitus/ Resonance
8 Adventitious sounds in Resp. Auscultation
9Localized decrease in intensity of Breath
Sound 10-Condition where Bronchial Breath
Sound found
139.
Choose 1 mostappropriate answer
1 Which is not a feature of Respiratory Illness?
a) Breathlessness
b) Palpitation
c)Chest Pain
d)Loud P2
2)Foul smelling sputum is a feature of?
a)Chronic Bronchitis
b)Emphysema
c)Bronchial Asthma
d) Bronchiectasis
140.
-
3)In resp. illness“Good days and Bad days” is
associated with?
a)Bronchial Asthma
b) Pneumoconiosis
c) Chronic
Bronchitis
d)Emphysema
4) Evening fever with
sweating is a
feature of?
a)Tuberculosis
b) Pneumonia
c) Bronchiectasis
141.
-
5) What isnormal Breathing : Pulse ratio at Rest?
a) 1 : 2
b) 1 : 3
c) 1 : 4
d) 1 : 5
6) Cyclic increase and decrease in respiratory
effort and rate with a period of Apnea is called?
a)Hyperpnoea
b) Cheyne stoke Breathing
c)Kussmaul Breathing
d)Paradoxical Respiration
142.
-
7) Drooping ofShoulder is commonly found in?
a)Chronic Bronchitis
b)Emphysema
c)Interstitial Lung Disease
d) Tuberculosis
8) Normal Liver Dullness
starts in?MCL Mid Axill.Line Mid Scap.Line
a) 3rd
5th 7th
b)
4th 6th 8th
c)
5th 7th 9th
d)
6th 8th 10th
143.
-
9) Which donot cause intercostal fullness?
a) Bronchial Asthma
b)Emphysema
c) Pleural Effusion
d) Pneumothorax
10) Normal Trachea is
?
e) Exactly central
f) Slightly deviated
to Right
g) Slightly deviated
to Left
144.
-
11) Which isnot a feature of Cor pulmonale ?
a)Left Parasternal heave
b) Epigatric Pulsation
c) Loud P2
d) Wide & Fixed Splitting of 2nd Heart Sound
12) Breath Sound is Produced in ?
a)
Larynx
b)Trachea
c)Main
Bronch
us
145.
-
13) Which isnot a cause of decreased
Vocal fremitus ?
a) Emphysema
b) Collapse with patent Bronchus
c) Thickened Pleura
d) Pleural effusion
14) Obliteration of hepatic & cardiac
dullness is
feature of ?
a)Chronic Bronchitis
b)Emphysema
c)Pneumoconiosis
d) Asbestosis
146.
-
15) Hyper resonanceon percussion not found in?
a)Consolidation
b) Large Empty Cavity
c) Pneumothorax
d) Emphysema
16) Stony Dullness on percussion is found in ?
a) Consolidation
b)Cavit
y
c)Collapse
d)
Hydrothor
147.
-
17) We askthe Patient to put both hands on
head for?
a) Direct Percussion
b) Anterior Chest Percussion
c) Axillary chest Percussion
d)Inter scapular Percussion
18) Not true for Bronchial Breath sound?
a)Prolonged Expiration
b) Gap between inspiration & expiration
c) Low pitched Rustling Character
d) Increased Vocal Resonance at the site
148.
-
19) Which isnot true for
Ronchi ?
a) Intermittent sound
b) Musical Sound
c)Due to narrowed airways
d) Common during Expiration
20) Ronchi is not heard in ?
a) Bronchial Asthma
b)Chronic Bronchitis
c) COPD
d) massive Pleural effusion
149.
-
21) Post Tussivesuction is a feature of ?
a) Consolidation
b) Collapse
c) Cavity
d) Fibrosis
22) Suction Splash is found in?
a) Pneumothorax
b)Left ventricular out flow obstruction
c) Gastric Outlet obstruction
d) Pericardial effusion
150.
-
23) Pleural frictionrub may be heard in?
a) Massive Pleural Effusion
b) Large Pneumothorax
c)Large Cavity
d) Lobar Pneumonia
24) Mark Odd Statement
a) Decreased Vocal fremitus
b)Dull on percussion
c)Bronchial Breath Sound
e) Increased Vocal
Resonance
151.
-
25) Mark oddstatement
a) Bronchophony
b)Whispering pectoriloquy
c) Nasophony
d) Aegophony
-
7-Causes of IncreasedVocal fremitus/ Resonance
*Consolidation
*Large Empty Cavity
*Open Type of Pneumothorax
*Collapse with Patent Bronchus
*Fibrosis pulling major bronchus near chest
wall
-
9- Localized decreasein intensity of Breath
Sound
*Marked Pleural Thickening
*Pleural effusion
*Pneumothorax (Except Open Type)
*Absorption collapse (Obstruction in
airway)
162.
-
10-Conditions Where BronchialBreath Sound
found
*Consolidation (Tubular Bronchial)
* Large Cavity ( Cavernous Bronchial)
*Open Pnemothorax/ Broncho Pleural
Fistula (Amphoric Bronchial)
*Collapse with Patent Bronchus
*Localized fibrosis pulling major Bronchus
near chest wall
*Some times above the level of Pleural
Effusion
163.
-
1 Which isnot a feature of Respiratory Illness?
a) Breathlessness
b) Palpitation
c)Chest Pain
d)Loud P2
2)Foul smelling sputum is a feature of?
a)Chronic Bronchitis
b)Emphysema
c)Bronchial Asthma
d) Bronchiectasis
164.
-
3)In resp. illness“Good days and Bad days” is
associated with?
a)Bronchial Asthma
b) Pneumoconiosis
c)Chronic Bronchitis
d)Emphysema
4) Evening fever with
sweating is a
feature of?
a)Tuberculosis
b) Pneumonia
c) Bronchiectasis
d) Chronic
165.
-
5) What isnormal Breathing : Pulse ratio at Rest?
a) 1 : 2
b) 1 : 3
c) 1 : 4
d) 1 : 5
6) Cyclic increase and decrease in respiratory
effort and rate with a period of Apnea is called?
a)Hyperpnoea
b) Cheyne stoke Breathing
c)Kussmaul Breathing
d)Paradoxical Respiration
166.
-
7) Drooping ofShoulder is commonly found in?
a)Chronic Bronchitis
b)Emphysema
c)Interstitial Lung Disease
d) Tuberculosis
8) Normal Liver Dullness
starts in?
a)
MCL Mid Axill.Line Mid Scap.Line
3rd 5th 7th
b)
4th 6th 8th
c)
5th 7th 9th
d)
6th 8th 10th
167.
-
9) Which donot cause intercostal fullness?
a) Bronchial Asthma
b)Emphysema
c) Pleural Effusion
d) Pneumothorax
10) Normal Trachea is
?
e) Exactly central
f) Slightly deviated
to Right
g) Slightly deviated
to Left
168.
-
11) Which isnot a feature of Cor pulmonale ?
a)Left Parasternal heave
b) Epigatric Pulsation
c) Loud P2
d) Wide & Fixed Splitting of 2nd Heart Sound
12) Breath Sound is Produced in ?
a)Larynx
b)Trachea
c)Main
Bronch
us
d) Bronch
169.
-
13) Which isnot a cause of decreased
Vocal fremitus ?
a) Emphysema
b) Collapse with patent Bronchus
c) Thickened Pleura
d) Pleural effusion
14) Obliteration of hepatic & cardiac dullness
is feature of ?
a)Chronic Bronchitis
b)Emphysema
c)Pneumoconiosis
d) Asbestosis
170.
-
15) Hyper resonanceon percussion not found in?
a)Consolidation
b) Large Empty Cavity
c) Pneumothorax
d) Emphysema
16) Stony Dullness on percussion is found in ?
a) Consolidation
b)Cavit
y
c)Collapse
d)
Hydrothor
171.
-
17) We askthe Patient to put both hands on head
for?
a) Direct Percussion
b) Anterior Chest Percussion
c) Axillary chest Percussion
d)Inter scapular Percussion
18) Not true for Bronchial Breath sound?
a)Prolonged Expiration
b) Gap between inspiration & expiration
c) Low pitched Rustling Character
d) Increased Vocal Resonance at the site
172.
-
19) Which isnot true for
Ronchi ?
a) Intermittent sound
b) Musical Sound
c)Due to narrowed airways
d) Common during Expiration
20) Ronchi is not heard in ?
a) Bronchial Asthma
b)Chronic Bronchitis
c) COPD
d) massive Pleural effusion
173.
-
21) Post Tussivesuction is a feature of ?
a) Consolidation
b) Collapse
c) Cavity
d) Fibrosis
22) Suction Splash is found in?
a) Pneumothorax
b)Left ventricular out flow obstruction
c) Gastric Outlet obstruction
d) Pericardial effusion
174.
-
23) Pleural frictionrub may be heard in?
a) Massive Pleural Effusion
b) Large Pneumothorax
c)Large Cavity
d) Lobar Pneumonia
24) Mark Odd Statement
a) Decreased Vocal fremitus
b)Dull on percussion
c)Bronchial Breath Sound
e) Increased Vocal
Resonance
175.
-
25) Mark oddstatement
a) Bronchophony
b)Whispering pectoriloquy
c) Nasophony
d) Aegophony