Physical examinations
GA: A Thai boy , good consciousness
V/S – BP 112/74 mmHg, PR 110 bpm, T 37.2 oC,
RR 20/min
BW.25 kg. (P.25) , Height 128 cm. (P.10-25)
HEENT – No pale conjunctiva, anicteric sclera,
thyroid gland not enlargement, no frontal bossing
LN – Not palpable at supraclavicular, axillary and
both groins
Heart – Regular rhythm, normal S1S2, no murmur
Lungs – Clear both lungs
Abdomen – Soft , not tender, no palpable mass
8.
Extremities
Right leg: Mass 10x15 cm.above Rt. Knee
,hard concistency, ,round shape, fixed,irregular
border, not tender, no fluctuation
Rt.knee not tender, not swelling , full
ROM,sensory intact
Rt.hip not tender
9.
Skin –No rash, no petechiae, not seen
abnormal hypo/hyperpigmentation, normal
skin turgor, cap. Refil Rt.leg <2 sec
Neuro – Alert, pupils 3 mm RTLBE, Full
EOM,no facial palsy, motor grade V all
extremities, sensory intact, reflex 2+ all
10.
Problem lists
AThai boy 9 years old
Rapid growing Rt.leg mass above Rt.knee with
night pain 2 wk.PTA
Investigations
1. Plain film=> AP,lateral
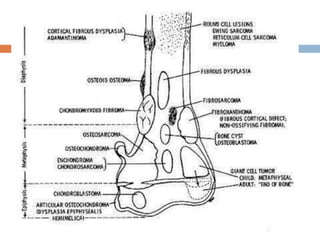
Enneking’s questions
Where is the lesion ?
What is the lesion doing to the bone ?
Geographic border (transitional zone ชัด)
Moth eaten border
Permeative border (transitional zone กว้าง)
28.
What isthe bone doing ?
Periosteal reaction
Solid
Codman’s triangle
Onion skin
Sunray appearance
30.
What isin the lesion ?
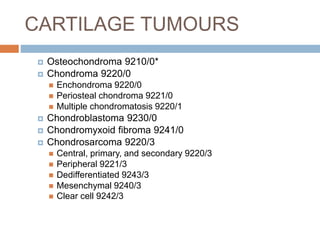
Bone forming tumor
Osteoid
Osteosarcoma
Chondroid
Chondrosarcoma