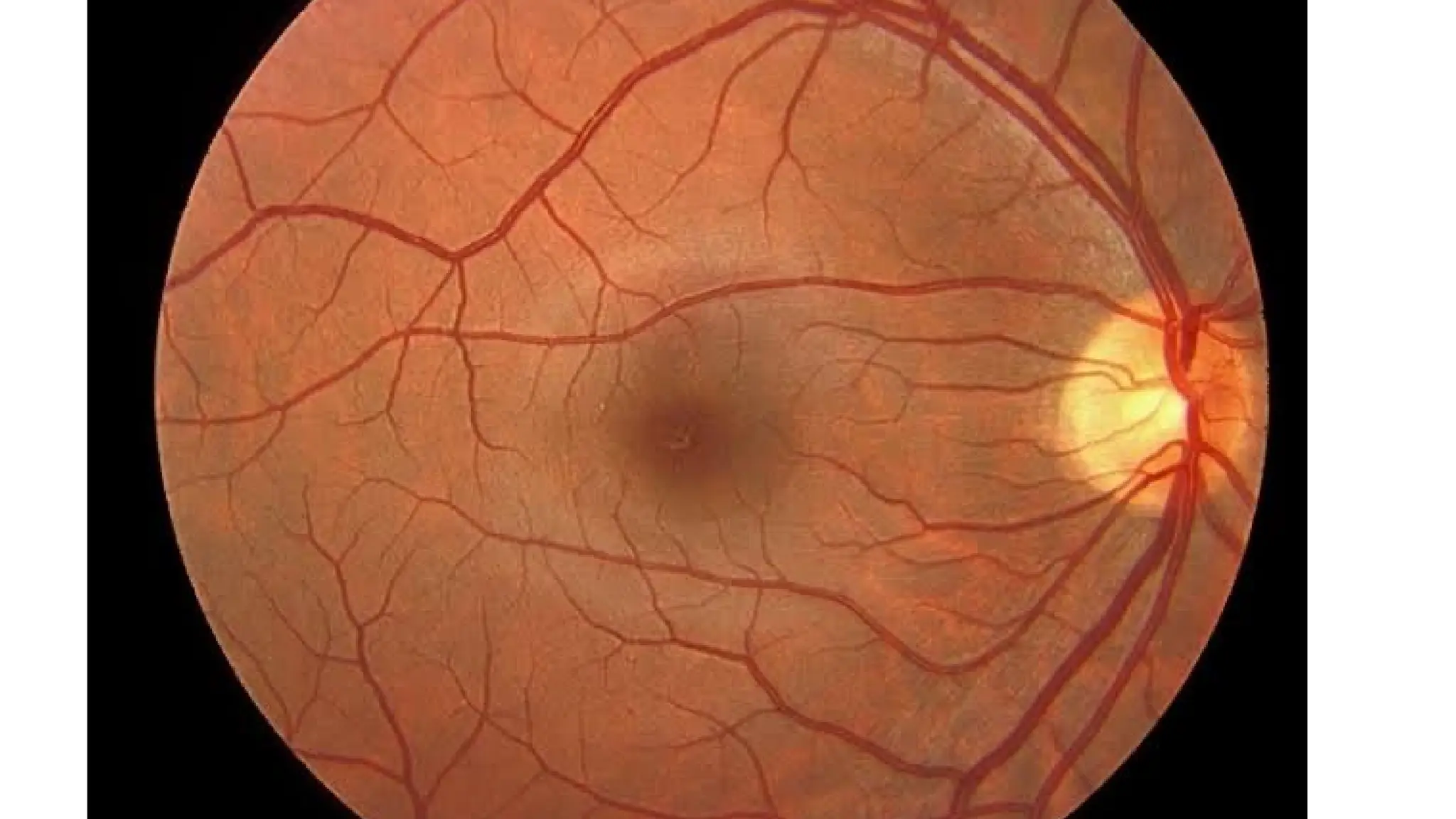
• It isa uniform red , punctate stippling periphery, varies color of
individual, normal choroidal vessels invisible
• Parts- disc, vessels, macula, periphery
• Ora serrate- junction between peripheral retina and pars plana
• Contents- dentate processes and oral bays
5.
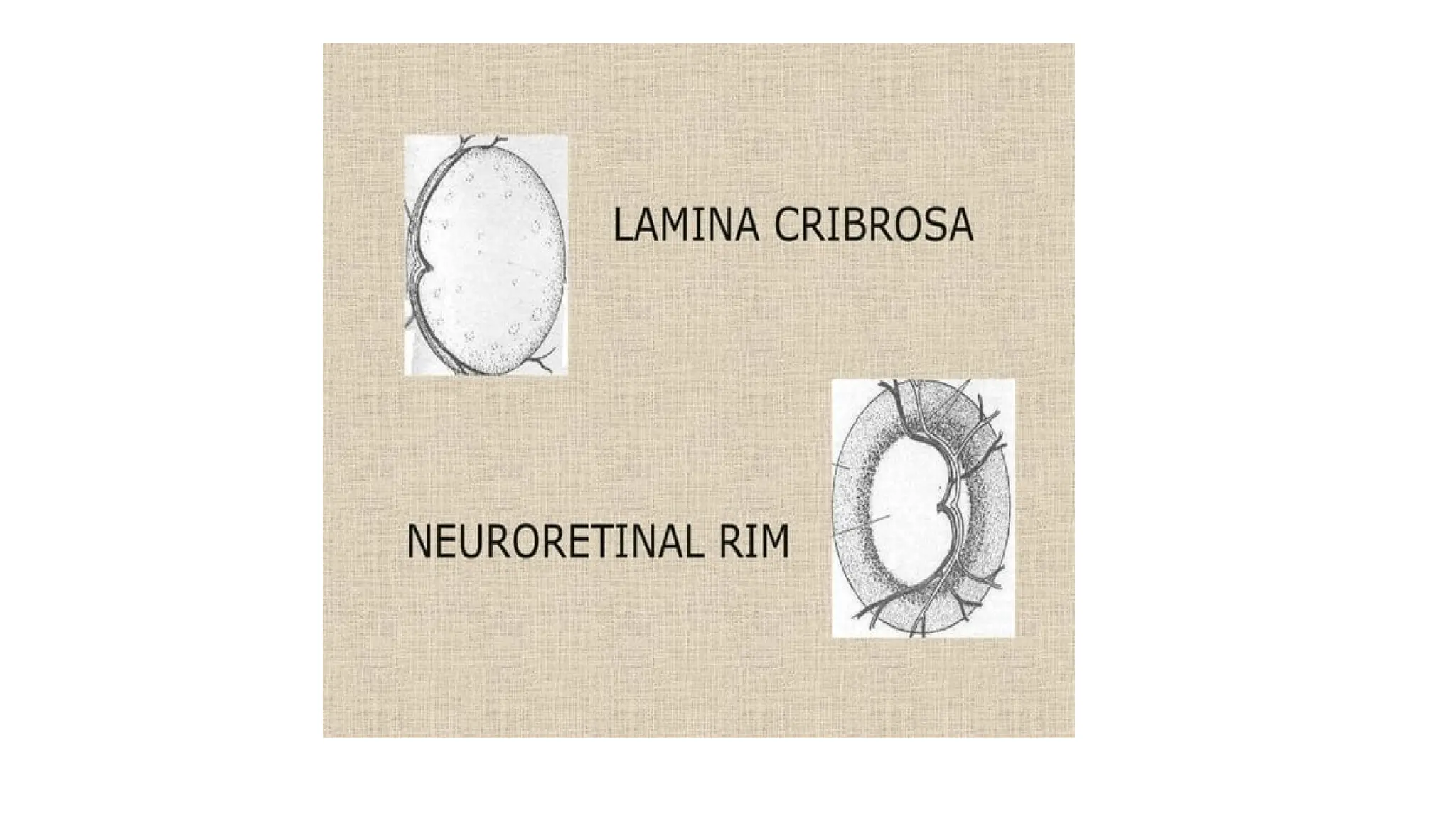
Optic disc
• Location-nasal to geometric axis
• Diameter- 1.5mm , color- pale pink, shape- circular, edges- regular
• Termination of all layers except NFL
• CDR – 0.3 to 0.5
6.
Vessels
• Retinal system:
•Central retinal artery and central retinal vein
• 4 major branches, arterioles, venules, capillaries
• Ciliary system: post ciliary arteries and choriocapillaries
Distant direct ophthamoscope
•Patient sitting in semi dark room – from distance of 20-25cm- features
of red glow in pupillary area is noted.
• Applications:
• To diagnose opacities in refractive media
• To differentiate between a mole and a hole in iris
• To recognize detached retina or a tumour arising from fundus
12.
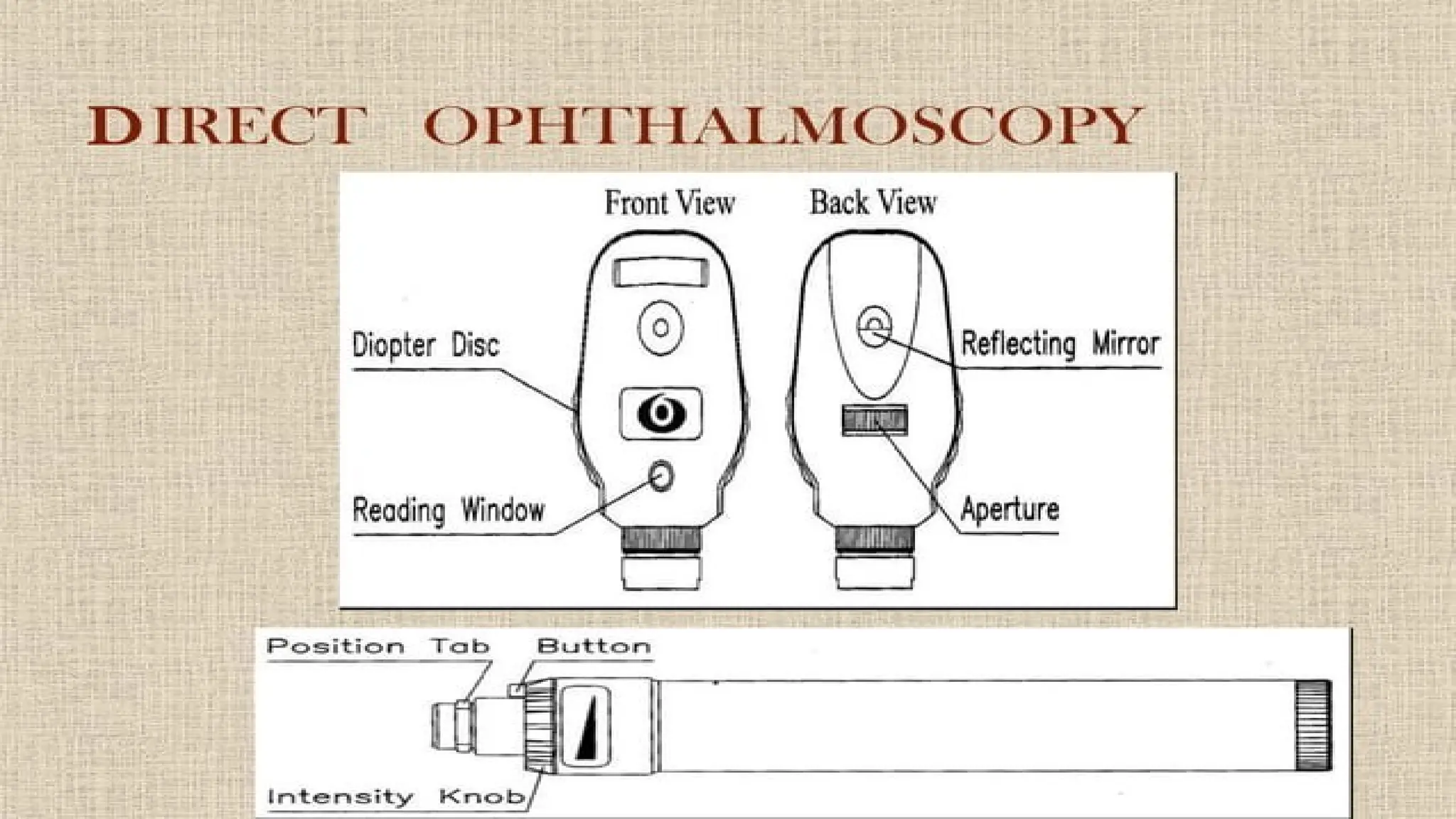
Direct ophthalmoscope
• Optics:
•A convergent beam of light reflected in patients pupil, emergent rays
from any point on patients fundus reaches observer retina through
hoe in ophthalmoscope.
• In hypermetropic retina, emergent rays will be divergent and it can be
brought to focus by convex lenses.
• In myopic retina , emergent rays will be convergent and it can be
brought to focus by concave lenses.
13.
• Characteristics ofimage formed :
• direct ophthalmoscopy, image is erect, virtual and 14-15 times magnified.
• Field of view:
• It is always smaller than the field of illumination.
• directly proportional to size of pupil , axial length of observed eye and
indirectly proportional to distance between observed and observer’s eye.
• Disadvantages:
• Unwanted reflections, peripheral viewing
14.
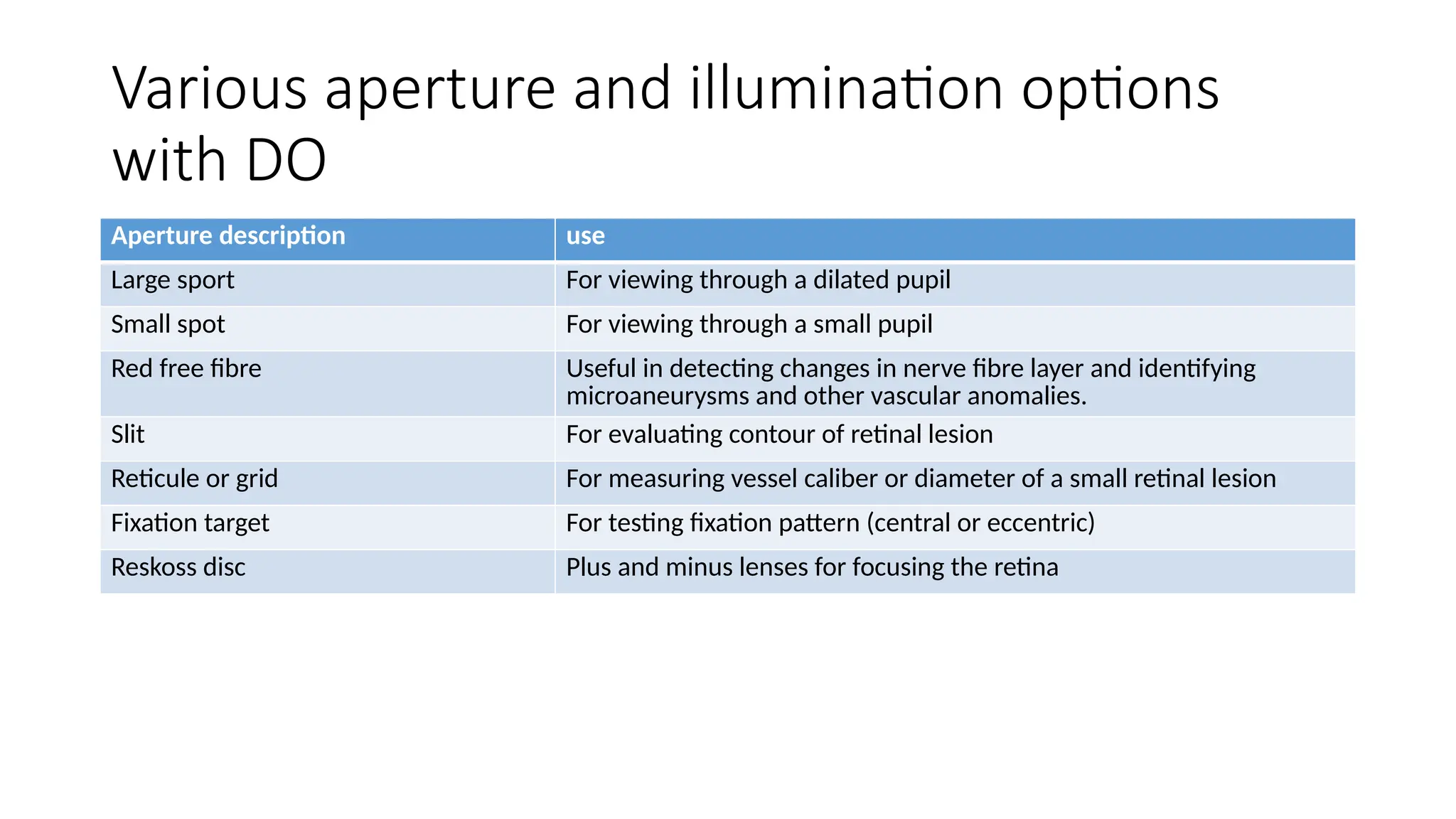
Various aperture andillumination options
with DO
Aperture description use
Large sport For viewing through a dilated pupil
Small spot For viewing through a small pupil
Red free fibre Useful in detecting changes in nerve fibre layer and identifying
microaneurysms and other vascular anomalies.
Slit For evaluating contour of retinal lesion
Reticule or grid For measuring vessel caliber or diameter of a small retinal lesion
Fixation target For testing fixation pattern (central or eccentric)
Reskoss disc Plus and minus lenses for focusing the retina
15.
Interpretation
• Start atoptic disc- look for CD ration, color, clarity of margins,
spontaneous venous pulasations and around the optic disc especially
superior and inferior temporal arcades.
• Vessels- AV ratio, color, diametr, course
• Macula- Foveal reflex, color, pigmentation.
• Any abnormalities described in disc area and distane from disc or
macula in terms of disc diameters.
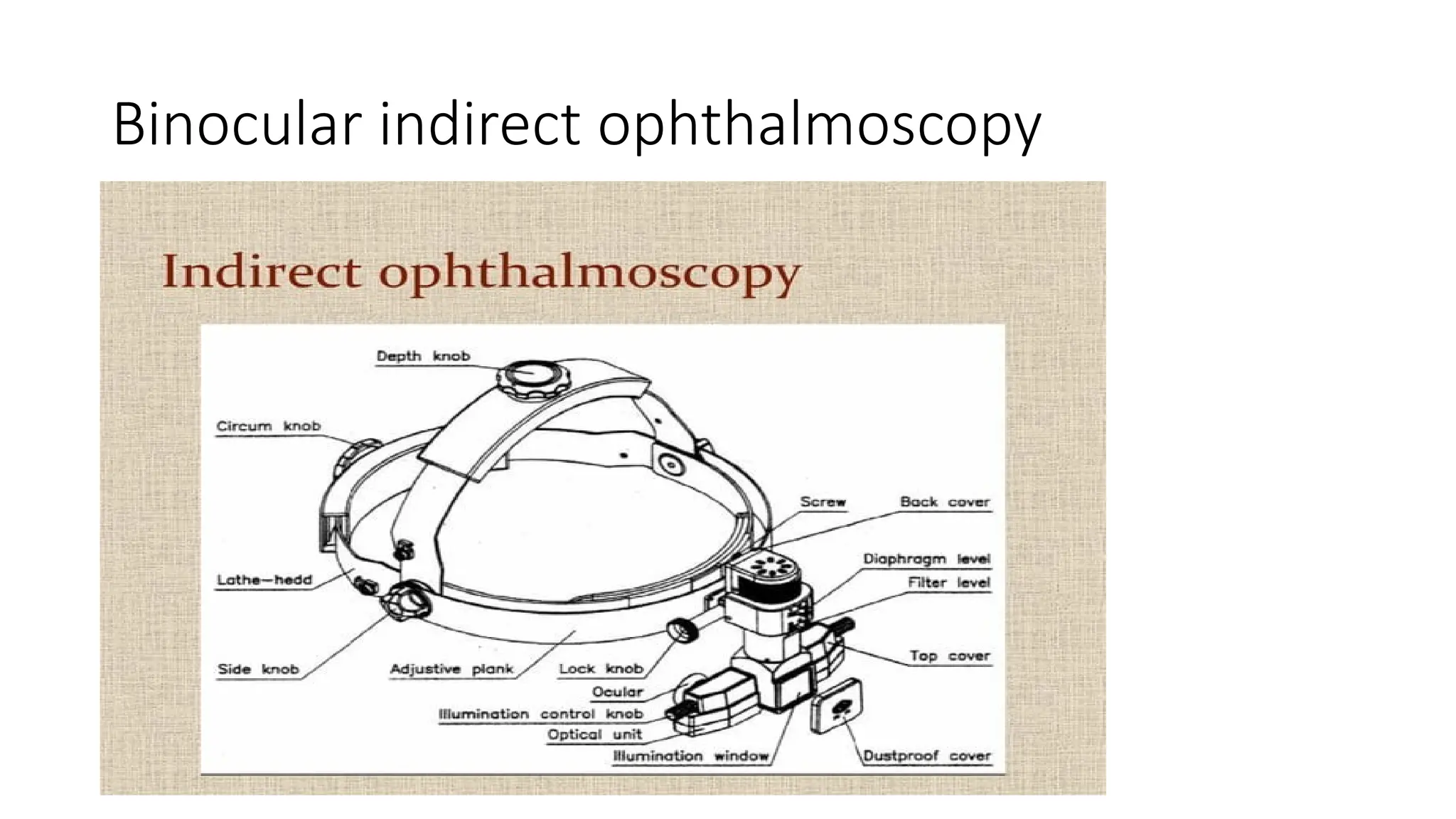
Structural features
• Illuminationrheostat at its base
• Focussing lever for image refinement
• Filter dial- red and yellow filter
• Forehead rest
• Iris diaphragm lever- to adjust illumination beam diaphragm
• Optics: an internal relay lens system re inverts the initially inverted
image to real erect one which is then magnified
18.
• Indications :
•Need for an increased field of view
• Small pupil
• Uncooperative children
• Patients intolerance of light in binocular IDO
• Basic fundus screening
• Extent of view:
• Anteriorly to peripheral equatorial region
• +40degree field of view is same as binocular IDO
19.
Advantages and disadvantages
•Advantages:
• Increased field of view as IDO
• Erect real image similar to DO
• Disadvantages:
• Lack of stereopsis
• Limited illumination
• Fixed magnification
• Fair to good resoution
Optics of Indirectophthalmoscope
• The principle of indirect ophthamoscope is to make the eye highly
myopic by placing a strong condensing lens in front to patients eye so
that emerging rays from an area of fundus are brought to focus as a
real inverted image.
• Optical system:
• Binocularity achieved by reducing interpupillary distance from 60mm
to 15mm by prism/ mirrors
• Field of illumination- more in myopes and less in hypermetropes
22.
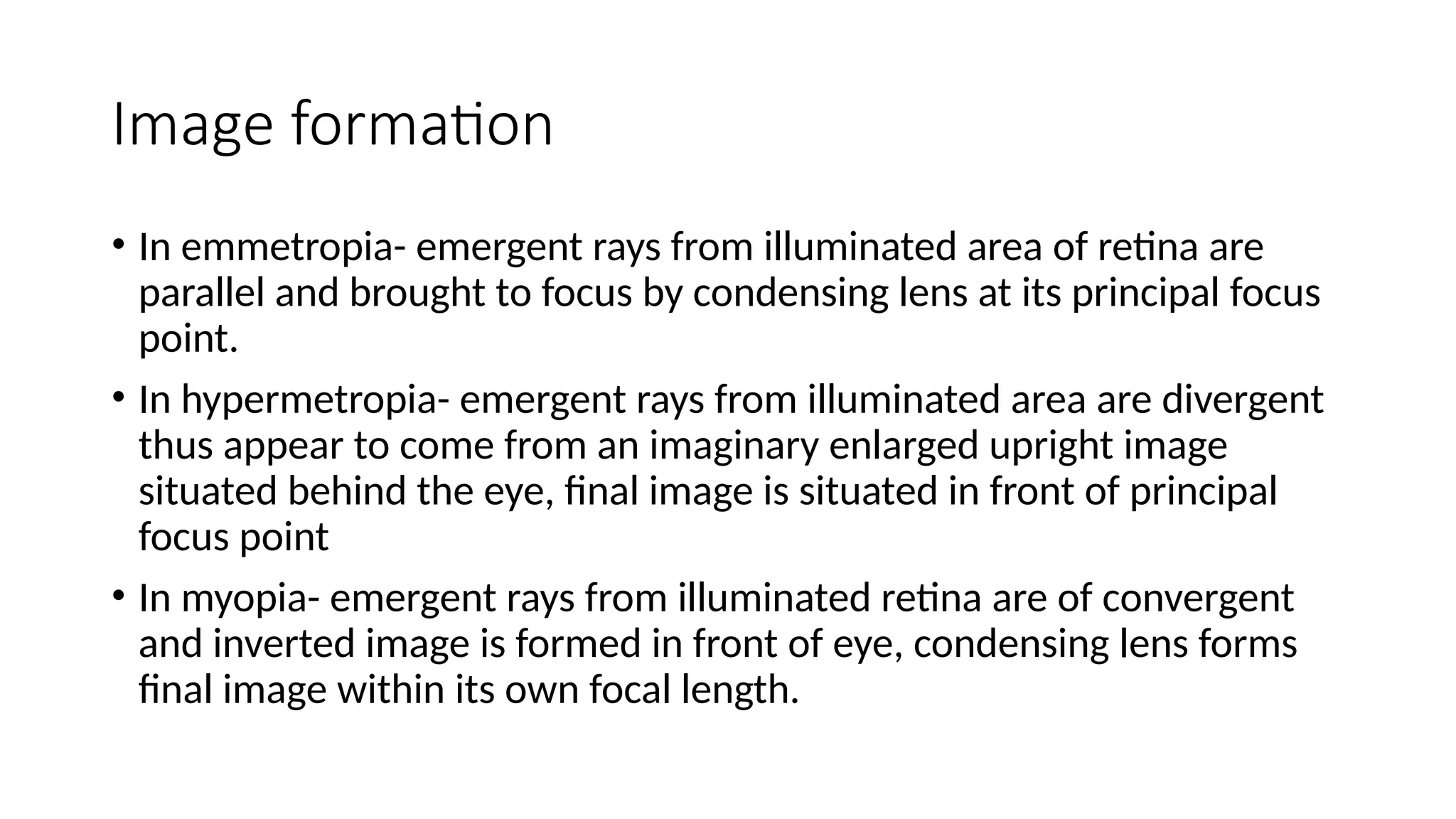
Image formation
• Inemmetropia- emergent rays from illuminated area of retina are
parallel and brought to focus by condensing lens at its principal focus
point.
• In hypermetropia- emergent rays from illuminated area are divergent
thus appear to come from an imaginary enlarged upright image
situated behind the eye, final image is situated in front of principal
focus point
• In myopia- emergent rays from illuminated retina are of convergent
and inverted image is formed in front of eye, condensing lens forms
final image within its own focal length.
24.
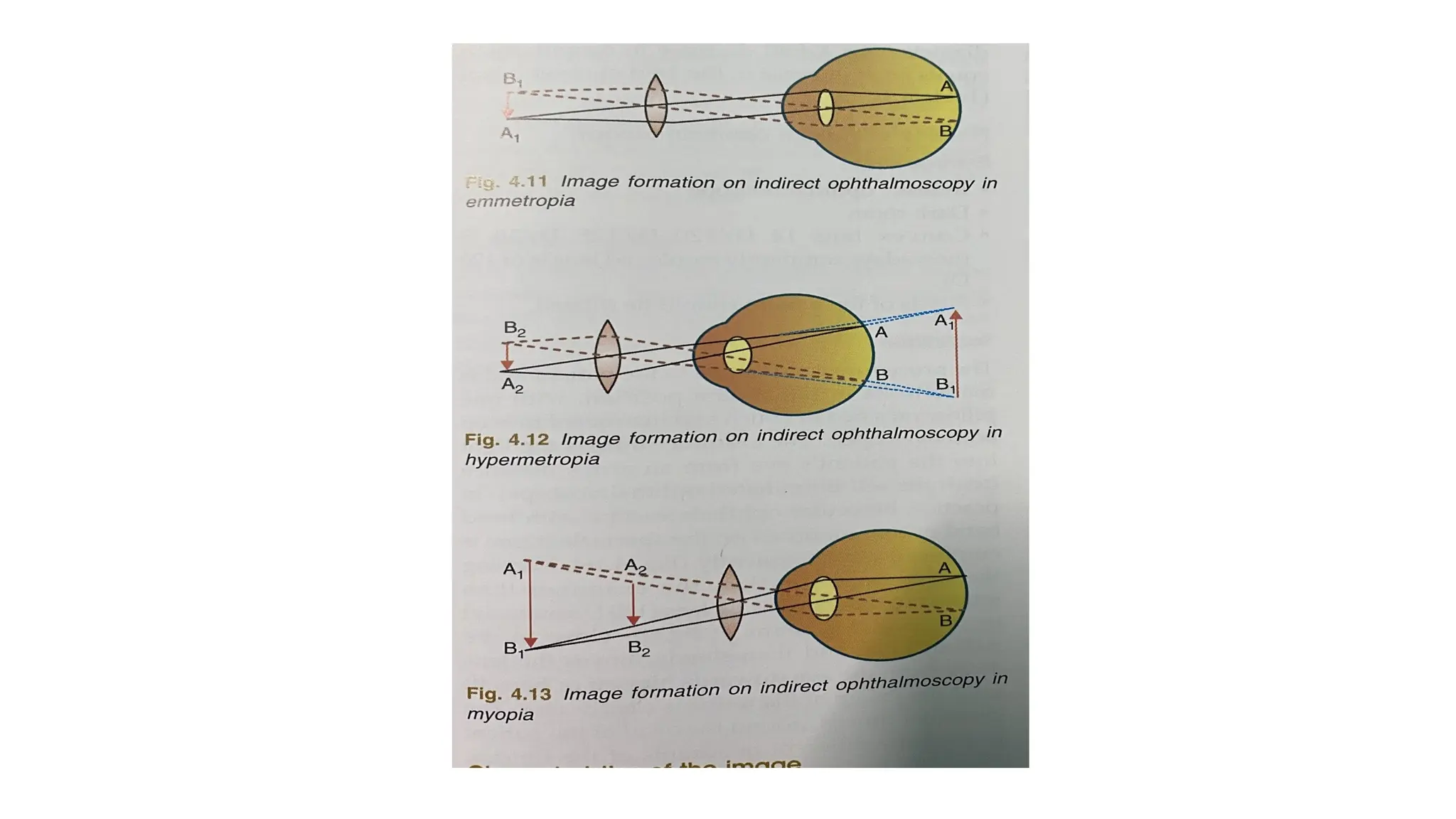
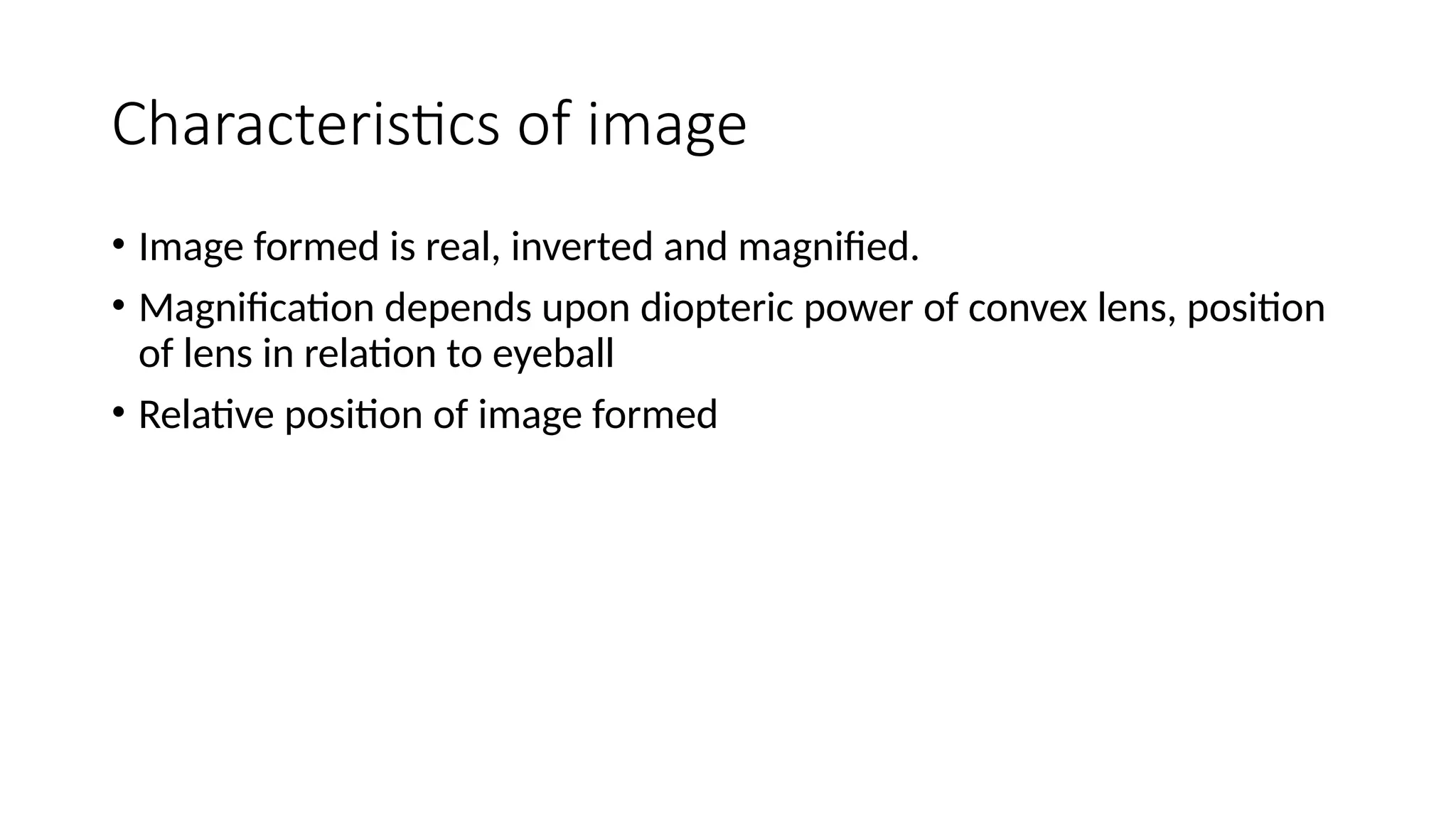
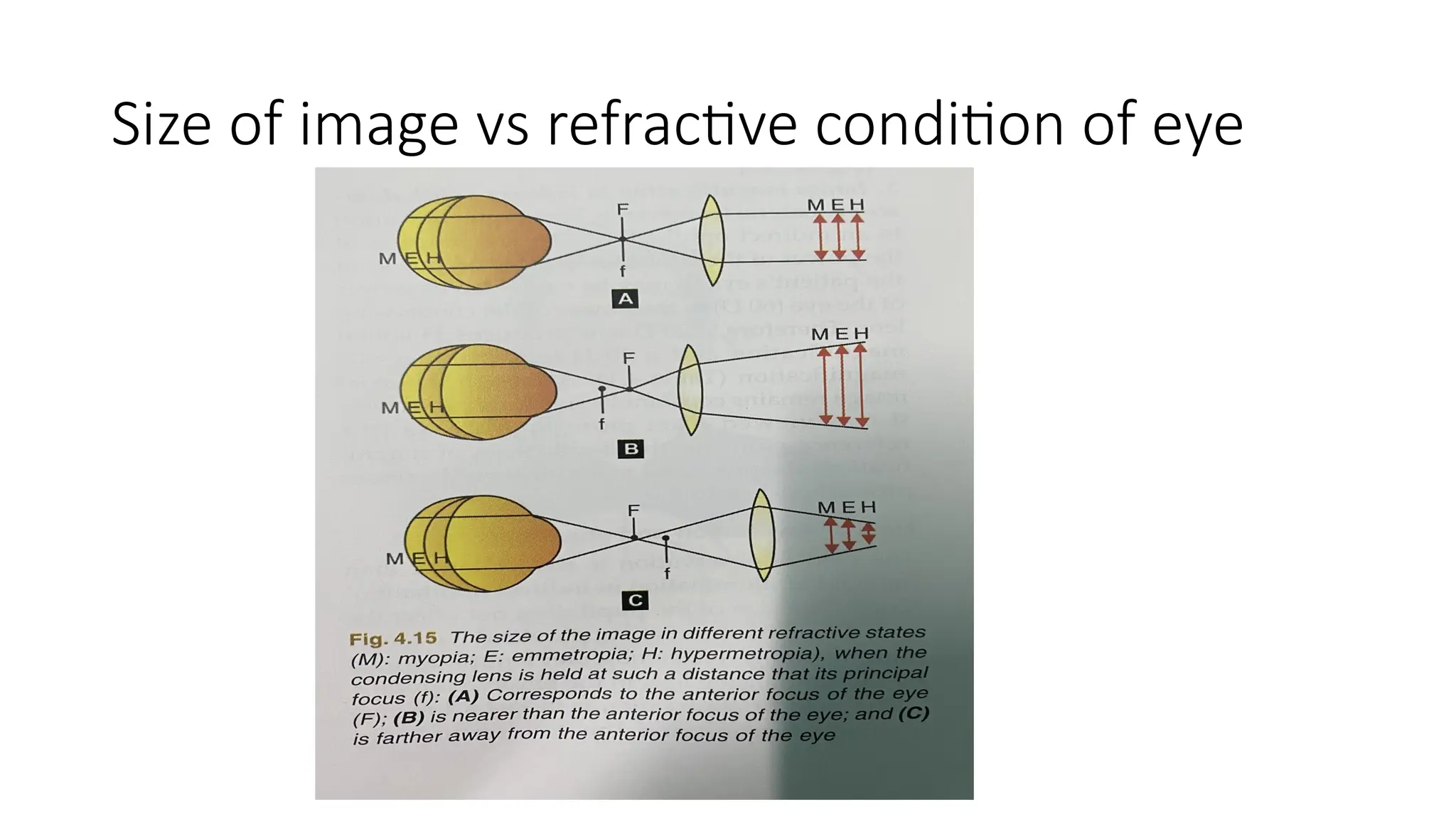
Characteristics of image
•Image formed is real, inverted and magnified.
• Magnification depends upon diopteric power of convex lens, position
of lens in relation to eyeball
• Relative position of image formed
Image magnification
• Lateralmagnification is a function of power of condensing lens and
patients eye.
• 20D produces 33 lateral magnification and 30D produces 23 lateral
magnification.
• Field of observation is larger than field of ilumination
27.
Practice of indirectophthalmoscopy
• Prerequisites:
• Indirect ophthalmoscope
• Dark room
• Convex lens 14D/120D/128D/30D
• Dilated pupil
• Technique:
• Patient in supine position, examiner throws light from an arm’s distance , keeping
the eys on the reflex, examiner then interposes condensing lens in the path of
beam close the patients eye. Examiner moves around the head of patient to
examine different quadrants, by using scleral indenter whole peripheral retina
upto ora serrata is visualized.
28.
Scleral indentation
• Usingdepressor placed on patients lids
• Scleral depressor moved in opposite direction to that of examining
quadrant.
• Depressor rolled gently and tangentially over the eye surface
• In superonasal quadrant- most sensitive to scleral depression.
• Sometimes topical anesthesia applied and depressor applied over the
medial conjunctiva
• When posterior areas of fundus are to be examined , ask the patient
to look slightly towards his or her position.
29.
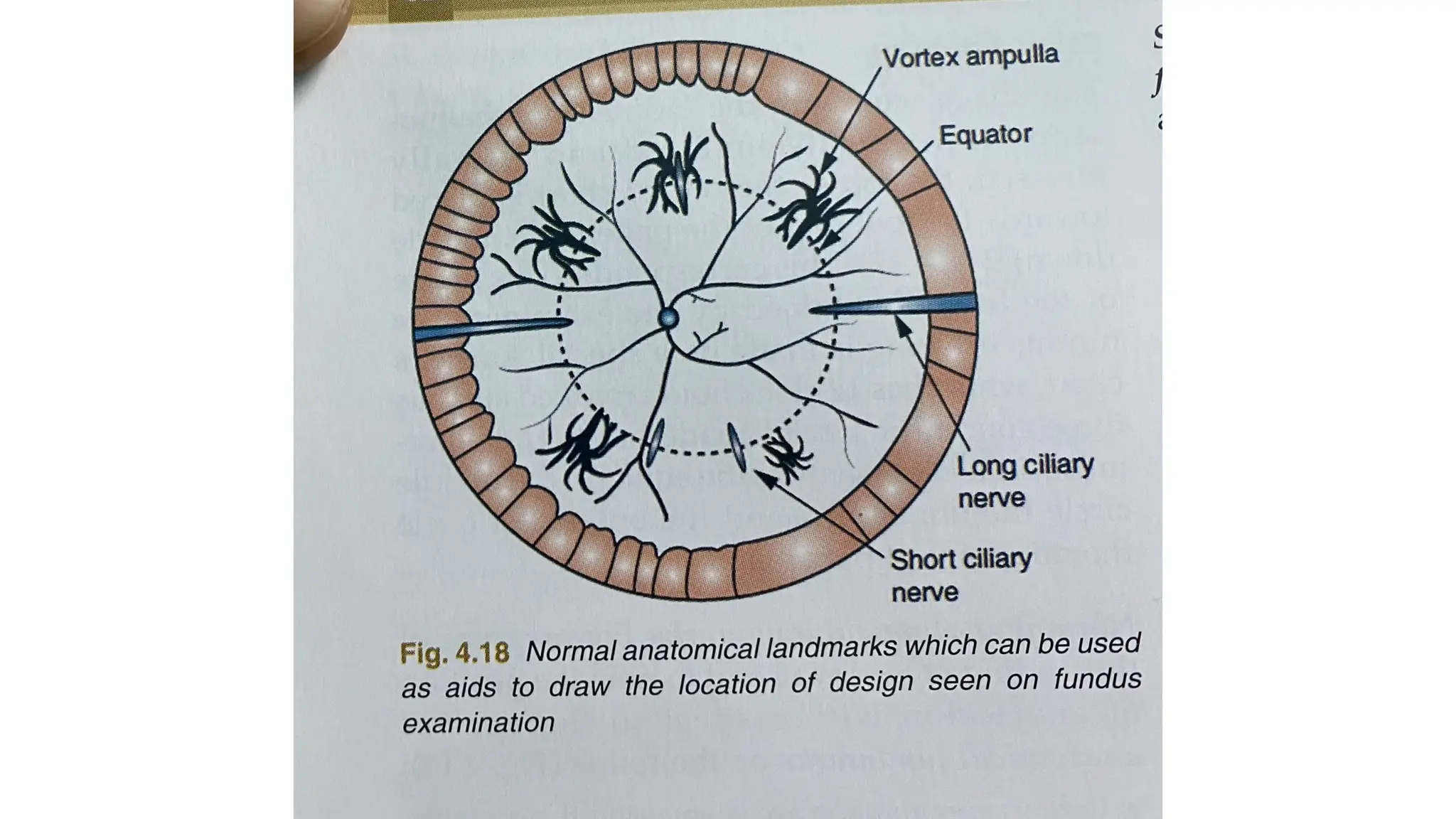
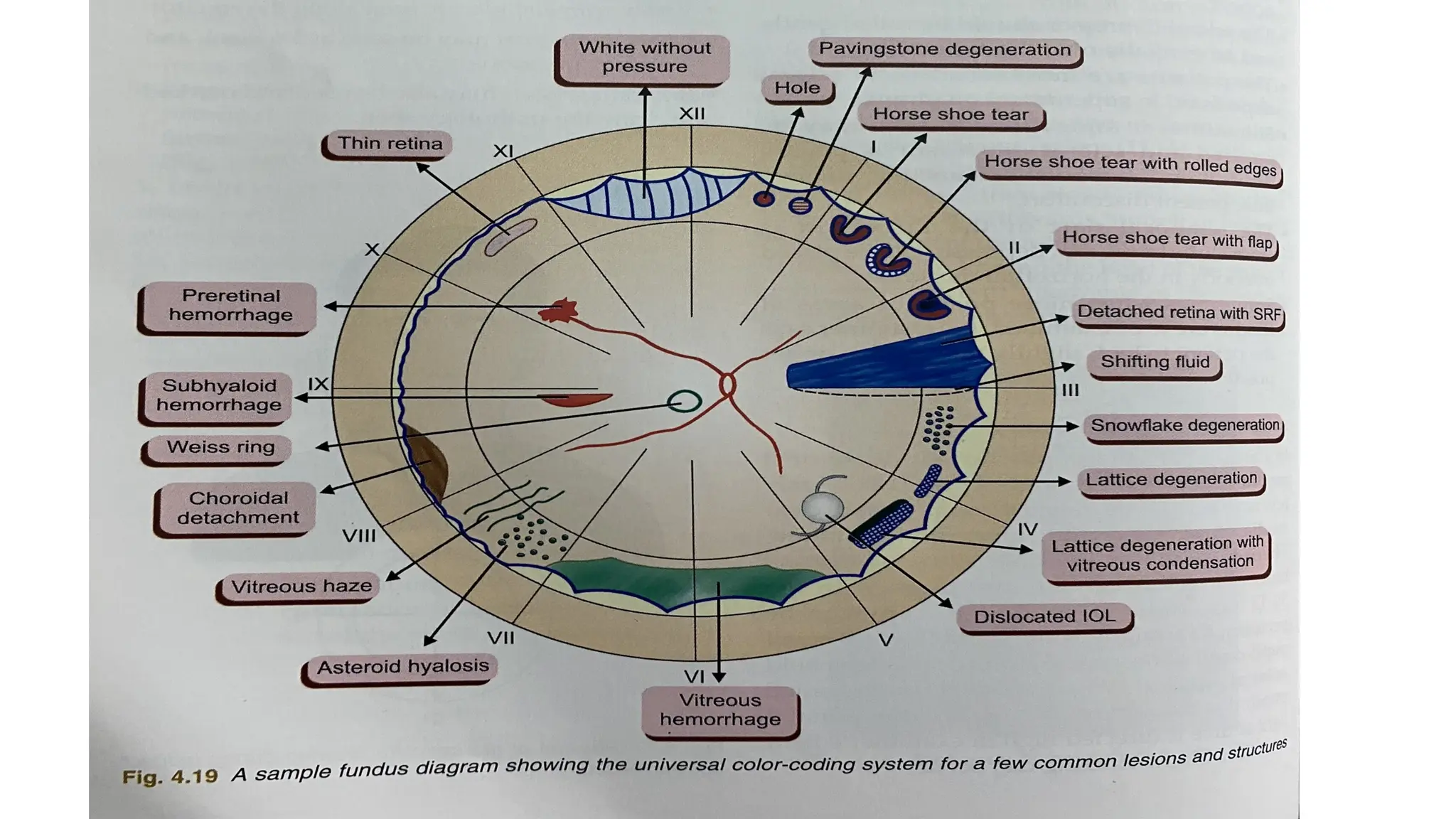
Fundus drawing
• Itis made on Amsler’s chart which has 12 clock hours marked and three
concentric circles on it .
• Innermost circle- equator
• Middle circle – ora serrate
• Outermost circle- midpoint of pars plana.
• Anatomical landmarks
• Vortex veins ampulla seen on equator
• Long ciliary veins- at 3and 9’o clock positions
• Branching vessels
32.
Advantages
• Larger fieldof retina is visible, 10 times increase in magnification
compared to DO.
• Lesser distortion of image
• Easy to examine , if patients eye movements are present and with
high spherical or astigmatic refractive errors.
• It gives 3D stereoscopic view of retina with considerable depth of
focus.
• Useful in hazy media because of its bright light and optical property.
33.
Disadvantages:
• Magnification is5 times compared to DO which is 15 times
• Impossible for very small pupils
• Patients are more uncomfortable with intense light and ith scleral
indentation.
• Procedure requires extensive practice
• Reflex sneezing occurs on exposure to bright light.
Hruby lens biomicroscopy
•It is a phacoconcave lens with 58.6D which neutralizes optical power
of normal eye160D, and forms virtual erect imageof fundus.
• It provides small field with low magnification and cannot visualize the
fundus beyond equtor.
36.
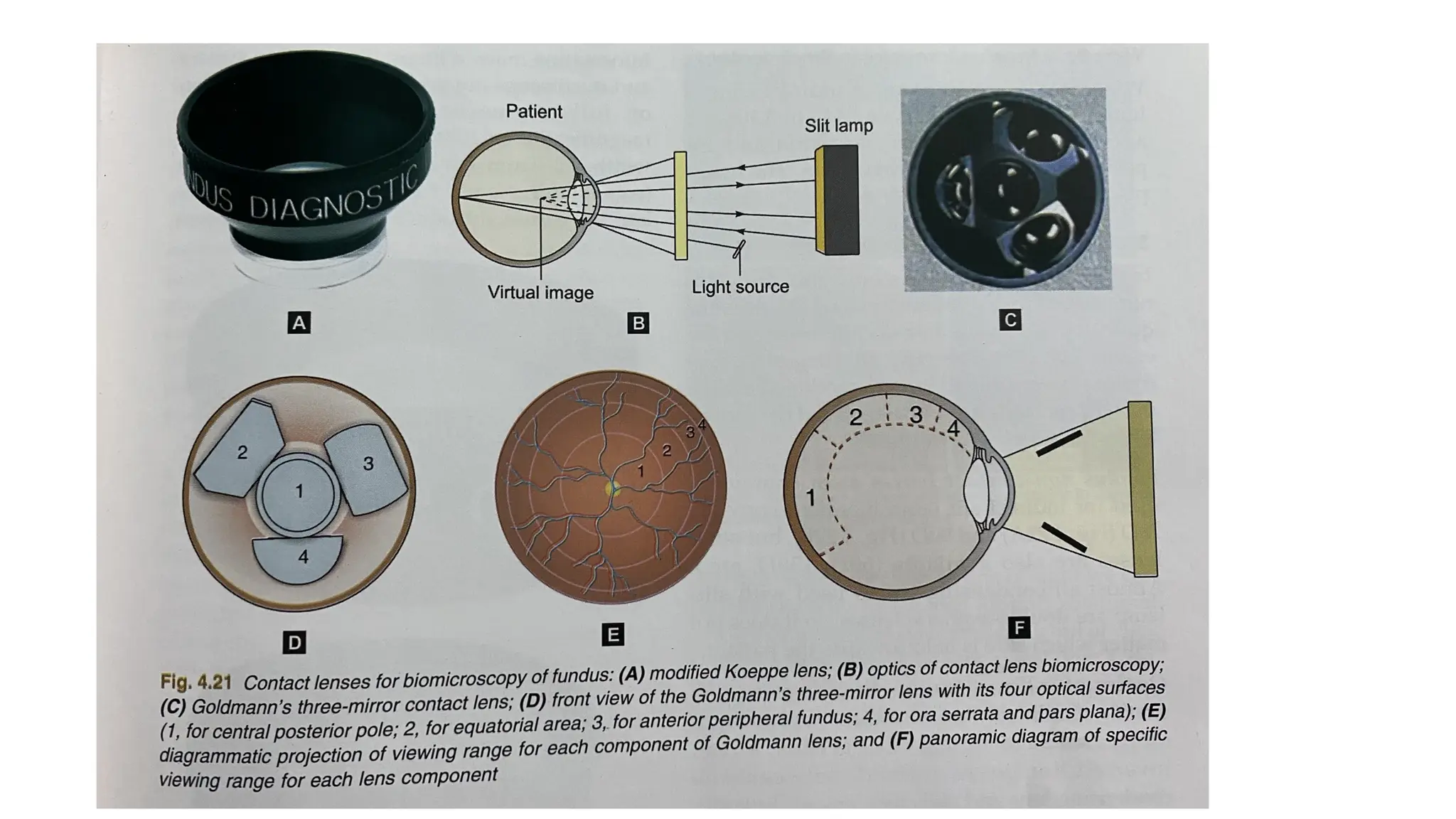
Contact lens biomicroscopyof fundus
• It combines stereopsis, high illumination and high msgnification with
advantage if slit beam.
• MODIFIED KOEPPE LENS EXAMINATION:
• It is a posterior fundus contact lens
• Provides virtual and erect image.
37.
Goldmann’s three mirrorcontact lens
examination
• Central contact lens with three mirrors placed in cone each with diferent angles of inclination
• Provides virtual and erect image.
• Technique:
• Dilate the pupils and instill topical anesthesia
• Insert coupling fluid into cup
• Ask patient to look up and insert the inferior rim of lens intolower fornix and press quickly
against cornea.
• when viewing different positions of peripheral retina, rotate axis of beam so it is always at
right angle to the mirror.
• To visualize the entire fundus rotate the lens for 3608 using tilted mirror
• 59- peripheral retina, 67- equatorial fundus, 738- area around posterior pole
39.
Indirect fundus biomicroscopy
•Non contact fundus biomicroscopy
• 78D and 90D
• Optics: same as of IDO , real and inverted image is formed between
condensing lens and objective lens of slit lamp
• Magnification: calculated by dividing power of eye by power of
lens( 60/90=0.66, minification of image
• By slit lamp magnified image is provided, 7.5X magnification with 90D
• Field of view:
• High powered lens provide larger field of view but lesser magnification.
40.
Technique
• Look foranterior segment
• Adjust slit lamp magnification of 10X, low illumination with slit width
of 2-3mm, fixed target.
• Hold the lens and focus the slit lamp beam, align image in center of
lens. Start fundus examination from peripheral fundus.
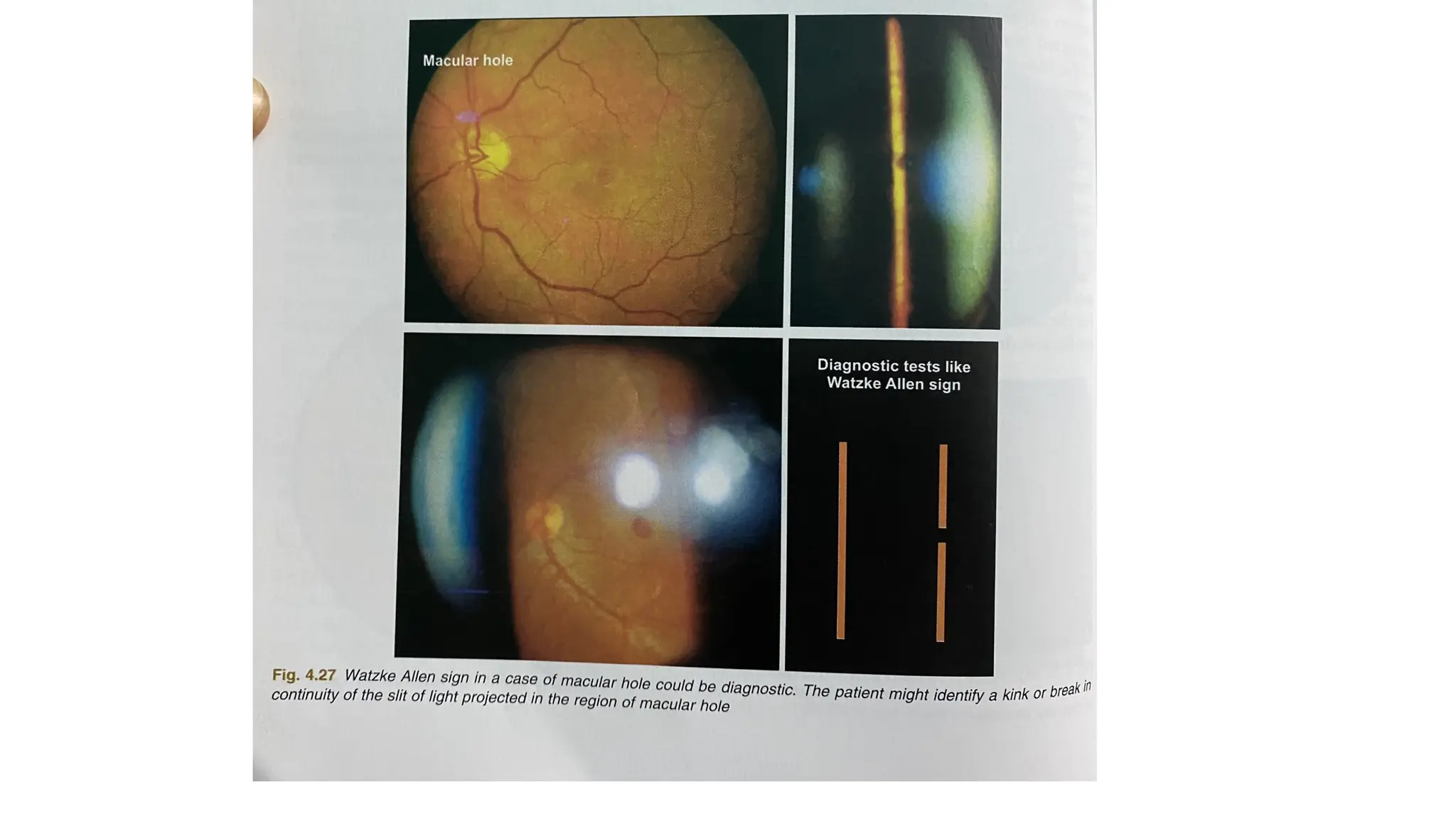
• Watzke allen sign: diagnostic of macular hole, we shine the slit of light
on hole patient sees kinking of slit or breaking of slit in center.
43.
Fundus camera
• Illuminationand observation pathways pass through different
portions of patient’s pupil to avoid reflection from cornea and from
surface of crystalline lens
• An inverted aerial image is reimaged on to film plane.
• 2 major components:
• Illumination system and observation and photography system
• It share one common point front or ophthalmoscopic lens.
44.
Modifications in funduscamera
• Fluorescein angiography system
• Digital fluorescein angiography system
• Wide field digital fundus fluorescein angiography
• Non mydriatic fundus camera
• Wide angle fundus cameras
• Television ophthalmoscopy
• Scanning laser ophthalmoscopy