Download to read offline
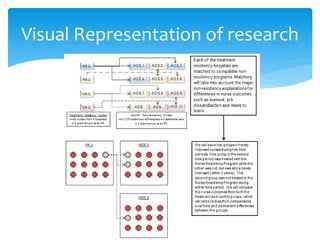
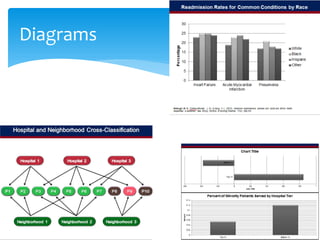

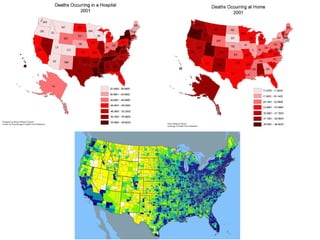




Egor Buharin has had a busy summer as a SUMR scholar mentored by Matthew D McHugh. He has worked on multiple research projects including analyzing end-of-life care costs and trends, California's nurse-to-patient mandate, and conducting nurse and patient surveys across 30 hospitals in the United Arab Emirates. Through these experiences, he has gained valuable skills in statistical programming, learned the challenges of organizing large datasets, and seen the potential impact of using empirical data to inform healthcare policy decisions internationally.



























































































