Emergency Medical Services
•Federal, state, and county systems.
• Establish, regulate, and monitor all components of Emergency care.
• Goals of the EMS:
1. Provide emergency care as quickly as possible.
2. Assure the “right client arrives at the right hospital in the least amount of
time”.
3.
Definition of EmergencyNursing
According to the ENA, the definition of emergency nursing is:
“the assessment, diagnosis, and treatment of perceived, actual or
potential, sudden or urgent, physical or psychosocial problems that
are primarily episodic or acute”.
4.
• Focused onurgent and critical care needs.
• Emergency nurses need special training, education,
experience, and expertise in assessing and identifying
health care problems in crisis situations.
Scope and Practice of Emergency Nursing
5.
• Nursing interventionsare accomplished interdependently under the
direction of a physician or nurse practitioner
• The emergency room staff work as an interdisciplinary team that
includes:
-Pre-hospital care providers
-Paramedics and EMTs
-Physicians
-Support staff
-Inclient unit staff
Scope and Practice of Emergency Nursing
6.
Legal Issues inthe ED
• Federal Legislation – any client must be treated regardless of their ability to
pay.
• COBRA – continuation of health insurance coverage following a life event
• Guidelines can vary by state
• EMTALA – medical screening must be done before gathering payment
information
• Client condition must be stabilized before transfer to another healthcare facility
• HIPAA
• Consent to Treat
• Mandatory Reporting
• Suspected abuse (signs), communicable diseases (syphilis, HIV, TB)
Motor Vehicle Crashes (MVC), animal bites (rabies), first time or
recurrent seizure activity (can’t drive for 6 months), food poisoning
(public health), death. Coroner’s case – leave all tubes, IV’s, etc. In place.
7.
• Chronic HealthProblems
• Primary Care
• Unhealthy Lifestyles
• Co-morbidities
• Economical Issues
• Don’t go to doctor until really sick
• Healthcare Access
• Who takes Medicaid, new clients
• Safety in ED’s – violence
The Changing ED Environment
8.
• Make safetythe first priority
• Ensure security and a safe environment
• Closely observe client and family members in
the event that they respond to stress with
physical violence
Priority Measures in the
Emergency Department
9.
• Assess theclient and family for psychological
function
• Plan client and family-focused interventions
Priority Measures in the
Emergency Department
10.
The ED isa temporary point on the continuum of care that
includes:
• Assessment – focused assessment
• Planning
• Interventions – teaching/discharge needs
• Evaluation of Care
• Community Resources
Continuum of Care
11.
Triage =
Sorting clientsby hierarchy based on the severity of their health
problems and the immediacy with which these problems must be
treated.
12.
Triage
• The triagenurse collects data and classifies the illnesses and/or
injuries into triage categories.
• Protocols may be initiated in the triage area.
• clients who are the most critically ill receive the most resources,
regardless of potential outcome
• 6 months to 1 year experience
13.
• Three Level
-Emergent…Highest Priority
-Urgent
-Non-urgent
• Five Level
-Resuscitation…immediate treatment
-Emergent
-Urgent
-Non-urgent
-Minor
Triage-ABCD
• Emergent-immediate threatto life
• Ex: respiratory distress, chest pain with diaphoresis, unstable vital
signs, stroke, active hemorrhage
• Urgent- major injuries that require immediate treatment
• Ex: severe abdominal pain, renal colic, displaced or multiple
fractures, complex or multiple soft tissue injuries, new-onset
respiratory infections especially pneumonia in older adults, new
onset abdominal pain
• Non-Urgent: minor injuries that do not require immediate treatment
• Ex: skin rash, strains, sprains, colds and simple fractures
ED TRIAGE
16.
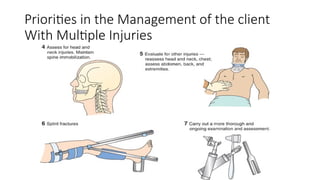
Primary Survey andResuscitation
Interventions
The primary survey organizes the order of
approach to the client by mnemonic device:
• (A) Airway/cervical spine
• (B) Breathing
• (C) Circulation
• (D) Disability
• (E) Exposure
If on the scene of a MVC, you must first survey the scene to
ensure your safety; then, do a primary survey.
17.
Secondary Survey
• Comprehensivehead-to-toe assessment to identify other
injuries or medical issues that need to be managed or that
impact the course of treatment.
18.
1) Age/pre-existing clientand environmental conditions
2) Do you remember the crash?
3) Were you the driver or the passenger?
4) Did you hit the steering wheel or dashboard? If so what part of body?
5) How fast was the vehicle going?
6) What did the vehicle hit?
7) Where is your pain?
Blunt Injuries From Falls
1) Age/pre-existing client and environmental conditions
2) How far did you fall?
3) What precipitated the fall?
4) What did you land on?
5) Where is your pain?
6) Self - reported loss of consciousness is not valid information
Examples of Questions to ask
19.
Gunshot Wounds
1) Age/pre-existingclient and environmental conditions
2) How long ago did the incident occur?
3) What were you doing when you got shot?
4) How many shots did you hear?
5) What did the gun look like?
6) Where is your pain?
Penetrating Wounds or Stab Wounds
1) Age/pre-existing client and environmental conditions
2) How long ago did the injury occur?
3) How many times were you stabbed?
4) What did the knife look like?
5) Where is your pain?
Examples of Questions to ask
20.
• Team approach
•Determine the extent of injuries and establish priorities of treatment
• Assume cervical spine injury / prevent further injury – CT before
removing C-collar
• Assign highest priority to injuries interfering with vital physiologic
function
Priorities of Care for the client With Multiple
Injuries
Trauma Center Level1
Elements of Level I Trauma Centers Include:
•24-hour in-house coverage by general surgeons, and prompt availability of care in specialties such as
orthopedic surgery, neurosurgery, anesthesiology, emergency medicine, radiology, internal medicine, plastic
surgery, oral and maxillofacial, pediatric and critical care.
•Referral resource for communities in nearby regions.
•Provides leadership in prevention, public education to surrounding communities.
•Provides continuing education of the trauma team members.
•Incorporates a comprehensive quality assessment program.
•Operates an organized teaching and research effort to help direct new innovations in trauma care.
•Program for substance abuse screening and client intervention.
•Meets minimum requirement for annual volume of severely injured clients.
24.
Trauma Center Levels– Level 2
Elements of Level II Trauma Centers Include:
•24-hour immediate coverage by general surgeons, as well as coverage by the
specialties of orthopedic surgery, neurosurgery, anesthesiology, emergency
medicine, radiology and critical care.
•Tertiary care needs such as cardiac surgery, hemodialysis and microvascular
surgery may be referred to a Level I Trauma Center.
•Provides trauma prevention and continuing education programs for staff.
•Incorporates a comprehensive quality assessment program.
25.
Trauma Center Levels– Level 3
Elements of Level III Trauma Centers Include:
•24-hour immediate coverage by emergency medicine physicians and the prompt availability of general
surgeons and anesthesiologists.
•Incorporates a comprehensive quality assessment program
•Has developed transfer agreements for clients requiring more comprehensive care at a Level I or Level II
Trauma Center.
•Provides back-up care for rural and community hospitals.
•Offers continued education of the nursing and allied health personnel or the trauma team.
•Involved with prevention efforts and must have an active outreach program for its referring communities.
26.
• Blunt orpenetrating injuries - surgery
• Abdominal trauma can cause massive life-threatening blood loss into
abdominal cavity
• Assessment
• Obtain history
• Perform abdominal assessment and assess other body systems for
injuries that frequently accompany abdominal injuries
Management of clients With
Abdominal Injuries
28.
• Assessment (cont.)
•Assess for referred pain that may indicate spleen, liver, or intra-
peritoneal injury
• Perform laboratory studies, CT scan, abdominal ultrasound, and
diagnostic peritoneal lavage
• Assess stab wound via sonography
Management of clients With
Abdominal Injuries
29.
Ensure airway,breathing, and circulation
Immobilize cervical spine
Continually monitor the client
Document all wounds
If viscera are protruding, cover with a sterile, moist saline dressing
Management of clients With
Abdominal Injuries (cont.)
30.
Hold oralfluids
NG to aspirate stomach contents
Provide tetanus and antibiotic prophylaxis
Provide rapid transport to surgery if indicated
Management of clients With
Abdominal Injuries (cont.)
• Dehydration fromheavy perspiration & inadequate fluid
consumption during heat exposure over hours to days
■ Prevention
■ Clinical manifestations resemble flu
Heat Exhaustion
34.
■ Stop physicalactivity, transfer to cool place, begin cooling
measures and rehydration
– Cold packs
– Soak in cool water
– Remove constrictive clothing
■ Sports drink or oral hydration solution
■ Plain water can worsen Na deficit
■ In clinical setting, NS if n/v
Heat Exhaustion- Treatment
35.
• A failureof the body’s heat regulating mechanisms.
• True medical emergency with high mortality rate without treatment
• Causes of Heat Stroke
• Exertion-Sudden onset; from strenuous physical activity in hot, humid
• Non-exertional (classic) – Occurs over period of time from chronic exposure to
hot, humid environment
• Elderly, very young, ill, or debilitated are at highest risk
Environmental Emergencies—Heat Stroke
36.
• Manifestations:
• CNSdysfunction (altered LOC, confusion), elevated
temperature, hot dry skin, anhidrosis (can’t sweat),
tachypnea, hypotension, and tachycardia, acid-
base imbalance, electrolyte imbalance
• Can cause death
37.
• Use ABCsand reduce temperature as quickly as possible
• Cooling methods
• Cool sheets, towels, or sponging with cool water
• Apply ice to neck, groin, chest, and axillae
• Cooling blankets – rectal temp monitor temp
• Immersion in cold water bath
• I’s and O’s – Indwelling catheter
• IV lines with NS
• Monitor electrolyte and acid/base imbalance
• Monitor for cerebral edema
• EKG
Management of clients With Heat Stroke
• Trauma fromfreezing temperature and actual freezing of fluid in the
intracellular and intercellular spaces
• Manifestations: extremity or area is hard, cold, and insensitive to touch; may
appear white or mottled; may turn red and be very painful as it is rewarmed.
Environmental Emergencies—Frostbite
Treatment:
• Controlled butrapid rewarming immersion in warm water.
• Administer analgesics for pain.
• Do not massage or handle the extremity; if feet are involved, do not allow
client to walk – safety falling.
43.
• Internal coretemperature is 35° C or less 95 F
• Elderly, infants, persons with concurrent illness, the
homeless, and trauma victims are at risk
• Alcohol ingestion increases susceptibility
• Hypothermia may be seen with frostbite
• Monitor continuously
Environmental Emergencies—Hypothermia
44.
• Manifestations:
• MILD:shivering, slurred speech, decreased muscle
coordination, impaired cognition, diuresis
MODERATE: muscle weakness, confusion, increased loss of
coordination, decreased clotting
SEVERE: bradycardia, severe hypotension, decreased RR,
dysrhythmias, decreased neuro reflexes, decreased pain,
acid/base imbalances
Management of clients With Hypothermia
45.
Use ABCs,remove wet clothing, and start rewarming
process quickly.
Re-warming
o Active core re-warming
Warm fluid administration
o Passive external re-warming
Warm blankets and heater devices
Cardiopulmonary Bypass – Severe Hypothermia
Management of clients With Hypothermia
46.
Continuous cardiacmonitoring
o Cold blood returning from the extremities has high levels
of lactic acid and can cause potential cardiac dysrhythmias
and electrolyte disturbances.
Management of clients With Hypothermia
• Leading causeof death in US
• Suffers primary respiratory impairment from submersion or
immersion in water or other liquid substances
• Heath teaching
• Constantly observation of people who can’t swim
• Do not swim alone
• Avoid alcohol when swimming or boating
• Safety equipment: life jacket, floatation devices, rope
Near Drowning
49.
• Assessment –water is aspirated into lungs
• Most Important
• Duration and severity of hypoxia
• Very cold water seem to have a protective effect – hypothermia might offer
some protection to hypoxia
• Hospital Care
• Airway and cardiopulmonary support, 02, ET, CPR, defibrillation, as necessary
• Gastric decompression – NG tube – will increase ventilation
• Can lead to ARDS
Near Drowning
50.
Altitude
Related
Illnesses
• Also knownas high altitude disease (HAD)
– Obese, chronic illness, dehydration, central nervous system
depressants increases risk
• Acclimatization – adaptation to high altitudes
• Acute mountain sickness (AMS)
– Headache, anorexia, n/v, chilled, irritable, apathetic
• High altitude cerebral edema (HACE)
– Dyspnea at rest
– Inability to perform ADLs
• High altitude pulmonary edema (HAPE)
– Most common cause of death associated with high altitude
– Manifestations: Poor exercise tolerance, persistent cough,
cyanosis of lips, tachycardia, tachypnea, crackles, pink-frothy
sputum
51.
• Exposure tolow partial pressure of oxygen in high elevations
• 18,000 feet are extreme altitudes – supplemental 02 is necessary
• Factors – obesity, cardiovascular problems, dehydration, alcohol use
• Issues with altitude sickness - high altitude cerebral edema,
pulmonary edema,
• Intervention – descend to lower altitude
• Treatment and Prevention – acetazolamide (Diamox) sulfa drug,
induces diuresis
Altitude Related Illness
52.
Lightning
Strikes
■ Cardiopulmonary andcentral nervous
systems profoundly affected
■ Asystole is most lethal initial effect on
cardiopulmonary system
■ Treatment is immediate CPR
■ No danger to rescuer from contact with victim
■ client Teaching Box-Preventing lightening
strikes
53.
• Look forinjury where struck with lightning AND where lightning
leaves the body (often on bottom of feet)
Lightning and burns
Poison isany substance that when ingested, inhaled, absorbed, or
applied to the skin injures the body by its chemical action.
Treatment goals:
◦ Remove or inactivate the poison before it is absorbed
◦ Provide supportive care in maintaining vital organ systems
◦ Administer specific antidotes
Management of clients With Poisoning
56.
• ABCs
• MonitorVS, LOC, ECG, and UO
• Assess laboratory values
• Determine what, when, and how much substance was ingested
• Assess signs and symptoms of poisoning and tissue damage
• Assess health history
• Determine age and weight
Assessment of clients With
Ingested Poisons
57.
Measures toremove the toxin or decrease its
absorption
◦ Use of emetics – syrup of ipecac no longer recommended
◦ Gastric lavage
◦ Activated charcoal
◦ Other measures may include diuresis, dialysis, or
hemoperfusion
Management of clients With
Ingested Poisons
58.
•Corrosive agents causedestruction of tissues by
contact; do not induce vomiting with corrosive
agents
Management of clients With
Ingestion of Corrosive Agents
59.
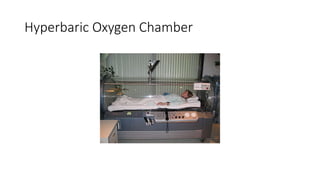
Inhaled carbonmonoxide
• Binds to hemoglobin as carboxyhemoglobin.
Manifestations: CNS symptoms
Treatment
◦ Get to fresh air immediately
◦ Perform CPR as necessary
◦ Administer oxygen: 100% or oxygen under hyperbaric
pressure
Monitor client continuously
Management of clients With
Carbon Monoxide Poisoning
• Severity ofthe injury depends upon the mechanism of action
of the substance, the penetrating strength and concentration,
and the amount of skin exposed to the agent
• Immediately flush the skin with running water from a shower,
hose, or faucet
– Lye or white phosphorus must be brushed off the skin
before flushing
Management of clients With
Chemical Burns
62.
• Protect healthcare personnel from the substance
• Determine the substance
• Some substances may require prolonged flushing/irrigation
• Follow-up care includes reexamination of the area at 24 hours, 72
hours, and 7 days
Management of clients With
Chemical Burns (cont.)
63.
• A suddenillness due to the ingestion of contaminated food or
drink
• Food poisoning may result in respiratory paralysis and death
• ABCs and supportive measures
• Determination of type of food poisoning
• Treat fluid and electrolyte imbalances
• Control nausea and vomiting
• Provide clear liquid diet and progression of diet after nausea and
vomiting subside
Management of
Food Poisoning
64.
• Acute alcoholintoxication:
• May result in death
• Maintain airway and observe for CNS depression and
hypotension
• Rule out other potential causes of the behaviors before it
is assumed the client is intoxicated
• Examine for withdrawal delirium, injuries, and evidence of
other disorders
Management of clients With
Substance Abuse
65.
Prioritize
• client #1: admitted with difficulty speaking and
hemiparesis 67-year-old African American
male
• client # 2: admitted with chest pain and shortness of
breath 62-year-old white male.
• client # 3: admitted with temp of 101 F with swollen and
inflamed right knee (had knee
replacement a week ago) 70-year-old Hispanic female
• client # 4: admitted with open fracture of the right arm 19-
year-old white male
• client # 5: admitted with a sucking chest wound 21-year-
old Hispanic male
• What healthcare team interventions would be initiated for
each of the above client?
66.
Prioritize
• client #1: Child with medication controlled asthma resents with
rapid, shallow respirations, and cyanosis around the lips and is
very anxious. He has been this way for about 20 minutes.
• client # 2: Woman with a cold for 3 days says she has no primary
care MD and must be seen immediately because she cannot
breathe. Her respirations are normal, pulse oxygenation
saturation is 100%, and she complains of sinus drainage.
• client # 3: Woman hit by a car whole she was riding her bike.
Instead of calling 911, a friend drove her to the ED. She is
complaining of neck pain and tingling in her upper extremities
since the injuries. She is beginning to have difficulty breathing.
• client # 4: Young boy was riding his skateboard arrives to the ED
with an angulated wrist. Pulses are normal, but the wrist is painful
• client # 5: An elderly woman presents with C/O 24 hours of
vomiting. Her vital signs are normal, but she is diaphoretic and
appears weak.
• How theclient is received and treated in the ED is important
to his or her psychological well-being
• Crisis intervention begins as soon as the client enters the
facility; the client should be seen immediately
• Goals are to provide support, reduce emotional trauma, and
gather evidence for possible legal proceedings
Crisis Intervention—Rape Victims
69.
• Accurate historytaking and documentation.
• Physical examination and collection of forensic
evidence.
• Role of the sexual assault nurse examiner (SANE)
• Maintaining “Chain of Custody” of evidence.
• Management:
• Maintainthe safety of all persons and gain control of the
situation.
• Determine if the client is at risk for injuring himself or
others.
• Maintain the person’s self-esteem while providing care.
• Determine if the person has a psychiatric history.
Psychiatric Emergencies
72.
Restraints in theEmergency Department
• Restraints may be necessary at times in order to keep a client from
harming themselves or others.
• Types of restraints:
• Leather
• Soft
• Chemical
• Joint Commission – National client Safety Goals.
• Health carefacilities are required by the Joint Commission on
Accreditation of Healthcare Organizations to create a plan for
emergency preparedness and to practice this plan twice a
year
Emergency Operations Plan
75.
• Essential componentsof the plan:
• An activation response
• An internal/external communication plan
• A plan for coordinated client care
• Security plans
• Identification of external resources
• A plan for people management and traffic flow
Emergency Operations Plan
76.
• Essential componentsof the plan:
• A data management strategy
• Deactivation response
• Post-incident response
• A plan for practice drills
• Anticipated resources
• Mass casualty incident planning
• Staff education for all of the above
Emergency Operations Plan
77.
“The key principleof disaster care is to do the greatest good
for the greatest number of clients, while the objective of
conventional medical care is to do the greatest good for the
individual client” (Flury, 2008)
Disaster Triage
78.
Disaster Triage Categories
DisasterCategories Disaster Tags
• Depending on Book:
• Red – Immediate/Emergent/Class 1
• Yellow- Delayed/Urgent/Class 2
• Green – Minor/Non-Urgent/Class 3
• Black- Expectant/Class 4
79.
In disaster situationswith large numbers of
casualties, triage decisions are based on the
likelihood of survival and the consumption of
resources.
Disaster Triage
80.
• Emergent orClass I- red tag: immediate threat to life
• Ex: airway obstruction or shock
• Urgent or Class II- yellow tag: major injuries that require treatment
• Ex: open fracture with distal pulse and large wounds, needs treatment within 20 minutes to 2
hours
• Nonurgent or class III- green tag: minor injuries that do not require immediate treatment
• Ex: walking wounded, closed fractures, sprains, strains, abrasions, contusions
• Expectant or class IV: black tag: expected and allowed to die
• Ex: head trauma, extensive full thickness body burns, high cervical spinal cord injury affecting
ventilation
Disaster Triage
• Tornadoes
• Hurricanes
•Fires
• Explosions
• Multiple vehicle accidents.
• Planes, trains, boats, and bus accidents.
• Terrorist attacks
Disasters that Produce Mass Casualties
83.
• Purpose:
To shieldthe health care provider from chemical,
physical, biological, and radiologic hazards that may
exist when caring for contaminated clients.
Personal Protective Equipment (PPE)
84.
• Biological agentsmay be delivered or spread in a
number of ways.
• Spread of agent may occur in areas thousands of
miles apart.
• Health care providers need to be aware of potential
signs of biological agent exposure; signs and
symptoms are similar to those of common disease
processes.
Precautions for Biological Terrorism Agents
85.
• Isolation practicesdepend upon the infecting agent
• Always use Standard Precautions (PPE)
• Some agents require Transmission-Based Precautions
• Terminal disinfection and disposal of wastes depends
on the infecting agent
Precautions for Biological Terrorism Agents
• Client Placement
•Negative pressure rooms may be necessary.
• clients with same exposure can be in same room.
• Respiratory Protection
• Client Transport
• Minimize the risk of infection to others.
• Environmental Control
• Ensure appropriate equipment cleaning.
Transmission Based Precautions
88.
• Chemical substancesthat quickly cause injury and/or
death.
• Types of Agents:
• Nerve agents - are damaging to the human body
because they cause a build-up of acetylcholine. This
causes constant triggering of the neurons and
therefore, constant contraction of muscles.
• Blood agents - preventing the exchange of oxygen and
carbon dioxide between the blood and the body's cells
• Vesicants
• Pulmonary agents
Chemical Weapons or
Chemical Exposure
89.
• Chemical substancesthat quickly cause injury and/or
death.
• Types of Agents:
• Vesicants - Blister agents burn and blister the skin
or any other part of the body they contact.
• Pulmonary agents - or choking agent, is a chemical
weapon agent designed to impede a victim's
ability to breathe.
Chemical Weapons or
Chemical Exposure
90.
• Agents varyin volatility, persistence, toxicity, and period of latency.
• Limit exposure.
• Decontaminate immediately and as close to the scene as possible.
Chemical Weapons or
Chemical Exposure
91.
• Anthrax isrecognized as the most likely biologic agent
to be used for bioterrorism.
• Infection caused by the bacterium Bacillus anthracis.
It can occur in four forms: skin, lungs, intestinal, and
injection. Symptoms begin between one day and two
months after the infection is contracted.
Anthrax
92.
• Cutaneous Anthrax
•Infection anthrax spores formed by Anthrax bacteria
• Local or systemic
• Inhalation Anthrax
• 100% fatal
• Does not spread person to person
• Manifestations:
• Early: Fever, fatigue, dry cough, mild chest pain
• Late: dyspnea, diaphoresis, stridor, hypoxia, high fever, pleural effusion,
hypotension, septic shock
• Rare natural occurrence
• Thus, act of terrorism and MUST be reported
• Treat with ciprofloxacin IV
Anthrax
93.
• Radiation exposuremay occur due to nuclear weapons,
nuclear reactor incidents, or exposure to radioactive
materials
• Exposure to radiation is affected by time, distance, and
shielding
Radiation Exposure
94.
• Triage outsidethe hospital.
• Cover floor and use strict isolation precautions to
prevent the tracking of contaminants.
• Seal air ducts and vents.
• Double bag all waste and put in a container labeled
radiation waste.
Radiation Decontamination
95.
• Staff Protection
•Water-resistant gowns, 2 pairs of gloves, caps, goggles,
masks, and booties
• Dosimetry devices
• Radiation Exposure
• Effects the Red Blood Cells (RBCs)
Radiation Decontamination
96.
• Provide activelistening and emotional support.
• Provide information as appropriate.
• Refer to therapists and other resources.
• Discourage exposure to media regarding the event.
• Encourage return to normal activities.
Managing the Short and Long Term Psychological Effects
of a Disaster
97.
• Critical incidentstress management (CISM)
• Programs that include education, field support, defusing,
debriefing, and follow-up components for disaster victims.
• Persons with ongoing stress reactions should be
referred to mental health specialists.
Managing the Short- and Long-Term Psychological
Effects of a Disaster