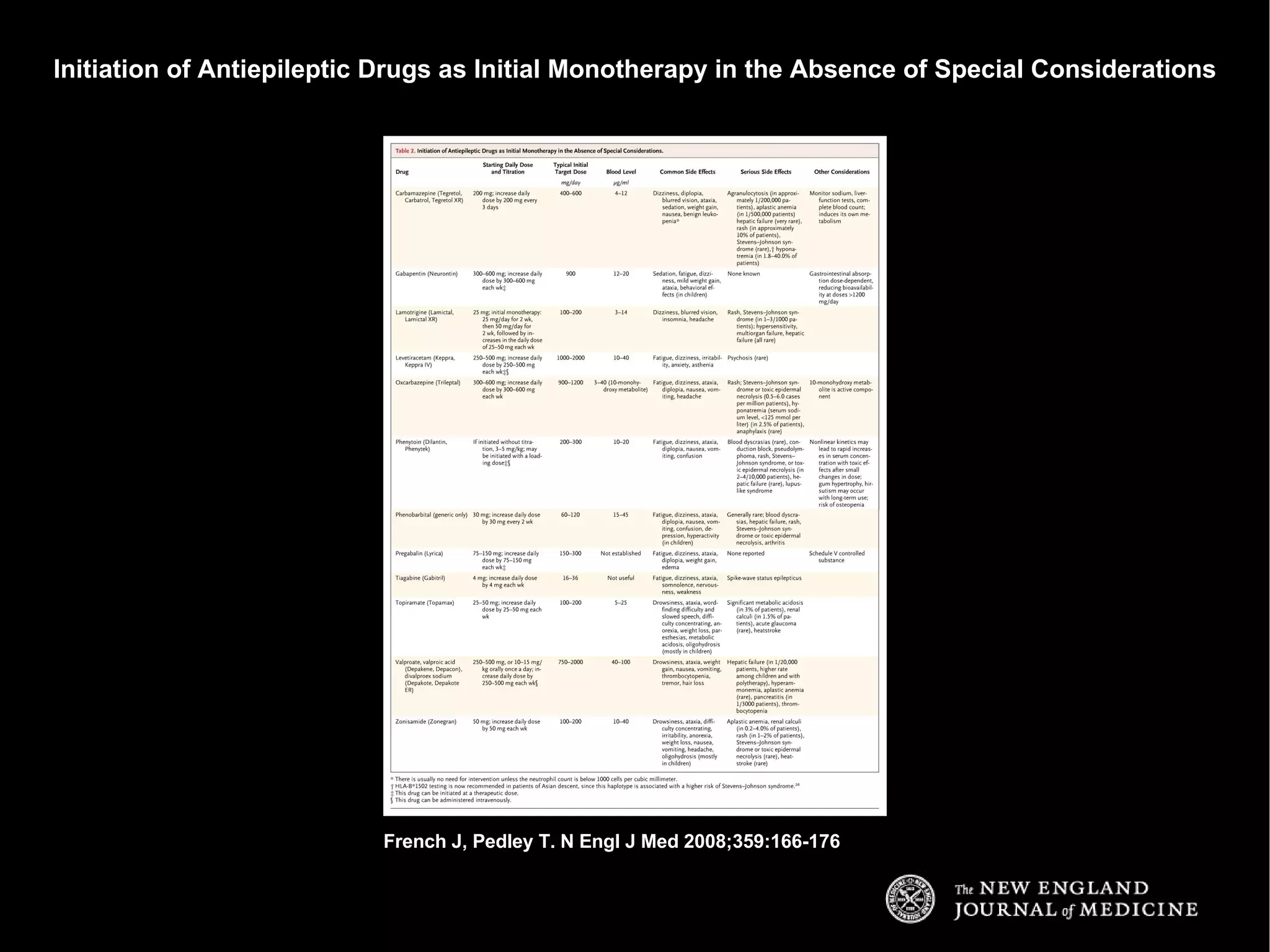
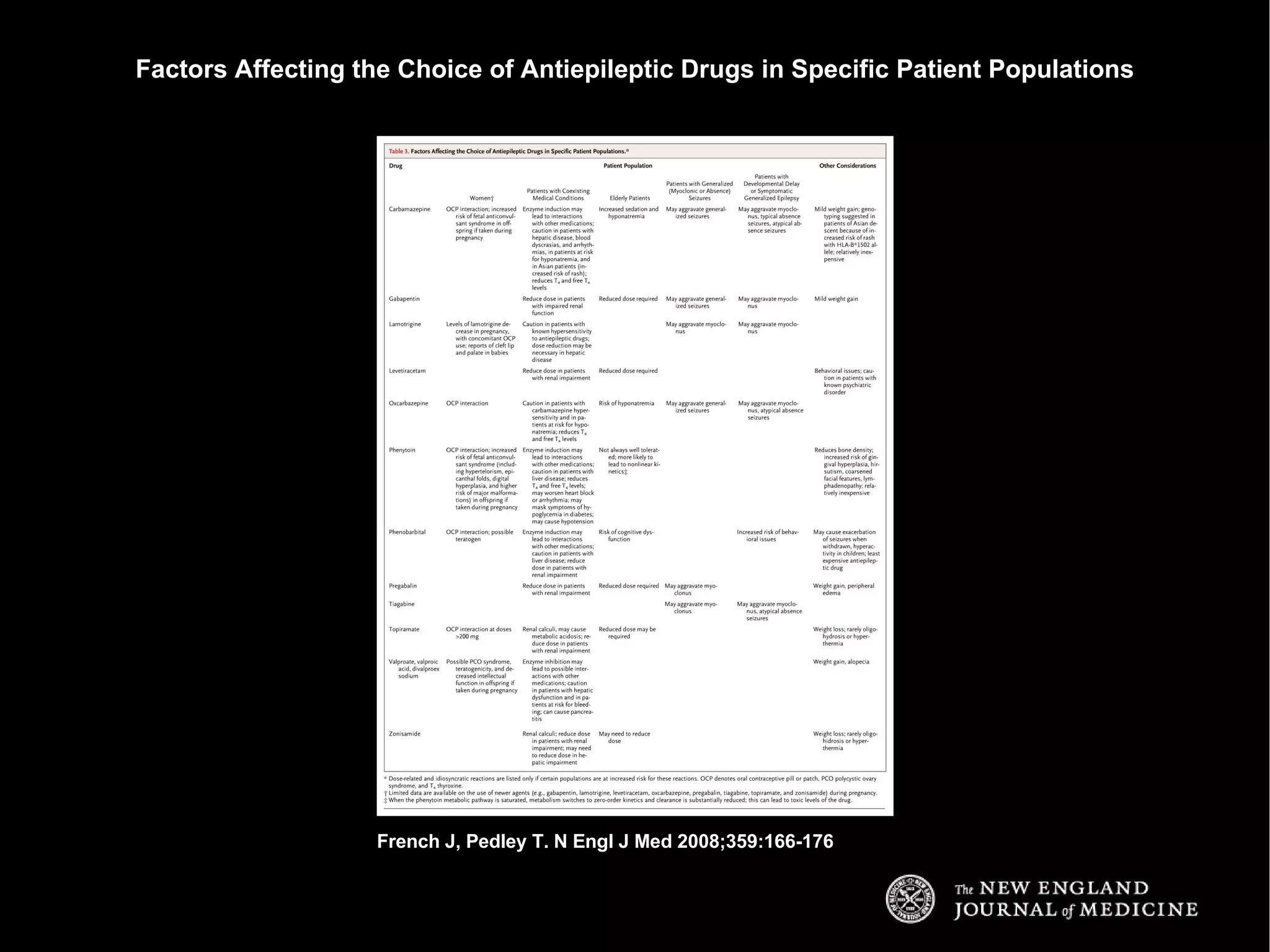
The document discusses the initial management and treatment of epilepsy. It describes a case of a 29-year-old woman who experienced two probable seizures. The summary recommends that she be evaluated through a neurological exam, EEG, and brain MRI. While test results may be normal, antiepileptic drug therapy should still be initiated given her history of seizures. A broad-spectrum drug is preferable since the type of seizures is unclear. Lamotrigine or levetiracetam are preferred initial treatments options due to safety considerations with her use of oral contraceptives.





































![Epilepsia Mexicali[1]](https://cdn.slidesharecdn.com/ss_thumbnails/epilepsiamexicali1-090509173319-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























































