Case Scenario
Male baby,born to 34 year old, G4 mother,
Maternal blood group:B Positive
Baby blood group: B Positive
Baby of X
4.
Antenatal History
Conception Spontaneous
ANCvisits 6-8
Booked and supervised At MRH
Periconceptional folic acid
intake
Taken
TT received Yes
Antenatal steroids Dexa covered
Maternal risk factors Hypothyroidism since 11th
week,Tab Thyronorm @ 125mcg/day
IHCP since 26 week ,Tab Udiliv 300mg,1 tab TDS
Investigations NT/NB scan- done(Uterine artery –Raised PI)Started Ecospirin,
Dual marker-High risk,Amniocentesis-Low risk for aneuploidy.
Antenatal scan at 26+6 week suggestive of UTD A2-3,Right AP
RPD 9.3 mm
Scan at 30 week suggestive of intrabdominal cyst ? Enteric
Duplication Cyst(1.8cm*1.1 cm) above bladder.
5.
Antenatal History
Gravida Details
Gravida1
(2017)
Spontaneous conception. Taken periconceptional folic acid. TIFFA normal.
History of IHCP(at 6 th month of gestation). Term, Male baby, NVD,3000g, weak
cry, NICU admission ,?sepsis. Expired on DOL 3 .
Gravida 2
(2017)
Ovulation induction conceived. Spontaneous abortion at 4 months. D& C not
done.
Gravida 3
(2020)
Spontaneous conception. Received periconceptional folic acid.NT NB not done.
TIFFA normal. H/O itching in mother. USG at 8 month suggestive of IUD ,
induced NVD. Birth weight 2.5 kg , no gross malformation.
6.
Antenatal History
Mode ofdelivery Em LSCS (Ind-Not willing for trial of labor)
Presentation Vertex
Date and time of delivery 3/02/22 at 3:40 pm
Birth weight 2745 grams (10-50th
centile on fenton’s chart)
Amniotic fluid Clear
APGAR scores 8,9,9
Gender Male
Gestation 36+3 weeks
Cord pH 7.336,Deficit- 1
Delivery room
management
Baby cried immediately after birth. Delayed cord clamping done. Routine care
given.
7.
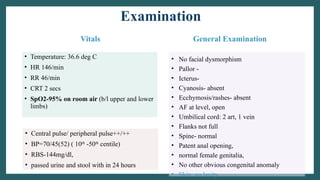
Examination
Vitals
• Temperature: 36.6deg C
• HR 146/min
• RR 46/min
• CRT 2 secs
• SpO2-95% on room air (b/l upper and lower
limbs)
General Examination
• No facial dysmorphism
• Pallor -
• Icterus-
• Cyanosis- absent
• Ecchymosis/rashes- absent
• AF at level, open
• Umbilical cord: 2 art, 1 vein
• Flanks not full
• Spine- normal
• Patent anal opening,
• normal female genitalia,
• No other obvious congenital anomaly
• Skin: no laxity
• Central pulse/ peripheral pulse++/++
• BP=70/45(52) ( 10th
-50th
centile)
• RBS-144mg/dl,
• passed urine and stool with in 24 hours
8.
Systemic examination
Respiratory CVSPer abdomen CNS
• Bilaterally
symmetrical chest
movements
• Bilaterally equal air
entry
• No added sounds
• S1 S2 present
• No murmur
• Soft
• No
organomegaly
• Cry/tone/activity –
good
• AF at level
9.
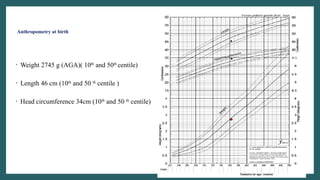
Anthropometry at birth
•Weight 2745 g (AGA)( 10th
and 50th
centile)
• Length 46 cm (10th
and 50 th
centile )
• Head circumference 34cm (10th
and 50 th
centile)
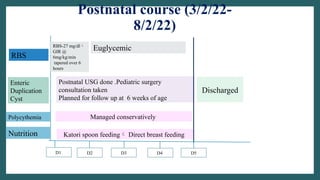
10.
D1
Postnatal USG done.Pediatric surgery
consultation taken
Planned for follow up at 6 weeks of age
Katori spoon feeding Direct breast feeding
Postnatal course (3/2/22-
8/2/22)
D4
Discharged
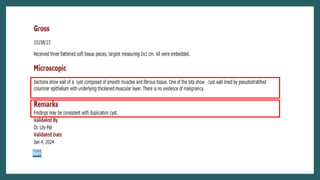
Nutrition
Enteric
Duplication
Cyst
D5
D3
D2
RBS
RBS-27 mg/dl
GIR @
6mg/kg/min
tapered over 6
hours
Euglycemic
Polycythemia Managed conservatively
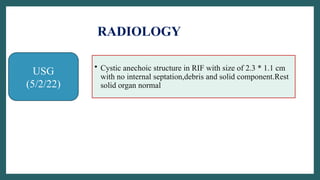
USG
(5/2/22)
• Cystic anechoicstructure in RIF with size of 2.3 * 1.1 cm
with no internal septation,debris and solid component.Rest
solid organ normal
RADIOLOGY
13.
Status at discharge
•Baby was 5 days old
• On breastfeed Ad lib
• Euglycemic
• Passing stools and urine adequately
• Supplements-vit D3,multivitamin
• Vaccinated
• Screenings :
• Hearing screen-B/l passed
• Pulse oximetry screening- passed
• TSH-5.64mIU
14.
Working Diagnosis
Late Preterm/36+3 week/Birth weight 2.745kg / AGA/
Male/LSCS/CIAB/ Polycythemia/Hypoglycemia/ Enteric duplication
cyst
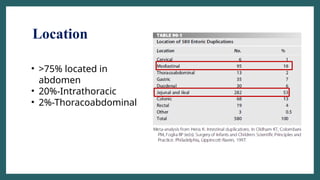
Introduction
• The firstreport was by Calder in 1733
• Rare developmental anomalies
• Originate anywhere along the alimentary tract from the tongue to the
anus.
• Incidence is 1:4,500 births
• Male>Female
• Most duplications are detected in children (antenatally or within first
two years of life) and fewer than 30% of all duplications are diagnosed
in adults.
Textbook of Pediatric Surgery,Arnold G Coran,7 th Edition
Pathophysiology
• In 1937,WilliamE. Ladd tried to simplify the nomenclature.
• Duplications of the alimentary tract had three characteristics:
(1) the presence of a well-developed coat of smooth muscle,
(2) an epithelial lining representing some type of intestinal tract mucosa
(3) intimate anatomic association with some portion of the
gastrointestinal tract
24.
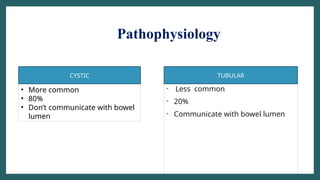
Pathophysiology
• Less common
•20%
• Communicate with bowel lumen
• More common
• 80%
• Don’t communicate with bowel
lumen
CYSTIC TUBULAR
25.
Pathophysiology
• On thebasis of part of alimentary canal attached to
1)Foregut
2)Midgut
3)Hindgut
• Ileum followed by oesophagus most common location
• The foregut duplications can be further divided into esophageal,
bronchogenic, and neurenteric depending on their embryological
origin.
26.
Embryology
• No singletheory
Partial/abortive twinning
Split notochord theory and anomalous
adhesion
Diverticula and canalization defects
Environmental factors
27.
Partial/Abortive Twinning
• Agroup of rare congenital anomalies of cloacally- derived structures–
eg, focal doubling of the GI tract at Meckel's diverticulum, extending to
anus, doubling of bladder, vagina, penis, sacrum, or lumbar vertebrae.
• Can be considered as a part of Caudal Duplication Syndrome.
• Along with genitourinary structure there is duplication of lower gastro
intestinal tract also.
• Explains the colorectal tubular duplication/duplication of hindgut that
are associated with duplication of genital and urinary structures.
28.
Partial/Abortive Twinning
• Thetiming of these twinning anomalies may explain the extent of the
twinning; for example, a split in the primitive streak earlier in gestation
followed by subsequent caudal growth may result in complete twinning
of the caudal end of the fetus.
• Split at a later date may result in only colonic duplication.
• Doesn’t explain other enteric duplication cyst abnormality.
29.
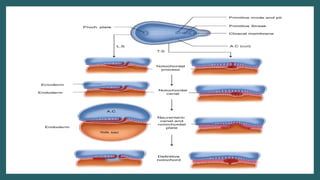
Split Notochord Theory
•In 3rd
week of gestation the notochord appears growing cephalad,
starting in close association with the endoderm, and normally separates
from the endodermal cells.
• During this separation, a gap sometimes appears in the notochord
through which
a diverticulum from the foregut (endoderm) can herniate by incomplete
detachment.
• These endodermal cells from the developing foregut then attach to
ectoderm to form a cyst, or, if they remain attached to the notochord, may
act as a barrier to later anterior fusion of the vertebral mesoderm,
resulting in anterior spina bifida of the type seen with neuroenteric cysts.
31.
Diverticula And CanalizationTheory
During development (solid stage) is progressively canalized leading to
formation of lumen
Diverticula exist in mammalian embryos.
During canalization diverticula regress .
Failure lead to enteric duplication cyst.
These diverticula are most frequently located in the ileum, the site of most
enteric duplications.
This mechanism may contribute to the formation of enteric duplications.
32.
Diverticula Theory
• Pitfalls:
•A)Heterotopic mucosa
• B)Duplication located on mesenteric site while but diverticula on
antimesenteric side
33.
Environmental Factors
Role unclear
Duringembryologic development, there is much tissue growth,
differentiation, migration,preprogrammed cell death, and tissue
adherence.
Other anomalies, particularly intestinal atresias, may be induced by
intrauterine vascular accidents..
Disorders of any of these mechanisms of development may be involved
in the formation of enteric duplications
Trauma & hypoxia-Duplication and twinning attempts in fetus
34.
History And PhysicalExamination
• Depends on location of cyst,type of cyst and presence of ectopic tissue.
• Neonates:
Antenatally diagnosed
Asymptomatic mass
Abdominal distension
Vomiting
Failure to pass meconium
35.
History And PhysicalExamination
• Majority present in childhood
• Mass in chest-Wheezing,pneumonia,dysphagia,chest pain(rare)
Cyst characteristic Signs and symptoms
Acute distension Severe abdominal pain
Heterotopic gastric
mucosa
Bleeding--Ulceration-Perforation
Acutely enlarging cyst ObstructionNausea,vomiting
Large duplication Localized volvolus
36.
History And PhysicalExamination
• Tubular
Cystic
• Generally
symptomatic
• Abdominal pain
• Chronic constipation
• Loading of intestinal
contents
37.
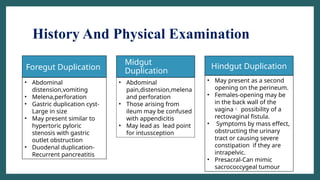
History And PhysicalExamination
• Midgut
Duplication
Foregut Duplication Hindgut Duplication
• Abdominal
distension,vomiting
• Melena,perforation
• Gastric duplication cyst-
Large in size
• May present similar to
hypertoric pyloric
stenosis with gastric
outlet obstruction
• Duodenal duplication-
Recurrent pancreatitis
• Abdominal
pain,distension,melena
and perforation
• Those arising from
ileum may be confused
with appendicitis
• May lead as lead point
for intussception
• May present as a second
opening on the perineum.
• Females-opening may be
in the back wall of the
vagina possibility of a
rectovaginal fistula.
• Symptoms by mass effect,
obstructing the urinary
tract or causing severe
constipation if they are
intrapelvic.
• Presacral-Can mimic
sacrococcygeal tumour
38.
Diagnosis
• Antenatal diagnosisby USG –Sensitivity of 20-30%
• History and physical examination-Boggy and mobile mass +/- tender
• Chest mass –Locally diminished breath sounds
• Lab examination –Anemia(if bleeding due to heterotopic tissue)
• Duplication cyst in head of pancreas-Raised amylase and lipase +clinical
features of pancreatitis
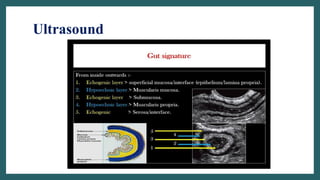
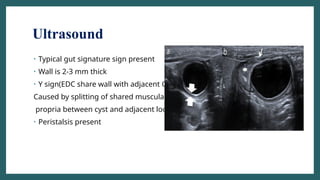
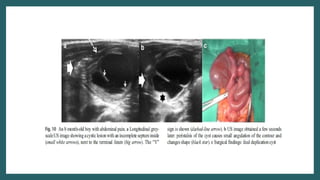
Ultrasound
• Typical gutsignature sign present
• Wall is 2-3 mm thick
• Y sign(EDC share wall with adjacent GIT.
Caused by splitting of shared muscularis
propria between cyst and adjacent loop)
• Peristalsis present
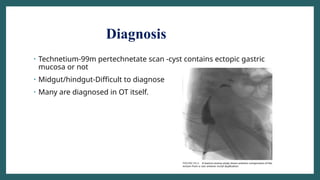
Diagnosis
• Technetium-99m pertechnetatescan -cyst contains ectopic gastric
mucosa or not
• Midgut/hindgut-Difficult to diagnose
• Many are diagnosed in OT itself.
45.
Histopathology
• A distinctmucosal lining and smooth muscle coat are characteristic
features
• The mucosal lining generally corresponds to some part of the
gastrointestinal tract.
• The mucosal lining may be heterotopic and may not correlate with the
adjacent bowel.
• Ectopic gastric mucosa is seen in approximately 20% to 30% of the
cases and is common in esophageal and midgut duplication cysts.
• Pancreatic mucosa is commonly observed in gastric duplications.
• Besides this, bronchogenic cysts have respiratory epithelium, cartilages,
and bronchial submucosal glands.
46.
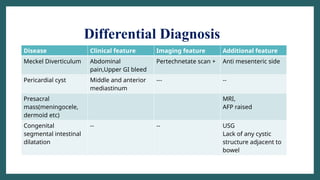
Differential Diagnosis
Disease Clinicalfeature Imaging feature Additional feature
Meckel Diverticulum Abdominal
pain,Upper GI bleed
Pertechnetate scan + Anti mesenteric side
Pericardial cyst Middle and anterior
mediastinum
--- --
Presacral
mass(meningocele,
dermoid etc)
MRI,
AFP raised
Congenital
segmental intestinal
dilatation
-- -- USG
Lack of any cystic
structure adjacent to
bowel
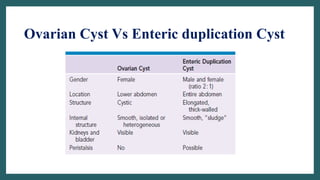
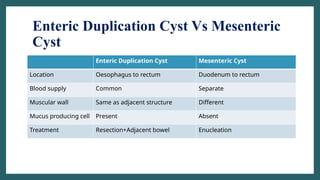
Enteric Duplication CystVs Mesenteric
Cyst
Enteric Duplication Cyst Mesenteric Cyst
Location Oesophagus to rectum Duodenum to rectum
Blood supply Common Separate
Muscular wall Same as adjacent structure Different
Mucus producing cell Present Absent
Treatment Resection+Adjacent bowel Enucleation
49.
Cervical Esophageal Duplication
•Very rare
• Presentation- Early in life with respiratory distress that can be life threatening.
• Intubation, rapid diagnosis, and intervention are often necessary.
• The mass may be appreciated on physical examination.
• Investigation of choice –CT scan
• Differential diagnosis-other cystic masses of the neck such as lymphatic
malformations and cysts of the airway or bronchial apparatus, or thyroglossal cysts.
• Treatment -excision
• If complete excision is not possible, the mucosa should be removed from the
duplication to allow for obliteration of the cyst cavity
51.
Thoracic and Thoracoabdominal
duplication
•20% of alimentary tract duplications -thorax or are
thoracoabdominal.
• Location-Lower half of posterior mediastinum
• Most fall in neuroenteric cyst group
• Frequently associated with vertebral anomalies
• Asympyomatic +/- Respiratory distress
• CT scan-Investigation of choice
• Treatment-Primrary excision
52.
Neurenteric Cyst
• Rareforegut duplications that also have connections to the spinal
canal, sometimes with the dura.
• Most common in thorax
• Cysts are formed when the notochord and foregut are in
apposition, either by failure of complete separation or by
herniation of foregut endoderm into the dorsal ectoderm.
• Investigation-MRI
54.
Abdominal Foregut DuplicationCyst
• Cystic,large,early presentation and frequently symptomatic
• Along greater curvature
• Palpable mass and vomiting
• In infants mimic hypertrophic pyloric stenosis(USG useful in
diagnosis)
• Symptoms due to mass effect and pressure on surrounding
structures gastric outlet obstruction,pancreatitis,GER. ulcer-
type symptoms from unbuffered hyperacidity with poor feeding
and abdominal pain.
• Treatment-Resection
57.
Duodenal Duplication
• Presentas biliary or pancreatic symptoms such as jaundice(d/d-choledochal
cyst) or pancreatitis.
• Vague symptoms- upper abdominal pain +/-nausea and vomiting
(80%),early satiety, or failure to thrive.
• Location- medial and posterior portions of the second and third portions of
the duodenum.
• These lesions most commonly contain duodenal or small intestinal mucosa
and may occasionally communicate with the lumen of the duodenum.
• Investigation-CT,ERCP and MRCP
• Treatment-Resection
58.
Midgut Duplication
• Cystic/tubularlocated on mesenteric side.
• Duplication shares its muscular wall and blood supply with the adjacent
intestine such that the duplication resides in the leaves of the mesentery.
• Communication with lumen of the intestine variable.
• Abdominal mass and pain
• Cystic duplication –Intussception-Volvolus
• Tubular duplication-Obstruction
• Ectopic gastric mucosa peptic ulceration, bleeding, or perforation.
• Ectopic gastric mucosa can be diagnosed by technetium-99m pertechnetate
59.
• Type 2(Intramesenterictype)
Type 1(Parallel Type)
• Duplication more to one
side of the mesentery with
an artery supplying the
duplication while the
opposite vessel went
directly to the native bowel
• More common
• 5% associated with spinal
abnromalities
• Duplication truly centered
in the mesentery and
vessels from both sides of
the mesentery traversed
the duplication to get to
the native bowel
• Less common
• 90% associated with
vertebral anamolies
Treatment –Surgical removal
Midgut Duplication
61.
Hindgut Duplication
• 17%of all duplication
• Simple cystic lesions in the wall or mesentery of the colon or quite
extensive, running the entire length of the colon and emerging on the
perineum as a separate opening, sometimes in the back wall of the
vagina.
• May be associated with abortive twinning anomalies and conjoined
twins,duplication of urinary tract abnormalities(may be associated with
lower spinal abnormalities.
62.
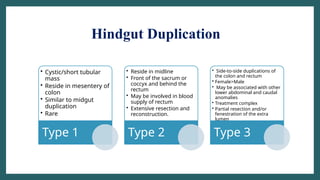
Hindgut Duplication
• Cystic/shorttubular
mass
• Reside in mesentery of
colon
• Similar to midgut
duplication
• Rare
Type 1
• Reside in midline
• Front of the sacrum or
coccyx and behind the
rectum
• May be involved in blood
supply of rectum
• Extensive resection and
reconstruction.
Type 2
• Side-to-side duplications of
the colon and rectum
• Female>Male
• May be associated with other
lower abdominal and caudal
anomalies
• Treatment complex
• Partial resection and/or
fenestration of the extra
lumen
Type 3
63.
Hindgut Duplication
• Asymptomatic
•Cystic mass,distension and obstructive symptoms
• Vague abdominal pain, constipation or failure to thrive.
• Rectovaginal fistula,urinary obstruction or retention
• Rectal duplications- pain or rectal obstruction
64.
Hindgut Duplication
• Difficultdiagnosis
• CT,MRI or Barium enema
• Rectal duplication (CT or MRI)-show the extent of the lesion, as well as
the relationship to the rectum, spine, and urinary tract.
• Currarino triad-presacral mass, rectal stenosis and sacral bony
anomalies
• Treatment-Surgical Removal
67.
Prognosis
• 85% ofpatients with enteric duplication cyst become symptomatic and
require surgery.
• Surgery –Curative
68.
Take Home Message
•Intestinal duplications may present in diverse ways and encompass a
wide variety of lesions from the neck to the anus.
• Can be simple and cystic, complex, multiple or tubular.
• Can have other anomalies associated with them including spinal and
genitourinary anomalies.
• Optimal treatment is resection
• With proper treatment there is excellent long-term outcomes and
quality of life.
69.
References
• Avery Textbookof Newborn,11 th Edition
• Textbook of Pediatric Surgery,Arnold G Coran,7 th Edition
• Anand S, Aleem A. Duplication Cyst. 2022 Oct 24. In: StatPearls [Internet].
Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 33232017.
• Frederic Chantraine, Boris Tutschek,24 - Abdominal Cyst2018,Pages 97-
105.e1
• Sangüesa Nebot C, Llorens Salvador R, Carazo Palacios E, Picó Aliaga S,
Ibañez Pradas V. Enteric duplication cysts in children: varied presentations,
varied imaging findings. Insights Imaging. 2018 Dec;9(6):1097-1106. doi:
10.1007/s13244-018-0660-z. Epub 2018 Oct 11. PMID: 30311079; PMCID:
PMC6269332
70.
NEURENTERIC CYSTS
• Neurentericcysts are rare foregut duplications that also have
• connections to the spinal canal, sometimes with the dura. Although
• they most commonly present as intrathoracic masses,
• they may also present as an intraspinal mass. The coexistence
• of a cystic posterior mediastinal mass with adjacent hemivertebrae
• should raise suspicion of a neurenteric cyst as well as
• anterior myelomeningocele.124 Neurenteric cysts are thought
• to form early in development when the notochord and foregut
• are in apposition, either by failure of complete separation or by
• herniation of foregut endoderm into the dorsal ectoderm
#27 Hox gene
Anorectal and urogenital system
A similar mechanism of anomalous
adhesions may also explain the rare long duplications arising
in the abdomen but seemingly tethered to the spinal column
high in the chest. Such adhesions would have to occur early,
possibly even before the appearance of the notochord, to
account for the long distances such duplications sometimes
traverse
#29 A similar mechanism of anomalous
adhesions may also explain the rare long duplications arising
in the abdomen but seemingly tethered to the spinal column
high in the chest. Such adhesions would have to occur early,
possibly even before the appearance of the notochord, to
account for the long distances such duplications sometimes
travers
#35 Failure to thrive,RD and vomiting
Mobile mass-50%^




![References
• Avery Textbook of Newborn,11 th Edition
• Textbook of Pediatric Surgery,Arnold G Coran,7 th Edition
• Anand S, Aleem A. Duplication Cyst. 2022 Oct 24. In: StatPearls [Internet].
Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 33232017.
• Frederic Chantraine, Boris Tutschek,24 - Abdominal Cyst2018,Pages 97-
105.e1
• Sangüesa Nebot C, Llorens Salvador R, Carazo Palacios E, Picó Aliaga S,
Ibañez Pradas V. Enteric duplication cysts in children: varied presentations,
varied imaging findings. Insights Imaging. 2018 Dec;9(6):1097-1106. doi:
10.1007/s13244-018-0660-z. Epub 2018 Oct 11. PMID: 30311079; PMCID:
PMC6269332](https://image.slidesharecdn.com/entericduplicationcyst-250308080957-cc2390fa-250812153450-fabd4b50/85/Enteric-duplication-cyst-etiology-and-management-69-320.jpg)