TỔNG ÔN TẬP THI VÀO LỚP 10 MÔN TIẾNG ANH NĂM HỌC 2023 - 2024 CÓ ĐÁP ÁN (NGỮ Â...
ENT LECTURES Combined.pdf
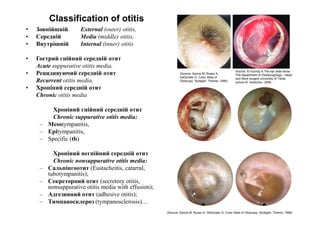
1. Classification of otitis
• Зовнійшній External (outer) otitis,
• Середній Media (middle) otitis,
• Внутрішній Internal (inner) otitis
• Гострий гнійний середній отит
Acute suppurative otitis media,
• Рецидивуючий середній отит
Recurrent otitis media,
• Хроніний середній отит
Chronic otitis media
Хроніний гнійний середній отит
Source: El-Guindy A.The ear slide show.-
The department of Otolaryngology - Head
and Neck surgery university of Tanta,
school of medicine.- 2006.
(Source: Sanna M, Russo A,
DeDonato G. Color Atlas of
Otoscopy. Stuttgart: Thieme; 1999)
Chronic suppurative otitis media:
– Mesotympanitis,
– Epitympanitis,
– Specific (tb)
Хроніний негнійний середній отит
Chronic nonsuppurative otitis media:
– Сальпінгоотит (Eustacheitis, catarral,
tubotympanitis);
– Секреторний отит (secretory otitis,
nonsuppurative otitis media with effusion);
– Адгезивний отит (adhesive otitis);
– Тимпаносклероз (tympanosclerosis)…
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
2. Гострий гнійний середній отит Acute otitis media
Local sign:
Complains:
• 1. Вушний біль (Otalgia, earache – 1st stage).
• 2. Виділення з вуха (Otorrhea - 2nd st.).
• 3. Зниження слуху (Hearing loss, deafness – 1-3rd st.).
• 4. Шум у вусі (Tinnitus 1-3rd st.).
Otoscopy:
• Гіперемія, випинання барабаної перетинки
(Hyperemic, thickened eardrum, bulging - 1st stage),
• Перфорація барабаної перетинки (Tympanic
• Перфорація барабаної перетинки (Tympanic
membrane perforation - 2nd stage),
• Слизово-гнійні виділення (muco-purulent discharg -
2nd stage).
Інфекційно-інтоксикаційний синдром (особливо у
дитячому віці)
(infectious-intoxicative syndrom (especially in
childhood)):
• Підвищення to тіла, інтокскація, лейкоцитоз…
• (Pyrexia, Intoxication, leucytosis ...) Source: El-Guindy A.The ear slide show.-
The department of Otolaryngology - Head
and Neck surgery university of Tanta,
school of medicine.- 2006.
3. Stages of Acute Otitis Media
1.1. Стадія доперфорації (prePerforative stage):
• Скарги: біль, зниження слуху, шум у вусі
• Отоскопія: гіперемія, потовщення барабаної перетинки
1.2. Предперфоративний период доперфоративноїх стадії
(prePerforative period of the prePerforative stage):
• Скарги: + нестерпний біль…
• Отоскопія : + випинання барабаної перетинки…
2. Стадия перфорации (perforative stage):
• Перфорация барабанной перепонки - оторрея
• Зниження слуху, шум у вусі
• Зниження слуху, шум у вусі
3. Наслідки (sequelae):
a) одужання;
b) хронізація
c) ускладнення:
1) мастоідити;
2) параліч лицьового нерва;
3) лабіринтити;
4) внутрішньочерепні...
Source: El-Guindy A.The ear slide show.-
The department of Otolaryngology - Head
and Neck surgery university of Tanta, school
of medicine.- 2006.
4. (Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
5. Acute otitis media
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of medicine.- 2006.
6. Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of medicine.- 2006.
7. Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of medicine.- 2006.
8. 3. Sequelae of Acute Otitis Media
3.1. Одужання (Healing - healthy ear):
- без залишкових ознак (full restoring of the
tympanic membrain, conductive system);
- кальціфікація барабанної перетинки
(calcification of the tympanic membrane);
3.2. Хронізація: (chronic otitis):
Хронічні гнійні перфоративні середні отити
(Chronic suppurative perforative otitis media):
- мезотимпаніт (mesotympanitis);
- епітимпаніт (epitympanitis).
Хронічні негнійні середні отити:
(Chronic nonsuppurative otitis media)
- Сальпінгоотит (Eustacheitis, catarral,
tubotympanitis);
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and
Neck surgery university of Tanta, school of medicine.- 2006.
tubotympanitis);
- Секреторний отит (secretory otitis,
nonsuppurative otitis media with effusion);
- Адгезивний отит (adhesive otitis);
- Тимпаносклероз (tympanosclerosis)…
3.3. Ускладнення (complications):
- Intratemporal:
1) мастоідити (mastoditis);
2) парез лицьового нерва
(facial nerve paralysis);
3) лабіринтити (labyrinthitis);
4) внутрішньочепні - Intracranial:
менінгіти, абсцеси мозку…
(meningitis, brain absces etc.)
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head
and Neck surgery university of Tanta, school of medicine.- 2006.
9. Sequelae & Complications of the Otitis Media
• Sequelae
a) healing and healthy ear,
b) chronic otitis (mesotympanitis, epitympanitis,
Atelectasis, Adhesive otitis, tympanosclerosis or perforative
otitis),
c) complications:
• Intratemporal Complications:
- Acute Mastoditis (1.4, 1.7, 1.8, 2.1, 2.2), Petrositis,
- Facial nerve paralysis,
- labyrinthitis (Local or diffuse).
1
- labyrinthitis (Local or diffuse).
• Intracranial Complications:
- Extradural abscess (1.2),
- Meningitis,
- Subdural abscess (1.1),
- Temporal lobe brain abscess (1.3),
- Cerebellar abscess (1.6),
- Lateral (sygmoid) sinus thrombosis (2.3),
- Otic hydrocephalus.
2
10. Management of Acute Otitis Media
1. Похідні карбол-гліцеринових вушних крапель (ear drops):
1st stage – феназон 0,5+лідокаїн 0,1+гліцерин 10 (Ототон)
2nd stage – антибіотик (не ототоксичний, без спирту, теплий) з
димексидом 25% або кортикостероідом.
2. Назальні (топічні) деконгестанти (nasal decogestans):
фармазолін 0,1% - 3 краплі 3 рази на добу в ніс 5(7) діб
3. НПЗЗ (nonsteroid antiinflamatory):
діклофенак натрія 0,05-0,15 1-3 р/д 3-5 діб після їжі, запивати
(Na diclofenaci 0,05-0,15 1-3 t/d 3-5 days after eating with water).
4. Антигістамінні (antihystamine): лоратадин 10 мг (Loratadinum 10 mg).
5.1. Watchful Waiting (72 hours) – спостереження без АБ-терапії
initial watchful waiting without antibiotic therapy
initial watchful waiting without antibiotic therapy
for healthy 2-year-olds or older children
with nonsevere illness (mild otalgia and fever <39°C).
5.2. Антибариальна терапія (аntibioticоtherapy):
Amoxicillin (80 mg/kg with clavulanate (0.125-0.75)
6. Surgical Measures:
Парацентез (tympanotomy, myringotomy)
Найчастіше в задньо-нижньому відділі
барабанної перетинки
(mainly in posterior-inferior quadrant
of the tympanic membranes)
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck
surgery university of Tanta, school of medicine.- 2006.
11. Особливості хронічних гнійних
перфоративних середніх отитів
Peculiaryties of Chronic Suppurative Otitis Media
• Постійна перфорація барабанної
перетинки (Chronic tympanic
membrane perforation).
• Постійна або рецидивуюча гноєтеча
(або ні).
Source: El-Guindy A.The ear slide show.- The department of
Otolaryngology - Head and Neck surgery university of Tanta,
school of medicine.- 2006.
або ні).
(Chronic or recurrent mucopurulent
otorrhea (or not)).
• Зниження слуху (hearing loss).
• Шум у вусі (Tinnitus).
• Грануляції, поліпи у вусі (granulation,
ear polip).
(Pain is not a usual feature like polyp or
granulation tissue formation).
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of
Otoscopy. Stuttgart: Thieme; 1999)
12. Chronic suppurative otitis media
Chronic mesotympanitis & Chronic epitympanitis
• Виділення з кров’ю, каріозним запахом, кусочками холестеатоми, кістковим піском,
лусочками епідермісу (bloodstained otorrhea, with cariotic smell, pieces of cholesteatoma, bone sand,
desquamous epithelium);
• Крайова перфорація у ненатягнутій частині (Marginal perforation in pars flaccida);
• Шорсткість кістки при ощупуванні стінок б/порожнини (probe test - rough bone of the tympanic
cavity walls);
• Вимивання канюлею Гартмана кусочків холестеатоми, кісткового піску, лусочoк епідермісу
(cholesteatoma, bone sand, desquamous epithelium by washing attic with Hartmann canulae);
• Поліпи, грануляції (polyp or granulation tissue formation);
• Руйнування кістки на КТ, овальна холестеатома на МРТ (bone destruction by X-rays
examinations CT, MRI);
• Змішана приглухуватість (conductive & sensoneural hearing loss by audiological investigation).
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head
and Neck surgery university of Tanta, school of medicine.- 2006.
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy.
Stuttgart: Thieme; 1999)
13. Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of medicine.- 2006.
14. • Remission
stages,
• Exacerbation
stages,
Chronic purulent epitympanitis
• External
meatus polips,
• cholesteatoma
in the external
meatus.
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
Source: El-Guindy A.The ear slide show.- The department of
Otolaryngology - Head and Neck surgery university of Tanta,
school of medicine.- 2006.
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
15. (Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
16. (Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
17. (Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
18. Treatment Summary for Otitis Media.
Acute Otitis Media (AOM) Otitis Media with Effusion
Chronic Suppurative Otitis
Media
Watchful
waiting
Up to 72 hours with analgesia /
antipyretics if nonsevere and
patient > 2 years old
For 3 months from onset or
diagnosis
not indicated
Medical
therapy
Antibiotics (amoxicillin) not indicated
Aural toilet and topical
antibiotics (quinolones)
Surgical
intervention
Myringotomy for refractory
AOM
VT insertion if unresolved after
3 months
Tympanoplasty
Cortical mastoidectomy in
nonresponding mastoiditis
Adenoidectomy on second VT
insertion
Tympanomastoid surgery if
refractory to medical
therapy
NI - not indicated; VT - ventilation tube.
19. Source: Menner Albert L. A Pocket Guide to the Ear / Thieme.- Stuttgart · New York.- 2003.- 145 p.
Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
Source: Hughes GB, Pensak MP. Clinical Otology. New York: Thieme; 1997.)
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of
medicine.- 2006.
Ballenger’s Otorhinolaryngology. Head and Neck Surgery / James B. Snow Jr,, John Jacob Ballenger // Sixteenth Edition.- BC Decker Inc.-
2006.- 1616 p.
20. Classification of otitis
• Acute Otitis Media Suppurative,
• Recurrent,
• Chronic Otitis Media
• External (outer),
• Media (middle),
• Internal (inner)
– Suppurative
• Mesotympanitis,
• Epitympanitis,
• Specific (tb)
– Nonsuppurative
• Eustacheitis (catarral,
tubotympanitis)
• Nonsuppurative Otitis media with
effusion (secretory otitis)
21. Factors Relevant to the Epidemiology
of Otitis Media
Environmental Factors
• Day-care attendance.
• Not being breast-fed.
• Exposure to tobacco
smoke.
• Seasonal variation in
respiratory infections.
• Host Factors.
Genetics
• Immunodeficiency.
• Birth defects.
• Cleft palate.
• Down syndrome.
23. Stage of Acute Otitis Media
• 1. Stage before perforation (preperforative)
• earache
• hearing loss
• tinnitus
Otoscopy
• thickened hyperemic tympanic membrane
• immobile on pneumatic otoscopy.
• 2. Stage after perforation (perforative)
• spontaneous rupture
of the tympanic membrane
or after myringotomy
• resulting in otorrhea
• 3. Sequelae of Acute Otitis Media
a) healthy ear
b) chronic otitis
(Adhesive or perforative otitis media)
c) complications:
- Intratemporal Complications:
1) Mastoditis;
2) Facial nerve paralysis;
3) Suppurative labyrinthitis;
4) - Intracranial Complications:
(meningitis, brain abscecc etc.)
24. Treatment of Acute Otitis Media
1. Ear drops
1st stage - Carbol-glycerinici ear drops (Otipax)
2nd stage - Antibiotoc with corticosteroid or antibiotic with 25%
dimetylsulfoxid
2. Nasal drops (local or topical decongestans)
or general decongestans (pseudoephedrini hydrochloridi
3. Antibiotic Therapy
- Amoxicillin (80 mg/kg/d given in three divided doses for 10 days)
remains the first-line therapy,
- In resistant cases, amoxicillin (0.5-0.8) should be given in
combination with clavulanate (0.125-0.75).
or
• Watchful Waiting (72 hours)
initial watchful waiting without antibiotic therapy
for healthy 2-year-olds or older children
with nonsevere illness (mild otalgia and fever <39°C)
4. Adjunctive Therapy
• analgesics and antipyretics
5. Antihistamine, antiallergic
6. Surgical Measures
• - myringotomy
25. Essentials of Diagnosis “Acute Kataral Otitis Media”
“acute eustacheitis”, “acute tubotympanitis”
– Local sign:
• Acute katar of airways
(Acute rhynopharyngitis or
rhynosinusitis).
• 1. Hearing loss (deafness).
• 2. Tinnitus.
• 3. Fluctuation of hearing
Otoscopic:
• Concave tympanic membrane:
– General sign:
• If rhynosinusitis is viral
26. Management of the “Acute Kataral Otitis Media”
“acute eustacheitis”, “acute tubotympanitis”
• 1. Treatment of acute katar of
airways.
• 2. Intranasal (local) or general
decongestant.
• 3. Eustachian tube inflation:
– 1. Toinby procedure.
– 2. Valsalva’s procedure.
– 2. Politzerisation.
– 3. Catheterisation and inflation
Technics of Politzerisation.
28. Peculiarity of the acute middle otitis in childhood
– General sign (always):
• 1. Intoxication,
• 2. Pyrexia,
• 3. Meningismus
• 4. Dyspepsia, meteorismus.
• 5. Lungs insufficiency.
• 6. Weight insufficiency,
• 7. More often middle otitis then in
adult (micsoid tissue, peculiarity of
Eustachian tube)
– Local sign:
• 1. “Tragus” sign positive.
• 2. “rumination” (“mastication”)
sign positive
• 3. Normal eardrum with middle otitis.
• 4. More often diagnostic
paracentesis.
• 4. Hyperemia without middle otitis.
29. Peculiarity of the acute viral otitis media
– Local sign:
Otoscopic:
• 1. Hemorrhage on the
normal tympanic
membrane,
• 2. Vesicles with water-like
fluid or hemorrage,
• 3. Sensoneural hearing
loss.
– General sign:
• Pyrexia,
• Intoxication.
30. Peculiarity of the Tb otitis
– Local sign:
– Otoscopic:
• 1. Multiply perforstions.
• 2. Discharge like Cheese.
– X-rays examination
• 3. Bone Secvestration.
– General Tb sign:
• The lungs focus,
• Intoxication.
31. Sequelae & Complications of Otitis Media
• Sequelae
a) healthy ear
b) chronic otitis (Atelectasis, Adhesive,
Tympanosclerosis or perforative otitis media)
c) complications:
• Intratemporal Complications:
- Acute Mastoditis
- Petrositis
- Facial nerve paralysis
- Local or diffuse Suppurative labyrinthitis
• Intracranial Complications:
- Meningitis,
- Subdural abscess,
- Extradural abscess,
- Temporal lobe of brain abscess,
- Cerebellar abscess,
- Lateral (sygmoid) sinus thrombosis,
- Otic hydrocephalus
32. Chronic Suppurative Otitis Media
• Chronic or recurrent
otorrhea or both.
• With pain (earache) or not
• Hearing loss.
• Tinnitus.
• Chronic tympanic
membrane perforation.
33. Pathogenesis of Chronic Suppurative Otitis Media
There are two main mechanisms by which a chronic perforation can
lead to continuous or repeated middle ear infections:
• 1) Bacteria can contaminate the middle ear cleft directly
from the external ear
because the protective physical barrier of the tympanic membrane is lost.
• 2) The intact tympanic membrane normally results in a middle ear "gas
cushion," which helps to prevent the reflux of nasopharyngeal secretions
into the middle ear via the eustachian tube.
The loss of this protective mechanism results in the increased exposure of
the middle ear to pathogenic bacteria from the nasopharynx.
34. Symptoms and Signs of Chronic Suppurative Otitis Media
• history of otorrhea,
intermittent or
continuous,
• hearing loss,
• discharge is usually
mucopurulent,
• polyp or granulation
tissue formation,
• bloodstained
otorrhea,
• Pain is not a usual
feature
35. Otitis chronica with cholesteatoma
• Retraction of the
tympanic membrane
with a squamous
debris collection or a
whitish mass behind
an intact tympanic
membrane.
• Squamous epithelium
in the middle ear or
mastoid.
Testing includes computed tomography (CT) scanning
36. Chronic suppurative otitis media
Chronic mesotympanitis & Chronic epitympanitis
(or cholesteatomic or malignant)
• Bloodstained otorrhea, with bad cariotic smell, pieces of
cholesteatoma, bone sand, desquamous epithelium,
• Marginal perforation in pars flaccida,
• Probe test (Rough bone of the tympanic cavity walls),
• Hartmann test (find the cholesteatoma, sand bone, desquamous
epithelium by washing attic),
• Polyp or granulation tissue formation,
• Bone destruction by X-rays examinations,
• Conductive & sensoneural hearing loss by audiological investigation,
37. Special Tests for diagnostic
Chronic Suppurative Otitis Media
• A swab of the discharge should be sent for culture and
sensitivity, preferably before beginning antimicrobial
therapy.
• If granulations are severe and unresponsive to antimicrobial
therapy, then chronic granulomatous conditions such as
- Wegener granulomatosis,
- mycobacterial infection,
- histiocytosis X, and
- sarcoidosis
should be considered.
Biopsy of the granulation or polyp in these
circumstances is recommended.
38. Pathogenesis of cholesteatoma
Acquired Cholesteatoma
• Cholesteatoma is the presence of squamous epithelium in the
middle ear, mastoid, or epitympanum.
• Primary acquired cholesteatoma is the most common of these
types and forms as a retraction of the tympanic membrane. In most
cases, the retraction occurs in the pars flaccida, although pars tensa
retractions can also occur.
• Secondary acquired cholesteatoma forms as a result of either
squamous epithelial migration from the tympanic membrane or
implantation of squamous epithelium into the middle ear during
surgery, such as ventilation tube placement or tympanoplasty.
Congenital Cholesteatoma
• Cholesteatomas that occur without tympanic membrane retraction or
implantation of squamous epithelial material are considered to be
congenital in origin. This type comprises a minority of cholesteatoma
cases.
• It is classically defined as an embryonic rest of epithelial tissue in
the ear without tympanic membrane perforation and without a
history of ear infection.
39. Clinical Findings (Symptoms and Signs) Patients with
cholesteatomas
Patients with acquired cholesteatomas typically present with
• recurrent or persistent purulent otorrhea and
• hearing loss.
• Tinnitus is also common.
• vertigo or dysequilibrium can result from the inflammatory process in the middle ear or, in rare
cases, from direct labyrinthine erosion by cholesteatoma.
• Facial nerve twitching, palsy, or paralysis can also result from the inflammatory process or from
mechanical compression of the nerve.
Physical findings are usually diagnostic in cases of acquired cholesteatoma.
• In primary acquired cholesteatoma, there will be a retraction of the pars flaccida in most
cases
• retraction contain a matrix of squamous epithelium,
• purulent otorrhea,
• polyps and
• granulation tissue,
• and ossicular erosion.
• In secondary acquired cholesteatoma, the findings depend on the cause. If the
cholesteatoma developed from a tympanic membrane perforation, the squamous epithelial matrix, keratin
debris, or both are usually visible through the perforation.
• Congenital cholesteatomas are usually asymptomatic until the mass grows to a sufficient size
that the ossicular chain function becomes disrupted and hearing loss develops.
40. Surgical Procedures for Cholesteatoma
Procedure End Result Advantages after
Surgery
Disadvantages after
Surgery
Tympanoplasty (canal
wall up) with
mastoidectomy
Ear canal with
tympanic
membrane
Low risk of otorrhea Risk of recurrent pars
flaccida
cholesteatoma
Atticotomy Ear canal with
tympanic
membrane and
defect into
epitympanum
Intermediate risk of
otorrhea
Risk of recurrent pars
flaccida
cholesteatoma
Modified radical
mastoidectomy
(canal wall down)
Mastoid cavity with
tympanic
membrane
Low chance of
recurrent pars
flaccida
cholesteatoma
Significant risk of
otorrhea
Radical
mastoidectomy
(canal wall down)
Mastoid cavity
without tympanic
membrane
Low chance of
recurrent pars
flaccida and pars
tensa
cholesteatoma
Significant risk of
otorrhea and poor
hearing
41. Treatment Summary for Otitis Media.
Acute Otitis Media (AOM) Otitis Media with Effusion
Chronic Suppurative Otitis
Media
Watchful
waiting
Up to 72 hours with analgesia
/ antipyretics if
nonsevere and patient > 2
years old
For 3 months from onset or
diagnosis
not indicated
Medical
therapy
Antibiotics (amoxicillin) not indicated
Aural toilet and topical
antibiotics (quinolones)
Surgical
interven
tion
Myringotomy for refractory
AOM
VT insertion if unresolved
after 3 months
Tympanoplasty
Cortical mastoidectomy in
nonresponding
mastoiditis
Adenoidectomy on second
VT insertion
Tympanomastoid surgery if
refractory to medical
therapy
NI - not indicated; VT - ventilation tube.
42. Local or diffuse Suppurative labyrinthitis
Local labyrinthitis:
• Caused epitympanitis,
• Fistule of the ampullae of the horizontal
semicircular canal,
• Fistule symptom,
• Treatment like epitympanitis – radical
mastoidectomy
Diffuse labyrinthitis: - Serous.
- Suppurative.
Diffuse Serous:
ill side
Contralatreral side
Contralatreral side
Contralatreral side
Contralatreral side (by
both hand)
Time more then 40 sec
Less then 50 ml
Diffuse purulent:
Contralatreral side
ill side
ill side
ill side
ill side (by
one hand)
Time more then 40 sec
More then 50 ml
Sign
Direction of nystagmus
Direction of Falling
Falling down in static tests
Deviation in Dynamic tests
Deviation in coordinative
tests (finger-nose test)
Rotatory test
Caloric test
43. Classifacation of the
mastoiditis & paramastoiditis
• Acute,
• Subacute,
• Chronic,
• Latent,
Mastoiditis:
• Tipical form,
• Tip form,
• Perisinuosus abscess,
Paramastoiditis:
• Subperiostal abscess,
• Zygomaticitis,
• Occipititis,
• Squamitis,
• Petrositis,
• Apicitis etc.
44. Acute mastoiditis
General sign of the inflamatory process:
• Intoxication, hight temperature, leucocytosis etc.
Sign of otitis (acute or chronic):
• (earache, discharge, tinnitus, hearing loss).
Local common sign of the mastoiditis:
• Painful palpation of the mastoid,
• Thickness soft tissue under mastoid,
• X-rays sign (cells shadow),
• Thickness of the posterior-superior part the bone part of
the external meatus,
Special Local sign of the mastoiditis:
It depend on the localisation:
• Tip form,
• Perisinuosus abscess,
• Zigomaticitis,
• occipititis,
• squamitis,
• petrositis,
• Apicitis etc.
45. 1. Surgical treatment:
It depend on the cause of the
mastoiditis!!!
• If mastoiditis was caused by acute otitis
the patients needs in simple
mastoidotomy (“Shwart’s or cortical
mastoidectomy”).
• If mastoiditis was caused by chronic
otitis the patients will be treated by
radical mastoidectomy.
2. Conservative treatment:
• Antibiotics (general & local),
(especially lincosamine group),
• Dehydratation,
• Detoxication,
• Antiinflammatory remedies,
1. Management of the mastoiditis
46. 1. Selection of Surgery otogenic any complications:
• If mastoiditis was caused by acute otitis the patients needs in simple
mastoidotomy (“Shwart’s or cortical mastoidectomy”).
• If mastoiditis was caused by chronic otitis the patients will be treated by
radical mastoidectomy.
2. Management of the mastoiditis
51. Otogenic extradural abscess
1. Sign of Acute or Chronic Otitis
media (earache, purulent discharge,
tinnitus, hearing loss).
2. Sign of Acute Mastoditis (painful
mastoid, thickness of posterior-
superior bony part of external meatus).
3. Local sign of extradural abscess:
combination of
- cistern sign (a lot of purulent
discharge) with
- pus pulsation
(double sign)
52. Otogenic meningitis
1. General Inflammatory sign:
- Intoxication,
- hypertermia,
- leucocytosis…
2. Meningeal sign:
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
3. Sign of increasing intracranial pressure:
- headache without benefit after using analgetics
or with nasea, vomiting,
- bradycardia,
- papilloedema (swelling of papilla of eyes
nerves)
4. Local sign of brain lession:
- hemiparesis…
53. Otogenic temporal lobe abscess of brain
1. General Inflammatory sign:
- Intoxication, hypertermia, leucocytosis…
2. Sign of increasing intracranial pressure:
- headache without benefit after using
analgetics or with nasea, vomiting,
- bradycardia,
- papilloedema (swelling of papilla of eyes
nerves)
3. Meningeal sign:
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
4. Local sign of brain lession:
- amnestic, motor or sensorial aphasia (left
side if patient is right-handed,
- contralateral paresis,
- dilated pupils, ptosis and lateral rectus
paralysis,
- homonymous hemianopia
54. Stages of the brain abscess:
1. Invasive stage - stage of encephalitis.
2. Latent stage - stage of almost no
symptoms.
3. Manifest stage - stage of raised
intracranial tension.
4. Terminal stage - stage of rupture.
on lumbar puncture, there is great
pressure of cerebrospinal fluid and
greater danger of coning of the medulla.
55. Otogenic cerebellar abscess
1. General Inflammatory sign:
- Intoxication, hypertermia, leucocytosis
2. Sign of increasing intracranial pressure:
- headache without benefit after using
analgetics or with nasea, vomiting,
- bradycardia,
- papilloedema (swelling of papilla of eyes
nerves)
3. Meningeal sign:
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
4. Local sign of cerebellar lession:
- 1. Falling down in static tests.
- 2. Deviation in Kynetic tests.
- 3. Deviation in coordinative tests (finger-
nose test )
- 4. Ipsilateral asynergia (dysdia-
dochokinesis).
- 5. Muscles hypotonia (flaccidity).
- 6. Nystagmus (continuous, big amplitude,
any directions till diagonalic…)
56. Otogenic lateral sinus trombosis signs
1. General Inflammatory sign:
- Intoxication, hypertermia, leucocytosis
And triad:
- chills (shivering) and fever,
- sweating (perspiring),
- aperiodic chills&fever and sweating,
2. Sign of Acute or Chronic Otitis media:
(earache, purulent discharge, tinnitus, hearing loss).
3. Sign of Acute Mastoditis:
- painful mastoid,
- thickness of posterior-superior bony part of
external meatus.
4. Local sign:
1. Obstructive symptoms
- Tobey-Ayer or Queckenstedt’s test (lumbar puncture and
digital pressure on the internal jugular vein on the healthy
side).
2. Infective symptoms (swinging temperature with rigors at
irregular intervals, formation of pyaemic abscesses in various
parts of the body chiefly lungs and joints, positive blood
cultyre, enlarged spleen and marked leucocytosis)
- Greisinger’s sign (If the mastoid emissary vein gets
involved, there is oedema and tenderness over its site).
57. Stage of the otogenic lateral sinus trombosis
1. The initial stage of attack when the vein wall
is inflamed and there is a mural clot inside it.
2. Stage of complete obliteration of the sinus
with big thrombus.
3. Suppuration of the thrombus resulting in
pyaemia and multiple abscesses in the body.
58. 1. Surgical treatment:
It depend on the cause of the complications!!!
• If any complication was caused by acute otitis
the patients needs in simple mastoidotomy
(“Shwart’s or cortical mastoidectomy”).
• If any complication was caused by chronic
otitis (epitympanitis) the patients will be
treated by radical mastoidectomy.
2. Conservative treatment:
• Antibiotics (general & local),
(especially lincosamine group),
• Dehydratation,
• Detoxication,
• Anti-inflammatory remedies…
Management of the otogenic
complications
59. Meniere’s desease
2. Clinical Triad:
1. An attack of severe vertigo without of
unconsciousness.
2. Vegetative disorders till nasea and vomiting.
3. One ear Tinnitus and deafness.
4. Nystagmus is labyrinthine in nature and to the side of the lesion,
whereas in between the attacks it is to the opposite side.
1. Unknown causes due to endolymphatic hydrops.
3. Treatment:
1) absolute rest, sedatives,
2) dehydratation therapy.
3) drainage of the endolymphatical succ.
60. Theories of Meniere’s desease (endolymphatic hydrops)
1. It is due to focal labyrinthitis from a distant septic focus.
2. It is due to vasospasm of the vessels of the stria vascularis which leads
to relative ischaemia which in turn gives rise to increased permeability of
the stria.
3. It is due to allergy of the labyrinth.
4. It is due to salt and water retention in the body.
61. Clinical Triad of Meniere’s desease
1. Suddenly struck with an attack of severe
vertigo. There is no loss of consciousness.
2. There may be vegetative disorders till nasea
and vomiting.
3. There is also tinnitus in the one ear and
appreciable deafness.
4. During the attack the nystagmus is
labyrinthine in nature and to the side of the lesion,
whereas in between the attacks it is to the
opposite side.
If the disease progresses, the intervals become
shorter and shorter and the hearing during the
free periods goes on getting worse and worse.
62. Differential diagnosis of Meniere’s desease
I. Diseases of the external or middle ear:
1. Earwax or foreign body in the external ear which impinges on the drum can push in
ossicular chain and give rise to vertigo.
2. Inflammation of the middle ear cleft may cause sympathetic irritation of the labyrinth
giving rise to vertigo.
3. Even Eustachian block can give rise to this condition.
II. Central or periferal nerves system lesion:
1) eighth nerve tumour,
2) thrombosis of the posterior inferior cerebellar artery,
3) syphilis of the central nervous system,
4) disseminated sclerosis etc.
involving the vestibular nuclei or their connections may give rise to vertigo.
III. Epilepsy: In this disease, there is loss of consciousness which seldom occurs in
Meniere’s disease.
IV. Diseases of the cerebellum may give rise to vertigo but there will be no remissions
as in the case of Menier’s disease.
V. Cardiovascular diseases:
1) hypertension,
2) arteriosclerosis,
3) anaemias or thrombosis of relevant blood vessels in the central nervous system
may also give rise to vertigo.
63. 1. Treatment of Meniere’s desease
The treatment resolves itself into: 1. During the attack and
2. After the attack
which may be: a) medicinal, or b) surgical.
1. During the attack:
1) The patient should be transported to a safe place and put to absolute rest.
2) He should be given sedatives.
3) The dehydratation therapy.
2. After the attack is over:
a) Pharmacotherapy:
I. The patient is prescribed a salt-free diet and minimum intake of fluid. This
does lot of good in nearly half the cases.
II. The patient is given vasodilators (nicotinic acid).
Once the disease is under control, the dose of nicotinic acid should be steadily reduced.
III. Antiallergic drugs are given. (In histamine sensitive patients, desensitisation
with histamine is advocated. Such patients are very few).
IV. Streptomycin is a general depressant to the labyrinth
but its action on the cochlea which is rather uncertain, prohibits its use routinely.
V. Smoking and drinking should be forbidden.
64. 2. Treatment of Meniere’s desease
I. During the attack:
1. Calm dark environment.
2. Sedativs:
- diazepamum 5mg 1(2) t. a day or
- diazepamum 10mg-2ml 1 t. a day or
3. The dehydratation therapy:
a) The patient is prescribed a salt-free diet and
minimum intake of fluid.
b) hypertonic solutions:
- Sol.glucosae 40%-20ml+
+ sol.ac.ascorbinici 5%-2ml i/v 1t. a day
- sol.magnesii hydrochloridi 25%-5ml i/m
c) diuretics:
- lasix 20mg-2ml i/m 1 t. a day in the morning or
- Furasemidum 40mg 1(2) t. a day in the morning
II. After the attack is over:
I.Salt-free diet and minimum intake of fluid.
II. Vasodilators (nicotinic acid 100mg x 3 t. day)
III. Pharmacotherapy like sensoneural deafness.
65. 3. Treatment of Meniere’s desease
2. After the attack:
a) osmotic therapy
by solt
66. 4. Treatment of Meniere’s desease
The treatment resolves itself into:
1. During the attack and
2. After the attack:
a) medicinal, or b) surgical.
b) Surgical treatment:
I. Removal of septic foci,
e.g., infected teeth, tonsils and sinuses.
II. Stellate ganglion block.
III. Cervical sympathectomy.
These two release nervous control over the stria vascularis.
IV. Drainage of the labyrinth - (Labyrinthotomy),
- drainage of the endolymphatical succ
V. Labyrinthectomy (destruction of the labyrinth):
- surgical,
- chemical (injection of alcohol into the labyrinth).
Operations on the labyrinth can be considered if the hearing of the affected
ear is extremely, poor and that of the unaffected ear is reasonable.
67. Meniere’s desease
2. Clinical Triad:
1. An attack of severe vertigo without of
unconsciousness.
2. Vegetative disorders till nasea and vomiting.
3. One ear Tinnitus and deafness.
4. Nystagmus is labyrinthine in nature and to the side of the lesion,
whereas in between the attacks it is to the opposite side.
1. Unknown causes due to endolymphatic hydrops.
3. Treatment:
1) absolute rest, sedatives,
2) dehydratation therapy.
3) drainage of the endolymphatical succ.
68. Otosclerosis
1. Unknown causes.
2. Ankilosis footplate of the stapes.
3. Conductive deafness.
4. Otoscopy of Otosclerosis:
1. Wided external meatus.
2. Skin of external meatus is thinner.
3. Earwax is absent.
4. Sensitivity of the external meatus skin is depressed.
5. The tympanic membrain is thinner.
6. Red spot on the medial wall of tympanic cavity (Schwart’s sign).
4. Piston’s stapedoplasty.
69. Otosclerosis
1. Unknown causes:
- Hereditary factors.
- Hormonal factors (Females after Pregnancy between 20-30 years of
age)
- Endocrine disturbances (Ca metabolism).
2. Ankilosis footplate of the stapes.
Normal bone in the middle layer of the otic capsule.
is absorbed and replaced by spongy osteoid bone,
which becomes thicker and less vascular at one or more constant sites.
This due to Ankilosis footplate of the stapes.
Morphological stage:
1. Vascularisation.
2. Osteospongious.
3. Osteosclerosis.
3. Conductive deafness.
1. Tympanal stage.
2. 2nd mixt stage
3. Sensoneural stage.
4. Otoscopy of Otosclerosis:
1. Wided external meatus.
2. Skin of external meatus is thinner.
3. Earwax is absent.
4. Sensitivity of the external meatus skin is depressed.
5. The tympanic membrain is thinner.
6. Red spot on the medial wall of tympanic cavity (Schwart’s sign).
4. Piston’s stapedoplasty.
70. Predisposing factor of Otosclerosis
Many theories have been advanced but none is satisfactory.
1. Hereditary factors.
White races are more commonly affected than coloured.
Fair complexioned persons are more prone than dark
persons.
There is family history in about 50% of cases.
Hereditary anomalies have all been postulated but not substantiated.
Common associated conditions are
Van der Hoere Syndrome and Paget’s disease.
2. Hormonal factors (endocrine disturbances).
The incidence of disease is much commoner in females
than in males.
Pregnancy may accelerate but never causes the disease.
The disease generally manifests between 20-30 years of age.
3. Different factors
- localized infection,
- malnutrition,
- general toxaemia,
- abnormal labyrinthine circulation.
71. Morphological abnormality of Otosclerosis
Normal bone is absorbed and
replaced by spongy osteoid bone,
which becomes thicker and less vascular
at one or more constant sites.
Morphological stage:
1. Vascularisation.
2. Osteospongious.
3. Osteosclerosis.
This occurs in the middle layer of the otic
capsule.
Silent areas may be present which do not
involve the oval window and do not cause
deafness.
Cochlea may be involved due to spread of
osteoid bone.
Its proximity to foot plate of stapes
causes ankylosis.
72. Clinical features of Otosclerosis
1. Hearing loss is the cardinal symptom.
2. Paracusis Willisii:
Patient generally complains that she can
hear better in presence of back ground
noises. The simplest explanation is that a
normal person raises his voice in pitch and
intensity in noisy surrounding.
Otoscopy of Otosclerosis:
1. Wided external meatus.
2. Skin of external meatus is thinner.
3. Earwax is absent.
4. Sensitivity of the external meatus skin is
depressed.
5. The tympanic membrain is thinner.
6. Red spot on the medial wall of tympanic
cavity (Schwart’s sign).
73. Clinical stage (type) of Otosclerosis
1. Tympanal stage. The deafness is of conductive type.
In early stages there is an upward slope towards the right.
Bone conduction shows a dip at 2000 Hz
(Carhart notch) and is seen in about l/3rd of patients.
2. 2nd mixt stage High tones are only affected, if cochlea is involved. When the cochlea is
invoved then there is downward slope to the right.
2. Mixt stage. 3. Sensoneural stage.
Patient feels handicapped when air conduction
loss exceed 50 dB.
74. Differential Diagnosis of Otosclerosis
1. Healed suppurative otitis media:
- Adhesive (deformity of tympanic membrane);
- Tympanosclerosis (hyalinic cartilages inside
tympanic membrane).
2. Chronic nonsuppurative otitis media
- Eustacheitis (retraction of tympanic membrain).
3. Ossicular disconnection.
4. Perceptive deafness in young adult.
5. Congenital stapes fixation (rare).
Otoscopy of Otosclerosis:
1. Wided external meatus.
2. Skin of external meatus is thinner.
3. Earwax is absent.
4. Sensitivity of the external meatus skin is
depressed.
5. The tympanic membrain is thinner.
6. Red spot on the medial wall of tympanic
cavity (Schwart’s sign).
75. Surgical Treatment of Otosclerosis (stapedectomy)
Surgical Treatment of Otosclerosis (stapedoplasty)
77. Complications surgical treatment of Otosclerosis
1. Perforation of tympanic membrane.
2. Vertigo.
3. Otitis Media.
4. Damage to facial nerve.
5. Taste disturbance.
6. Damage to membranous labyrinth.
7. Leakage of perilymph.
8. Dislocation of incus.
9. Bleeding.
10. Loss of part or whole of foot-plate
into the vesitbule.
Late complications:
1. Dislocation of prosthesis.
2. Meningitis.
3. Completely deaf ear.
4. Reparative granuloma.
78. Otosclerosis
1. Unknown causes.
2. Ankilosis footplate of the stapes.
3. Conductive deafness.
4. Otoscopy of Otosclerosis:
1. Wided external meatus.
2. Skin of external meatus is thinner.
3. Earwax is absent.
4. Sensitivity of the external meatus skin is depressed.
5. The tympanic membrain is thinner.
6. Red spot on the medial wall of tympanic cavity (Schwart’s sign).
4. Piston’s stapedoplasty.
79. Sensoneural deafness
2. Sensoneural desorders by Tonal audiometry .
х - bone conduction, о - air conduction.
AD (Auris Dexter)
RE (Right ear)
AS (Auris Sinister)
LE (Left ear)
- Tinnitus ++
>5m WV >1m
>20m CV >3m
20'' Tf (Tunning fork) 128 bone (N=20'') 10"
40'' Tf (Tunning fork) 128 air (N=40'') 20''
30'' Tf (Tunning fork) 2048 (N=30'') 150''
+ Rinne +"small"
Weber
Not longthened Schwabah shortened
Not shortened
3. Left ear Sensoneural deafness.
1. Normal otoscopic picture.
Sign:
1. Hearing loss.
2. Tinnitus.
3. Normal otoscopic picture.
4. Sensoneural deafness.
80. 1. Causes of deafness
Deafness may be classified in two ways:
I. a) Congenital, b) Acquired.
II. a) Conductive, b) Perceptive (sensotineural)
с) Mixed - conductive and perceptive.
It is two types of perceptive deafness:
1. Cochlear (sensory part)
2. Retro-cochlear or neural.
I. In the inner ear.
II. In the eighth nerve.
III. In the central nervous system.
81. 2. Causes of deafness
Pharmacologic toxicity
ototoxic drugs: eg - salicylates, quinine,
- aminoglycoside antibiotics (drugs like streptomycin and
quinine may affect the auditory nerve),
- loop diuretics (furosemide, ethacrynic acid,
- cancer chemotherapeutic agents (eg. cisplatin).
Infectious - Otitis media, viral, syphilis, meningitis,
Traumas: - transversal fractures pyramid of the temporal bone,
- noise-induced
Neurologic disorders: - vascular, demyelinating (eg. multiple sclerosis),
- infectious, or
degenerative disease affecting the central auditory pathways,
- cerebellopontine angle tumors
such as vestibular schwannomas (acoustic neuromas) or
meningiomas;
Vascular and
hematologic disorders: - Migraine, cryoglobinemia
Immune disorders: - Polyarteritis nodosa, HIV.
Bone disorders: - Paget disease
Inner ear deseases: - Meniere disease,
- Cochlear otosclerosis,
- Presbycusis (Age-Related Hearing Loss),
82. 3. Causes of deafness
Infant Infectious: - The infectious fevers in infancy
(meningitis, typhoid fever, measles,
mumps, whopping cough)
Congenital Hearing Loss: - HIV-Related Hearing Loss
(Human immunodeficiency virus (HIV) infection leads to both
peripheral and central auditory system pathology.
Genetic Causes: - hereditary hearing impairment (HHI) can manifest later in life.
HHI may be classified as either:
nonsyndromic hearing loss, in which deafness is the only clinical abnormality or
syndromic hearing loss, in which deafness is associated with anomalies in other organ
systems.
Syndromic (More than 200 syndromes are associated with hearing loss):
1. Usher syndrome (retinitis pigmentosa and hearing loss),
2. Waardenburg syndrome (pigmentary abnormality and hearing loss),
3. Pendred syndrome (thyroid organification defect and hearing loss),
4. Alport syndrome (renal disease and hearing loss), and
5. Jervell & Lange-Nielsen syndromes (prolonged QT interval and hearing loss).
Nonsyndromic: - Large vestibular aqueduct syndrome
83. 4. Causes of deafness
I. In the inner ear:
1. Meniere’s disease.
2. Senile deafness due to arteriosclerosis of the vessels supplying the internal ear.
3. Trauma. This maybe from noises, fractures of the temporal bone, or concussion of the internal ear or
4. Toxins. Drugs like streptomycin and quinine may affect the auditory nerve.
Exogenous toxins like too much alcohol or endogenous toxins like those found in diabetes and septic
foci are also likely causes.
5. General malnutrition and vitamin deficiency.
II. In the eighth nerve: Eighth nerve tumour.
III. In the central nervous system:
1. Tumours, vascular accidents, disseminated sclerosis, syphilis and mental
deficiency etc.
2. Cortical lesions do not give rise to perceptive deafness unless both centres on the right and left are
simultaneously affected because the nuclei in the brain stem send fibres to both cortical centres.
Psychogenic deafness:
It is that type of deafness in which there is no organic cause to explain it.
1. Hysterical or functional:
In this case, the patient in reality cannot hear external sounds due to something in his subconscious
mind.
2. Malingering, also cacalled feignet or simirfated deafness.
In this case, the patient can, in reality, hear external sounds, but on account of some reason of personal
gain, he pretends that he cannot hear.
84. Sign of Sensoneural deafness
Normal tonal audiometry.
х - bone conduction, о - air conduction.
2. Sensoneural desorders by Tonal audiometry .
х - bone conduction, о - air conduction.
AD (Auris Dexter)
RE (Right ear)
AS (Auris Sinister)
LE (Left ear)
- Tinnitus ++
>5m WV >1m
>20m CV >3m
20'' Tf (Tunning fork) 128 bone (N=20'') 10"
40'' Tf (Tunning fork) 128 air (N=40'') 20''
30'' Tf (Tunning fork) 2048 (N=30'') 150''
+ Rinne +"small"
Weber
Not longthened Schwabah shortened
Not shortened
3. Left ear Sensoneural deafness.
1. Normal otoscopic picture.
85. 1. Treatment of Sensoneural deafness
I. Its depend on causes:
1. Creating a Favorable Environment for Hearing.
2. Toxic – antidot or detoxication:
- Streptomycinum - Vit B15;
- spiritus methylicus - spiritus aethylicis.
3. Local vasospasmus - central vasodilatators:
- vinpocetinum (cavinton) 0.01-2ml i/v x 1t. a day or
0.01 1t. x 3 t. a day
4. Hypertension - peripheral vasodilatators:
5. Symptomatic hypertension:
- renal - surgery;
- endocrine - hormonal therapy…
6. Thrombosis:
- Sol. Heparini natrici 5000 “ME”/ml – 1(2)ml i/v x 1(3) t. a day +
next days s/c(abdomen) 5000 x 2 t. a day
7. Haemorrage:
- tab. Ethamsilatum 0.25 x 3 t. a day;
- sol. Ethamsilatum 12.5%-2ml I/v or I/m 2(3) t. a day
86. 2. Treatment of Sensoneural deafness
II. Nonspecific Pharmacotherapy:
I. Nootropic:
- pyracetamum 20%-5ml i/v 1t. a day or
- pyracetamum 0.2 x 3t. a day
II. Central vasodilators:
- vinpocetinum (cavinton) 0.01-2ml i/v x 1t. a day or
0.01 1t. x 3 t. a day
III. Blood desagregation:
- pentoxifyllinum (trental) 0.2 x 3 t. a day x 10 days and
next 0.1 x 3 t. a day x 10 days
IV. For stimulating transmission nerves impulses in synapses:
Anticholinestheratic:
- proserinum 0.05%-1ml i/m x 1t. a day
- Ipidacrinum (neiromidinum) 0.020 x 2 t. a day x10-30 days
0.5%-1ml s/c or I/m x 1 t. a day
V. Nerves system energy riser:
- Acidum gammaaminobutyricum (aminalon) 0.25 x 3 t. a day
- ATP-long 2%-2ml i/v 1 t. a day
VI. Nonspecific stimulators:
- corpus vitreum 1ml i/m x 1t. a day
VII. Vitamins B1 , B2 , B6 , B12: (Neurovitan, Neiron, Neurorubine)
88. 1. Prevention of Sensoneural deafness
1. Vaccination
The vaccination of infants against Haemophilus influenzae type
B meningitis prevents a major cause of acquired deafness, as have
immunizations for measles, mumps, and rubella.
A vaccine against Streptococcus pneumoniae, the most
common organism associated with otitis media, is also available and is
having a positive impact on the reduction in the incidence of ear
infections.
In addition, careful monitoring of serum peak-and-trough levels
can largely prevent the loss of vestibular function and deafness due to
aminoglycoside antibiotics.
89. 2. Prevention of Sensoneural deafness
2. Noise Avoidance
Ten million Americans have noise-induced hearing loss and 20
million are exposed to hazardous noise in their employment.
Noise-induced hearing loss can be prevented by avoiding exposure
to loud noise or by the regular use of earplugs or fluid-filled muffs to
attenuate intense sound.
3. High-Risk Activities
High-risk activities for noise-induced hearing loss include wood-
and metalworking with electrical equipment as well as target
practice and hunting with small firearms. All internal-combustion and
electric engines, including snowblowers and leaf blowers,
snowmobiles, outboard motors, and chain saws, require that the
user wear hearing protectors.
4. Education
Almost all noise-induced hearing loss is preventable through
education, which should begin before adolescence.
Industrial programs of hearing conservation are required when the
exposure over an 8-hour period averages 85 dB on the A scale.
Workers in such noisy environments can be protected with
preemployment audiologic assessment, the mandatory use of hearing
protectors, and annual audiologic assessments.
90. Sensoneural deafness
1. Patients with mild, moderate, and severe sensorineural hearing
losses are rehabilitated regularly with hearing aids that vary in
configuration and strength.
They also have been miniaturized; the current generation of
hearing aids can be placed entirely within the ear canal, thus
reducing the stigma associated with their use.
Digital hearing aids lend themselves to programming for the
individual;
(2) But, multiple and directional microphones at the ear level help
some individuals with the difficulty of using a hearing aid in noisy
surroundings. Since all hearing aids amplify noise as well as speech,
the only absolute solution to the problem is to place the microphone
closer to the speaker than to the noise source.
This arrangement is not possible with a self-contained, cosmetically
acceptable device; it is cumbersome and requires a user-friendly
environment.
2. In many situations, including at lectures and at the theater,
hearing-impaired persons benefit from assistive devices that are
based on the principle of having the speaker closer to the microphone
than to any source of noise.
Assistive devices include infrared and FM transmission; they also
include an electromagnetic loop placed around the room for
transmission to the individual’s hearing aid.
Hearing aids with telecoils also can be used with properly
equipped telephones in the same way.
Amplification
91. Sensoneural deafness
In the event that a hearing aid provides inadequate
rehabilitation, cochlear implants are appropriate.
The criteria for implantation are undergoing constant revisions.
Children with congenital and acquired profound hearing impairment
are also appropriate candidates for cochlear implantation; many are
being implanted as early as 6 to 9 months.
In most cases of profound hearing impairment, the auditory hair
cells are lost, but the spiral ganglion cells of the auditory division
of the eighth nerve are preserved.
Cochlear implants are a specialized hearing prosthesis for the
rehabilitation of profound deafness that convert mechanical sound
energy into electrical signals that are delivered to the neurons of
the cochlear nerve.
The basic operation of the implant is as follows:
A microphone is used to pick up acoustic information that is sent
to an external speech processor (located on the body or at ear level).
This processor converts the mechanical acoustic wave into an
electric signal that is transmitted via the surgically implanted
electrode array in the cochlea to the auditory nerve.
Bilateral cochlear implants hold the promise of enhanced sound
localization and improvement in understanding speech in the presence
of background noise.
1. Cochlear Implants
92. Sensoneural deafness
Cochlear Implants consist of:
1. A microphone, which picks up
acoustic information and converts it to
electrical signals;
2. An externally worn speech
processor that processes the signal
according to a predefined strategy;
3. A surgically implanted electrode
array that is in the cochlea near the
auditory nerve.
2. Cochlear Implants
Incision and implant site for
cochlear implantation.
93. Sensoneural deafness
3. Cochlear Implants
Location of induction coil.
Trough and groove drilled for electrode implantation into mastoid.
94. Sensoneural deafness
4. Cochlear Implants
The facial recess is bounded by the fossa incudis superiorly,
the chorda tympani nerve laterally and anteriorly,
and the facial nerve medially and posteriorly.
A cochleostomy is created anterior and inferior to the round window.
98. Sensoneural deafness
For individuals who have had both eighth nerves destroyed by
trauma or bilateral vestibular schwannomas (eg, patients with
neurofibromatosis II), a brainstem auditory implant placed near the
cochlear nucleus may provide auditory rehabilitation.
With additional advances in brainstem auditory implant technology,
patients may eventually obtain benefits similar to individuals who have
cochlear implants.
Brainstem Auditory Implant
99. Sensoneural deafness
2. Sensoneural desorders by Tonal audiometry .
х - bone conduction, о - air conduction.
AD (Auris Dexter)
RE (Right ear)
AS (Auris Sinister)
LE (Left ear)
- Tinnitus ++
>5m WV >1m
>20m CV >3m
20'' Tf (Tunning fork) 128 bone (N=20'') 10"
40'' Tf (Tunning fork) 128 air (N=40'') 20''
30'' Tf (Tunning fork) 2048 (N=30'') 150''
+ Rinne +"small"
Weber
Not longthened Schwabah shortened
Not shortened
3. Left ear Sensoneural deafness.
1. Normal otoscopic picture.
Sign:
1. Hearing loss.
2. Tinnitus.
3. Normal otoscopic picture.
4. Sensoneural deafness.
100. Classifacation of the
mastoiditis & paramastoiditis
• Acute,
• Subacute,
• Chronic,
• Latent.
Mastoiditis (Tipical):
• Tip form (2),
• Subperiostal abscess (4),
• Subperiostal abscess (4),
• Perisinuosus abscess (3),
Paramastoiditis:
• Zygomaticitis,
• Occipititis,
• Squamitis,
• Petrositis,
• Apicitis etc.
101. Гострий мастоїдит (Acute mastoiditis)
1. Симптоми отиту (Symptoms of otitis):
- вушний біль (otalgia), - виділення (discharge),
- зниження слуху (hearing loss), - шум у вухах (tinnitus).
2. Інфекційно-інтоксикаційний синдром
(signs of Infectious intoxication):
- weakness, mussles pain, perspiration,
- hypertermia, - leucocytosis…
3. Симптоми мастоідиту (mastoiditis sign):
- профузна оторрея (profuse otorrhea - “Cystern” sign);
- пастозність м’яких тканин соскоподібного відростка
(thickness soft tissue in mastoid region),
(thickness soft tissue in mastoid region),
- болючість соскоподібного відростка (painful mastoid),
- потовщення задньо-верхньої стінки кісткової
частини зовнішнього слухового проходу (thickness of
posterior-superior wall of the bony part of external meatus).
- Ro, CT затемнення комірок (X-rays, CT - cells shadow).
4. Особливі місцеві симптоми при парамастоїдитах
(Specific Local sign depend on the localisation):
верхівково-шийні форми, перисинуозний абсцес,
зигомацитит, петрозит, апіцит…
tip form, perisinuosus abscess, zigomaticitis, petrositis,
apicitis etc.
102. 1. Тактика лікування мастоїдітів залежить від характера причинного отиту.
(management of the mastoiditis depend on the cause of the mastoiditis).
• Якщо мастоідит викликаний гострим отитом (гнійним середнім) то виконується
проста (кортикальна) антромастоідеотомія,
If mastoiditis was caused by acute otitis indicated cortical antromastoidotomy (simple or
“Shwart’s antromastoidectomy”).
• Якщо мастоідит викликаний хронічним отитом (епітимпанітом) то виконується
загальнопорожнинна (радикальна) операція на вусі (атикоантромастоідеотомія)
If mastoiditis was caused by chronic otitis (epitympanitis) indicated radical
Management of the mastoiditis
If mastoiditis was caused by chronic otitis (epitympanitis) indicated radical
atticoantromastoidectomy.
2. Медикаментозне лікування (Conservative treatment):
• Антибактериальне (Antibiotics (general & local - lincosamine group).
• НПЗЗ (Antiinflammatory nonsteroid remedies).
• Дезінтоксикація (Detoxication).
• Дегідратація (Dehydratation).
• Назальні деконгестанти (nasal decongestants).
105. Simple or cortical AntroMastoidotomy
(Source: Hughes GB, Pensak MP. Clinical Otology. New York: Thieme;
1997)
106. 1. Симптоми отиту (Symptoms of otitis):
- pain, - discharge,
- deafness, - tinnitus.
2. Інфекційно-інтоксикаційний синдром
(signs of Infectious intoxication):
- weakness, mussles pain, perspiration,
- hypertermia,
- leucocytosis…
3. Симптоми внутрішньочерепної гіпертензії
Групи симптомів отогенного менінгіту
Groups of symptoms of the otogenic meningitis
3. Симптоми внутрішньочерепної гіпертензії
(Sign of the intracranial hypertension):
- bradycardia,
- papilloedema,
- diffuse strong headache
wich cann’t be controled by analgetics with
- nasea, vomiting,
4. Менінгеальні симтоми (Meningeal sign):
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of medicine.- 2006.
107. 1. Симптоми отиту (Symptoms of otitis):
- pain, - discharge,
- deafness, - tinnitus.
2. Інфекційно-інтоксикаційний синдром
(signs of Infectious intoxication):
- weakness, mussles pain, perspiration,
- hypertermia,
- leucocytosis…
3. Симптоми внутрішньочерепної гіпертензії
Групи симптомів отогенного менінгіту
Groups of symptoms of the otogenic meningitis
3. Симптоми внутрішньочерепної гіпертензії
(Sign of the intracranial hypertension):
- bradycardia,
- papilloedema,
- diffuse strong headache
wich cann’t be controled by analgetics with
- nasea, vomiting,
4. Менінгеальні симтоми (Meningeal sign):
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of medicine.- 2006.
108. 1. Симптоми отиту (Symptoms of otitis):
- pain, - discharge,
- deafness, - tinnitus.
2.Інфекційно-інтоксикаційний синдром
(signs of Infectious intoxication):
- weakness, mussles pain, perspiration,
- hypertermia,
- leucocytosis…
3.Симптоми внутрішньочерепної гіпертензії
(Sign of the intracranial hypertension):
- bradycardia,
- papilloedema,
- diffuse strong headache
wich cann’t be controled by analgetics with
- nasea, vomiting,
Групи симптомів отогенного абсцесу скроневої долі мозку
Groups of symptoms of the otogenic temporal lobe brain abscess
- nasea, vomiting,
4. Менінгеальні симтоми (Meningeal sign):
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
5. Local sign of brain lession:
- amnestic, motor or sensorial aphasia
(in case with left side temporal lobe brain leasion
if patient is right-handed,
- contralateral paresis,
- dilated pupils, ptosis and lateral rectus paralysis,
homonymous hemianopia
109. 1. Симптоми отиту (Symptoms of otitis):
- pain, - discharge,
- deafness, - tinnitus.
2. Інфекційно-інтоксикаційний синдром
(signs of Infectious intoxication):
- weakness, mussles pain, perspiration,
- hypertermia,
- leucocytosis…
3.Симптоми внутрішньочерепної гіпертензії
(Sign of the intracranial hypertension):
- bradycardia,
- papilloedema,
- diffuse strong headache
wich cann’t be controled by analgetics with
- nasea, vomiting,
4.
Групи симптомів отогенного абсцесу мозочка
Groups of symptoms of the otogenic cerebellar abscess
4.Менінгеальні симтоми (Meningeal sign):
- rigidity of the necks muscles,
- Kernig’s sign,
- Brudsinsky’s sign…
5. Local sign on cerebellar lesion side:
1. Falling down in static tests (Romberg test).
2. Deviation in Kynetic tests (step test).
3. Deviation in coordinative tests (finger-nose test).
4. Ipsilateral asynergia (dysdia-dochokinesis).
5. Muscles hypotonia (flaccidity).
6. Nystagmus (continuous, big amplitude,
any directions till diagonal…)
110. 1. Симптоми отиту (Symptoms of otitis):
- pain, - discharge,
- deafness, - tinnitus.
2. Інфекційно-інтоксикаційний синдром
- swinging temperature with rigors at irregular intervals,
- pyaemic abscesses chiefly in lungs & joints,
- positive blood cultyre,
- enlarged spleen and marked leucocytosis)
+ як паразитогенна інтоксикація при малярії
(signs of infectious intoxication like parasitogenic due to malaria):
+ Тріада: апериодична гіпертермія з потрясаючим ознобом і проливним потом
(triad: - aperiodic chills (shivering) & fever and sweating (perspiring).
+ плазмодій малярії у мазках крові, “+” імунохімічний тест
Групи симптомів отогенного тромбозу сигмоподібного синуса
Groups of symptoms of the otogenic Sigmoid (lateral) sinus thrombosis
+ плазмодій малярії у мазках крові, “+” імунохімічний тест
(plasmodium malaria in blood, “+” immunochemical test).
+ And effectiveness of specific treatment (chinin+ clindamycin, artemizin, chlorchin)
+ Anemia, hyperbilirubinemia, ALT, AST, hypoalbuminemia
3. Симптоми мастоідиту (mastoiditis sign):
- профузна оторрея (profuse otorrhea - “Cystern” sign);
- пастозність м’яких тканин соскоподібного відростка (thickness soft tissue in mastoid region),
- болючість соскоподібного відростка (painful mastoid),
- потовщення задньо-верхньої стінки кісткової частини зовнішнього слухового проходу
(thickness of posterior-superior wall of the bony part of external meatus).
- Ro, CT затемнення комірок (X-rays, CT - cells shadow).
4. Obstructive symptoms
4.1. Tobey-Ayer or Queckenstedt’s test – liquor hypertension via lumbar puncture + digital pressure
on the internal jugular vein on the healthy side).
4.2. Greisinger’s sign - oedema of mastoid (if the mastoid emissary vein gets involved).
111. 1.Симптоми отиту (Symptoms of otitis):
- pain, - discharge,
- deafness, - tinnitus.
2. Інфекційно-інтоксикаційний синдром
(signs of Infectious intoxication):
- weakness, mussles pain, perspiration,
- hypertermia,
- leucocytosis…
3.Симптоми мастоідиту (mastoiditis sign):
- профузна оторрея (profuse otorrhea - “Cystern” sign);
- пастозність м’яких тканин соскоподібного відростка (thickness soft tissue in mastoid region),
- болючість соскоподібного відростка (painful mastoid),
-потовщення задньо-верхньої стінки кісткової частини зовнішнього слухового проходу
(thickness of posterior-superior wall of the bony part of external meatus).
-Ro, CT затемнення комірок (X-rays, CT - cells shadow).
Gtroups of symptoms of the otogenic extradural abscess
(thickness of posterior-superior wall of the bony part of external meatus).
-Ro, CT затемнення комірок (X-rays, CT - cells shadow).
4. Місцеві ознаки (local sign):
поєднання (combination of)
- симптома «резервуара» (cistern sign)
накопичення гнійного вмісту з (accumulation of purulent discharge with)
- з пульсацією гнійних виділень (pus pulsation)
(double sign).
5.CT, MRI – накопичення рідини гнійної щільності
між кісткою черепа і твердою мозковою оболонкою
(accumulation of purulent discharge between skull bone & dura mater).
112. 1. Тактика хірургічного лікування залежить від характера
причинного отиту.
Management depend on the cause of the complications.
• Якщо внутрішньочерепне ускладнення викликане гострим
отитом (гнійним середнім) то виконується кортикальна
(проста) розширена антромастоідеотомія
(If any intracranial complication was caused by acute middle
purulent otitis indicated extended cortical mastoidotomy (simple
or “Shwart’s mastoidectomy”).
• Якщо внутрішньочерепне ускладнення викликанe хронічним
отитом (епітимпанітом) то показана загальнопорожнинна
Management of the otogenic complications
(Source: Hughes GB, Pensak MP. Clinical
Otology. New York: Thieme; 1997.)
отитом (епітимпанітом) то показана загальнопорожнинна
(радикальна) розширена операція на вусі
(атикоантромастоідеотомія)
If any intracranial complication was caused by chronic otitis
(epitympanitis) indicated radical atticoantromastoideotomy.
2. Медикаментозне лікування (Conservative treatment):
• Антибактериальне (Antibiotics (general & local - lincosamine
group),
• НПЗЗ (Antiinflammatory remedies),
• Дезінтоксикація (Detoxication),
• Дегідратація (Dehydratation),
• Назальні деконгестанти (nasal decongestants).
113. Source: Menner Albert L. A Pocket Guide to the Ear / Thieme.- Stuttgart · New York.- 2003.- 145 p.
Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
Source: Hughes GB, Pensak MP. Clinical Otology. New York: Thieme; 1997.)
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of
medicine.- 2006.
Ballenger’s Otorhinolaryngology. Head and Neck Surgery / James B. Snow Jr,, John Jacob Ballenger // Sixteenth Edition.- BC Decker Inc.-
2006.- 1616 p.
114. Хвороба Меньєра
Meniere’s desease
2. Clinical Triad:
1. An attack of severe vertigo without of
1. Ендолімфатичний гідропс внаслідок мультифакториальних причин
(Endolymphatic hydrops due to multifactorial causes).
1 An attack of severe vertigo without of
unconsciousness.
2. Vegetative disorders till nasea and vomiting.
3. One ear Tinnitus and deafness.
4. Nystagmus is labyrinthine in nature and to the side of the lesion,
whereas in between the attacks it is to the opposite side.
3. Treatment:
1) absolute rest, sedatives,
2) dehydratation therapy.
3) drainage of the endolymphatical succ.
115. 2. Treatment of Meniere’s desease
I. During the attack:
1. Calm dark environment.
2. Sedativs:
- diazepamum 5mg 1(2) t. a day or
- diazepamum 10mg-2ml 1 t. a day or
3. The dehydratation therapy:
a) The patient is prescribed a salt-free diet and
minimum intake of fluid.
b) hypertonic solutions:
b) hypertonic solutions:
- Sol.glucosae 40%-20ml+
+ sol.ac.ascorbinici 5%-2ml i/v 1t. a day
- sol.magnesii hydrochloridi 25%-5ml i/m
c) diuretics:
- lasix 20mg-2ml i/m 1 t. a day in the morning or
- Furasemidum 40mg 1(2) t. a day in the morning
II. After the attack is over:
I.Salt-free diet and minimum intake of fluid.
II. Vasodilators (nicotinic acid 100mg x 3 t. day)
III. Pharmacotherapy like sensoneural deafness.
116. Otosclerosis
1. Unknown causes.
2. Ankilosis footplate of the stapes.
3. Conductive deafness.
4. Otoscopy of Otosclerosis:
4. Otoscopy of Otosclerosis:
1. Wided external meatus.
2. Skin of external meatus is thinner.
3. Earwax is absent.
4. Sensitivity of the external meatus skin is depressed.
5. The tympanic membrain is thinner.
6. Red spot on the medial wall of tympanic cavity (Schwart’s sign).
4. Piston’s stapedoplasty.
117. Clinical stage (type) of Otosclerosis
1. Tympanal stage. The deafness is of conductive type.
In early stages there is an upward slope towards the right.
Bone conduction shows a dip at 2000 Hz
(Carhart notch) and is seen in about l/3rd of patients.
Patient feels handicapped when air conduction
loss exceed 50 dB.
2. 2nd mixt stage High tones are only affected, if cochlea is involved. When the cochlea is
invoved then there is downward slope to the right.
2. Mixt stage. 3. Sensoneural stage.
119. Sensoneural deafness
2. Sensoneural desorders by Tonal audiometry .
х - bone conduction, о - air conduction.
(Source: Sanna M, Russo A, DeDonato G. Color Atlas of
Otoscopy. Stuttgart: Thieme; 1999)
AD (Auris Dexter)
RE (Right ear)
AS (Auris Sinister)
LE (Left ear)
- Tinnitus ++
>5m WV >1m
>20m CV >3m
20'' Tf (Tunning fork) 128 bone (N=20'') 10"
40'' Tf (Tunning fork) 128 air (N=40'') 20''
30'' Tf (Tunning fork) 2048 (N=30'') 150''
+ Rinne +"small"
Weber
Not longthened Schwabah shortened
Not shortened
3. Left ear Sensoneural deafness.
1. Normal otoscopic picture.
Sign:
1. Hearing loss.
2. Tinnitus.
3. Normal otoscopic picture.
4. Sensoneural deafness.
Otoscopy. Stuttgart: Thieme; 1999)
120. 1. Treatment of Sensoneural deafness
I. Its depend on causes:
1. Creating a Favorable Environment for Hearing.
2. Toxic – antidot or detoxication:
- Streptomycinum - Vit B15;
- spiritus methylicus - spiritus aethylicis.
3. Local vasospasmus - central vasodilatators:
- vinpocetinum (cavinton) 0.01-2ml i/v x 1t. a day or
0.01 1t. x 3 t. a day
4. Hypertension - peripheral vasodilatators:
4. Hypertension - peripheral vasodilatators:
5. Symptomatic hypertension:
- renal - surgery;
- endocrine - hormonal therapy…
6. Thrombosis:
- Sol. Heparini natrici 5000 “ME”/ml – 1(2)ml i/v x 1(3) t. a day +
next days s/c(abdomen) 5000 x 2 t. a day
7. Haemorrage:
- tab. Ethamsilatum 0.25 x 3 t. a day;
- sol. Ethamsilatum 12.5%-2ml I/v or I/m 2(3) t. a day
121. 2. Treatment of Sensoneural deafness
II. Nonspecific Pharmacotherapy:
I. Nootropic:
- pyracetamum 20%-5ml i/v 1t. a day or
- pyracetamum 0.2 x 3t. a day
II. Central vasodilators:
- vinpocetinum (cavinton) 0.01-2ml i/v x 1t. a day or
0.01 1t. x 3 t. a day
III. Blood desagregation:
- pentoxifyllinum (trental) 0.2 x 3 t. a day x 10 days and
next 0.1 x 3 t. a day x 10 days
next 0.1 x 3 t. a day x 10 days
IV. For stimulating transmission nerves impulses in synapses:
Anticholinestheratic:
- proserinum 0.05%-1ml i/m x 1t. a day
- Ipidacrinum (neiromidinum) 0.020 x 2 t. a day x10-30 days
0.5%-1ml s/c or I/m x 1 t. a day
V. Nerves system energy riser:
- Acidum gammaaminobutyricum (aminalon) 0.25 x 3 t. a day
- ATP-long 2%-2ml i/v 1 t. a day
VI. Nonspecific stimulators:
- corpus vitreum 1ml i/m x 1t. a day
VII. Vitamins B1 , B2 , B6 , B12: (Neurovitan, Neiron, Neurorubine)
122. 2. Treatment of Sensoneural deafness
II. Nonspecific Pharmacotherapy:
I. Nootropic:
- pyracetamum 20%-5ml i/v 1t. a day or
- pyracetamum 0.2 x 3t. a day
II. Central vasodilators:
- vinpocetinum (cavinton) 0.01-2ml i/v x 1t. a day or
0.01 1t. x 3 t. a day
III. Blood desagregation:
- pentoxifyllinum (trental) 0.2 x 3 t. a day x 10 days and
next 0.1 x 3 t. a day x 10 days
next 0.1 x 3 t. a day x 10 days
IV. For stimulating transmission nerves impulses in synapses:
Anticholinestheratic:
- proserinum 0.05%-1ml i/m x 1t. a day
- Ipidacrinum (neiromidinum) 0.020 x 2 t. a day x10-30 days
0.5%-1ml s/c or I/m x 1 t. a day
V. Nerves system energy riser:
- Acidum gammaaminobutyricum (aminalon) 0.25 x 3 t. a day
- ATP-long 2%-2ml i/v 1 t. a day
VI. Nonspecific stimulators:
- corpus vitreum 1ml i/m x 1t. a day
VII. Vitamins B1 , B2 , B6 , B12: (Neurovitan, Neiron, Neurorubine)
124. Sensoneural deafness
2. Cochlear Implants
Cochlear Implants consist of:
1. A microphone, which picks up
acoustic information and converts it to
electrical signals;
2. An externally worn speech
processor that processes the signal
according to a predefined strategy;
3. A surgically implanted electrode
array that is in the cochlea near the
auditory nerve.
Incision and implant site for
cochlear implantation.
Ballenger’s Otorhinolaryngology. Head and Neck Surgery / James B. Snow Jr,, John Jacob Ballenger // Sixteenth Edition.- BC Decker Inc.- 2006.- 1616 p.
125. Sensoneural deafness
6. Cochlear Implants
Electrode in scala tympani (cross section of basal turn on cochlea).
Ballenger’s Otorhinolaryngology. Head and Neck Surgery / James B. Snow Jr,, John Jacob Ballenger // Sixteenth Edition.- BC Decker Inc.- 2006.- 1616 p.
126. Source: Menner Albert L. A Pocket Guide to the Ear / Thieme.- Stuttgart · New York.- 2003.- 145 p.
Source: Sanna M, Russo A, DeDonato G. Color Atlas of Otoscopy. Stuttgart: Thieme; 1999)
Source: Hughes GB, Pensak MP. Clinical Otology. New York: Thieme; 1997.)
Source: El-Guindy A.The ear slide show.- The department of Otolaryngology - Head and Neck surgery university of Tanta, school of
medicine.- 2006.
Ballenger’s Otorhinolaryngology. Head and Neck Surgery / James B. Snow Jr,, John Jacob Ballenger // Sixteenth Edition.- BC Decker Inc.-
2006.- 1616 p.
148. General condition
Temperature
Hyperemia of the
mucous membrane
not suffered
SUBfebril
posterior wall of the
pharynx
Differential diagnosis
Acute kataral tonsillitis & Acute pharyngitis
suffered
febril
tonsills
149. 4
1. Diet.
2. Pharyngeal washing & resorption of oroantiseptics
(pharyngosept, septefrylum, strepsils etc.).
If the general condition suffered (in childhood):
3. Antibiotics (аmoxicillini 0,5х3 t. a day х7 days).
4. Nonsteroid anti-inflammatory drugs (amizoni 0,25х1t.a day х10 days).
5. Desensitation (desloratadinum 0,01х1t.a day х10 days).
6. Compress with 40-50% alcohol on neck.
Treatment of the acute pharyngitis
150. Chronic katarrhal pharyngitis
1. Light diet, voluminous water drinking.
2. Oroantiseptics (chlorhexidini hydrochloridi 0.005 х6 t. a
day х5 days resorption intrapharyngeal).
3. Local nonsteriod anti-inflammatory remedies
(biclothymoli 4(6) t. a day х10 days).
Chronic heperplastic pharyngitis
+ electrocoagulation, chemical cautery, cryodistruction,
surgical remuving of lymphoid hyperplastic focus
(folliculs)
Chronic atrophic pharyngitis
+ washing mucous membrane (gargling) ,
+ stimulation of mucous glands by Lugol’s solution,
+ biogenic stimulators (aloes, placentae).
Chronic pharyngitis
157. 1
1. The desease is taking its like severe Infectious
disease,
+ convulsion with hypertermia,
+ pseudo opisthotonus.
2. With dispepsia, nausea, vomit(ing) (retching), ,
meteorism (tympanism); wieght doesn’n taking
normal.
3. Respiratory insufficiency (restriction of lungs
excursion).
4. More often laryngitis, bronchitis, pneumonia.
5. More frequently otitis.
6. Soft palate paresis possible.
7. Maceration angle mouth skin.
Peculiarity of acute tonsillitis in childhood
158. 1
Patient can be isolated at home or infectious department.
1. Bed regime (stay in bed) for complications prevention.
2. Light diet, voluminous water drinking.
3. Antibacterial (amoxicillini 0,5х3 t. a day х7 days).
4. Oroantiseptics (chlorhexidini hydrochloridi 0.005 х6 t. a day х5 days
resorption intrapharyngeal).
5. Local nonsteriod anti-inflammatory remedies (biclothymoli 4(6) t. a day х10
days).
6. Nonsteriod anti-inflammatory remedies (aspirini 0,5х3 t. a day х10 days).
7. Desensitation (loratadini 0,01х1 t. a day х10 days).
8. Neck compresses (40-50% alkohol or 25% dimethylsulfoxidi with antibiotic
х5-7 days).
Treatment of acute tonsillitis
159. 1
1. Severe general condition, intoxication…
3. Localy: errosion, cyanosis, edema more than hyperemia,
or dull greyish membrane formation is present on the
tonsil and extends beyond e.g., on to the pillars, palate
or uvula. It is not easily detachable with bleeding mucous membrane.
but till the 2st day it is whitish easily detachable.
or hemorrhage.
Diphtheria of pharyngis
4. Face, neck edema.
5. Regional lymphadenitis.
6. Toxic lesion of the peripheral nerves –
polineuritis (soft palate, vocal cord paresis..)
7. Toxic lesion of the heart muscle.
8. Toxic lesion of the kidneys.
Obligated investigation
Swab for BL-investigation !!!
160. 1
Form of Diphtheria
1. Katarrhal (edema, cyanosis more than hyperemia).
2. Membraneous: - local,
- diffuse
(dull greyish membrane formation on the tonsills and extends
beyond e.g., on to the pillars, palate, uvula. It is not easily detachable
with mucous membrane bleeding.
3. Toxic:
- SubToxic (I stage) – edema till half of neck.
- Toxic (II stage) – edema till clavicle.
- HyperToxic ( III stage) – below clavicle.
4. Hemorrhagic (+ Hemorrhage).
161. 1
Obligated investigation:
- Swab for bacteriological examination
(Leffler’s bacillus ) !!!
Treatment:
1. The specific drag is antidiphtheria serum.
If the diagnosis is not dear, 10,000-100,000 units of antidiphtheria
serum are injected intramuscularly immediately after testing the
sensitivity of the patient to the antitoxin depending on the toncity of the
patient.
2. Antibacterial
3. Detoxication.
4. Anti-inflammatory.
5. Antiedematic.
6. Symptomatic.
Treatment of the Diphtheria
162. 1
Infectious Mononucleosis
Synonyms: Pfeiffer’s glandular fever,
kissing disease
1. Assotiation with the Epstein–Barr virus (EBV).
The incubation period is 7–9 days.
2. It predominantly affects adolescents.
3. System poliadenopathia.
2. Hepatosplenomegaly.
3. Peripheral blood monocytosis.
4. Paul-Bunnel (92,5%) Tomchik reaction (90,7%).
5. Long-termclinical course with relapse (till 2 month).
Localy
- Any form of the acute tonsillitis (katarrhal, membranous, necrotic)
- Sometimes petechial rash и exantema on the mouth mucous membrane,
- Hemorrhage on the margin of the soft & hard palate, cheeks.
Treatment:
1. Like any acute tonsillitis & Symptomatic.
2. Anti-viral (anti-EBV serum).
163. 2
1. Genaral condition is normal.
2. Body’s temperature is normal.
3. Pharyngeal pain is absent.
4. Lymphadenitis (painfull).
5. Dull greyish membrane formation on one tonsil. It is easily
detachable. Ulcer crater with greyish fundus & Irregular border.
6. Spirochаeta buccalis + bac.fusiformis (saprophits!).
Treatment: = acute tonsillitis
1. Penicillinum i/m х7 days.
2. Gargling with КМО4, Н2О2...
3. Coagulation the ulcer by
5% Iodium spirituosae, 40% AgNO3…
4. Vitaminotherapy, high-calorie diet, nourishing diet …
Plaut–Vincent angina (trench mouth)
Finland tonsillitis
164. 2
Acute (catarrhal, pseudomembranous,
membranous-ulceric)
Trivial (light) form:
- general condition is satisfactory, subfebrility,
- possible spontaneous convalescence in 2-3 weeks,
Serious form (like diphtheria):
- Severe general condition, febrility,
- regional lymphadenitis,
- lingering clinical course, treatment with temporary benefit
Chronic form (month - years):
- often after long-term care by antibiotics,
- general condition is satisfactory, subfebrility,
- yelowish long-term membranes on soft palate, tonsills, posterior
wall of pharynx, isn’t changed after usual treatment
Fungal acute tonsillitis
+ stomatitis, glosittis
(Candida albicans)
165. 2
Diagnosis:
- only after exclusion diphtheria,
- identification of Candida,
- positive benefit after proof antifungal therapy
Treatment:
- cessation of antibioticotherapy,
- Local & system antifungal therapy (nystatinum, laevorinum,
nitrofunginum, mycosporum…)
- obligatory restorative & stimulative therapy
Fungal acute tonsillitis
+ stomatitis, glosittis
(Candida albicans)
170. 1. More than 2 acute tnsillitis a year (anamnesis morbi).
2. Purulent discharge from tonsillar crypt.
3. Hyperemia, hyperplasia, edema ant.&post. palatine arch. Scar between
tonsills and tonsillar pillar.
4. Regional lymphadenitis (lymphnodes before ant.margin
m.sternocleudomastoideus in upper 1/3.
Reliable (trustworthy) symptoms of chronic tonsillitis
171. Symptoms
of decompensations
Absent
In time acute stage
Continiously
Lucovsky’s
Compensation (stage)
SubCompensation
DeCompensation
Preobradgensky’s
Simple
Toxico-allergic 1st stage
Toxico-allergic 2nd stage
Classification of chronic tonsillitis
172. 1. Clinical (metatonsillar & related deseases):
- local: paratonsillitis, parapharyngitis, retropharyngitis,
purulent lymphadenitis, neck phlegmon...
- general: rheumatic fever, miocarditis, arthritis,
glomerulonephritis...
2. Laboratory:
- general: “+” rheumatic-test (СRP, seromucoid..),
- ECG-pathology, GBT, GUT
- local: functional activity of lymphocytes after microbal antigen
stimulation...)
Symptoms of decompensation of chronic tonsillitis =
Sign of lesion another organs and systems of ograns:
175. 1. Conservative: - general
- local (Lucovsky’s, Kolomiychenko’s,
Kischuk’s schema).
2. Surgical (tonsillectomy).
3. Half-surgical (cryotonsillotomy, ultrasound cryotonsillotomy,
cript orifice cuting by spesial knife or LASER evaporator).
Treatment of chronic tonsillitis
176. General:
1. Increasing general reactivity for prevention acute tonsillitis
(regimen of work & rest, nourishing diet (high-calorie diet),
physical trayning, sanatorium-and-spa treatment...);
2. Desensitation (nonspecific, specific - strptpcocci allergen on the
surface of tonsills...)
Local:
Lukovsky’s schema:
1st week: а) - washing crypt 1t. a day,
б) - painting iodine-glycerin 1t. a day;
2nd week: - а), б) - every other day, + massage of tonsills;
3d week: - а) и б) - twice a week, + snoot-quartz endooraly.
Conservative therapy of chronic tonsillitis 1
177. Kolomiychenko’s schema:
1. 1st course = Lukovsky’s schema (but... washing by penicillini, gargling
with календулой, painting by iodine solution, from 2nd week - snoot-
quartz endooraly, from 3rd week - high frequency therapy on tonsills);
2. Interruption 1-3 months;
3. 2nd course - tonsillar crypt stopping (filling) (1t. in 7 days N4-8)
+ ultrasound therapy on tonsills N10).
Kischuk’s schema:
1. Tonsillar massage (1t. a day N10).
2. Lugol’s (iodine-glycerin) solution painting (1t. a day N10).
3. Thymomimetic’s intratonsillar injection (thymogen) (1t. a day N10).
4. Magnetic therapy (1t. a day N10).
+ general 5. Loratadinum 0.01 (1t. a day х10).
6. Extract Alloes 1ml i/m (1t. a day х10).
7. Exinacea 2.2ml i/m every other day (N5).
8. Vit B1-B6 5% 1ml i/m every other day (N10).
Conservative therapy of chronic tonsillitis (local) 2
178. Indications for tonsillectomy:
1. Conservative treatment twice a year 2 years without benefit,
2. Decompensation stage of chronic tonsillitis.
- local sign (paratonsillitis, parapharyngitis, retropharyngitis...),
- general sign (metatonsillar complications - rheumatic fever..)
Contraindications for tonsillectomy:
1. General continuous:
- any organs deseases in decompensation stage,
- blood desease with coagulopathy,
- tumor any malignancy & localisation,
- psychotic deseases.
2. General temporary: (infectious deseases,pregnancy…)
3. Local temporary: (acute tonsillitis, otitis, thynitis…).
4. Local continuous: (carotid artery anomaly – tonsil’s pulsation...)
Surgical treatment of chronic tonsillitis - tonsillectomy
179. 3
If simultaneously indications & contraindications for surgical
treatment (tonsillect6omy) are present:
1. Indications for tonsillectomy:
- conservative treatment twice a year 2 years without benefit,
- decompensation stage of chronic tonsillitis.
&
2. Contraindications for tonsillectomy:
- general (continuous, temporary),
- local (continuous, temporary)
Half-surgical treatment of chronic tonsillitis
180. Chronic tonsillitis
Acute tonsillitis (anamnesis)
Purulent discharge from crypt
Changing palatine folds regional
Lymphadenitis
--
Hypertrophy of palatine tonsills
--
--
--
--
Hypertrophy all of tonsills
Differential diagnosis between
Chronic tonsillitis & hypertrophy of palatine tonsills
Treatment (tonsillotomy): - if the 3rd stage &
- if the 2nd stage with swallowing or breathing disturbances