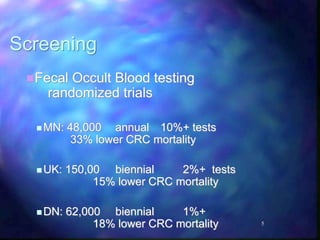
This document discusses advances in colorectal cancer treatment over the past century. In the early 1900s, surgery was the only option. In the 1960s, chemotherapy was introduced with 5-Fluorouracil being the first drug. Screening became important in the 1970s. Between 1995-present, prevention strategies improved along with adjuvant therapy using multiple chemotherapy drugs. Personalized medicine is now allowing for targeted drugs and precision treatment based on a patient's genetic profile. Continued research promises new immunotherapies and genetically engineered treatments that could further improve outcomes.