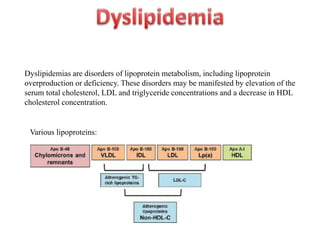
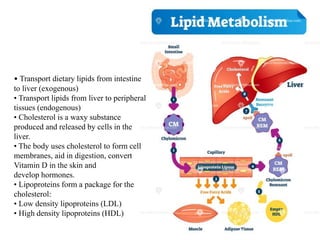
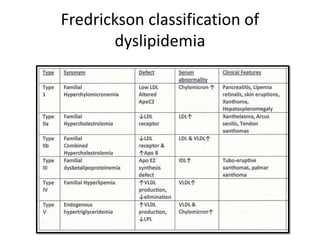
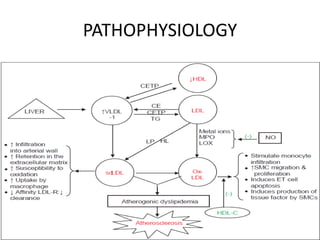
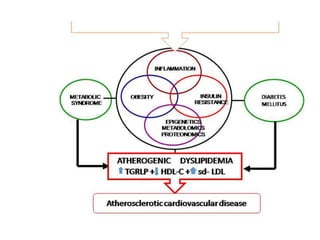
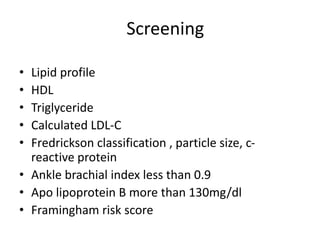
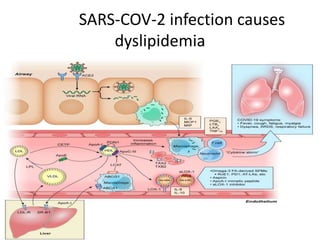
This document discusses dyslipidemias, which are disorders of lipoprotein metabolism that can cause abnormal cholesterol and triglyceride levels. It describes how different lipoproteins such as LDL and HDL transport lipids around the body. It also outlines screening recommendations and classification systems for dyslipidemias. Treatment options are discussed, including statins and other drugs that target cholesterol levels. Guidelines for treatment goals from organizations like the AHA are presented. Considerations for dyslipidemia management in COVID-19 patients and advances in treatments like PCSK9 inhibitors are also summarized.