DOSAGE FORMS FOR
PERSONALIZEDMEDICINE
PRESENTED BY-
Janvi Lokare (06)
Alisha Shaikh (12)
Radhika Vishwakarma (14)
F.Y.M.PHARM
(PHARMACEUTICS)
Dr. L. H. Hiranandani College of Pharmacy, Ulhasnagar-03
06-02-2026
1
INTRODUCTION
Personalized medicine refersto the application of patient-
specific profiles, incorporating genetic and genomic data
as
3
well as
clinical
individual risks
and environmental factors,to
assess and tailor prevention
and disease-
management strategies
Several terms, including “precision medicine,” “stratified
medicine,” “targeted medicine,” and
“pharmacogenomics,” are sometimes used
interchangeably with “personalized medicine.”
4.
INTRODUCTION
Early Examples ofPersonalized Medicine
1907: Reuben Ottenberg reports the first known blood
compatibility test for transfusion using blood
typing techniques and cross-matching between donors and
patients to prevent hemolytic transfusion reactions.
1956: The genetic basis for the selective toxicity of fava beans
(“favism”) and the antimalarial drug primaquine is
discovered to be a deficiency in the metabolic enzyme,
glucose-6- phosphate dehydrogenase (G6PD).
1977: Cytochrome P450 2D6, a polymorphic metabolizing
enzyme, is identified as the culprit for causing some
patients to experience an “overdose” or exaggeration
of the duration and intensity of the effects of
debrisoquine, a drug used for
treating hypertension. 4
5.
DEFINITION
A formof medicine that uses information about a person’s genes,
proteins, and environment to prevent, diagnose, and treat disease
Providing the right treatment to the right patient, at the right dose
at the right time
Understanding Human Genome
Simpler methods identify
genetic information
Genetic Information specific
to individual
Presele
ct
effec 5
6.
Advantages of personalizedmedicines
Provides right drug to the right patient at the right dose
Improves drug efficacy
Reduces adverse drug reactions
Enables dose optimization
Improves patient safety
Allows early disease prediction and diagnosis
Enhances treatment outcomes
Promotes rational drug use
Cost-effective by avoiding trial-and-error therapy
Improves patient compliance
PHARMACOGENETICS
Pharmacogenetics isthe study of influences of a gene on
therapeutic and adverse effects of drugs
Pharmacogenetics is also defined as the study of
inherited
variation in drug-metabolizing enzymes and drug
responses
Pharmacogenetics
Pharmakon- Drug
Genetikos- Generative
(origin)
9
10.
PHARMACOGENETICS
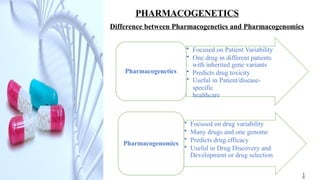
Difference between Pharmacogeneticsand Pharmacogenomics
• Focused on Patient Variability
• One drug in different patients
with inherited gene variants
• Predicts drug toxicity
• Useful in Patient/disease-
specific
healthcare
Pharmacogenetics
• Focused on drug variability
• Many drugs and one genome
• Predicts drug efficacy
• Useful in Drug Discovery and
Development or drug selection
Pharmacogenomics
1
0
11.
PHARMACOGENETICS
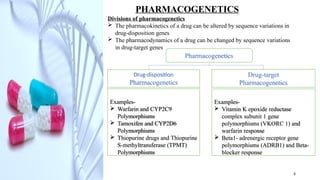
Divisions of pharmacogenetics
The pharmacokinetics of a drug can be altered by sequence variations in
drug-disposition genes
The pharmacodynamics of a drug can be changed by sequence variations
in drug-target genes
Pharmacogenetics
Drug-disposition
Pharmacogenetics
Drug-target
Pharmacogenetics
Examples-
Vitamin K epoxide reductase
complex subunit 1 gene
polymorphisms (VKORC 1) and
warfarin response
Beta1- adrenergic receptor gene
polymorphisms (ADRB1) and Beta-
blocker response
Examples-
Warfarin and CYP2C9
Polymorphisms
Tamoxifen and CYP2D6
Polymorphisms
Thiopurine drugs and Thiopurine
S-methyltransferase (TPMT)
Polymorphisms
9
12.
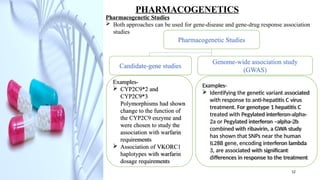
Examples-
Identifying thegenetic variant associated
with response to anti-hepatitis C virus
treatment. For genotype 1 hepatitis C
treated with Pegylated interferon-alpha-
2a or Pegylated interferon –alpha-2b
combined with ribavirin, a GWA study
has shown that SNPs near the human
IL28B gene, encoding interferon lambda
3, are associated with significant
differences in response to the treatment
PHARMACOGENETICS
Pharmacogenetic Studies
Both approaches can be used for gene-disease and gene-drug response association
studies
Pharmacogenetic Studies
Candidate-gene studies
Genome-wide association study
(GWAS)
Examples-
CYP2C9*2 and
CYP2C9*3
Polymorphisms had shown
change to the function of
the CYP2C9 enzyme and
were chosen to study the
association with warfarin
requirements
Association of VKORC1
haplotypes with warfarin
dosage requirements
12
13.
PHARMACOGENETICS
Role of Pharmacogeneticsin Pharmaceutical Industry
Pharmacogenetics has a threefold role in the pharmaceutical
industry including-
Studying drug metabolism and pharmacological effects
Predicting genetically determined adverse reactions
(ADRs)
Drug discovery and development and as an aid to planning
clinical trials
Can identify new targets. For example-
a) Genome wide assessment could identify genes
whose expression differentiate inflammatory process
b) A compound could be identified that can change
expression
of gene responsible for inflammatory process
c) That compound can serve as starting point for
anti-inflammatory drug development
13
14.
CATEGORIES OF PATIENTSFOR
PERSONALISED MEDICINE
Patients are mainly classified depending upon the genetic
polymorphism:
Genetic polymorphism
Epigenetic and other factors
Cytochrome P450 genetic polymorphism
Different families of enzymes polymorphism
Focusing on genomics, we have identified three categories for PM :-
Optimizing drug response: gene-drug interactions
Gene-based drug targeting
Prediction and diagnosis
14
15.
Genetic Polymorphism
Genetic polymorphismrefers to the presence of
variations in DNA sequence among individuals within a
population.
These variations can:
Alter how drugs are absorbed
Affect drug metabolism
Change drug action at receptor sites
Influence drug elimination
Because of genetic polymorphism, the same drug dose
may be:
Effective in one patient
Ineffective in another
Toxic in a third patient
Therefore, identifying genetic polymorphism helps in
selecting the appropriate drug and dose for an
individual.
16.
Epigenetic and OtherFactors
Epigenetics involves changes in gene expression without
changes in DNA sequence.These changes are influenced
by external and internal factors.
Important epigenetic and other factors include:
Age (children and elderly respond differently)
Gender (hormonal differences affect drug response)
Body weight and composition
Diet and lifestyle habits
Environmental exposure
Disease conditions like liver or kidney disorders.
These factors influence pharmacokinetics and
pharmacodynamics, making personalized treatment
necessary.
17.
Cytochrome P450 Genetic
PolymorphismCytochrome P450 enzymes play a crucial role in drug
metabolism, especially in the liver.
Genetic variations in CYP450 enzymes lead to different metabolizer
types:
• Poor metabolizers – slow drug metabolism → toxicity
• Intermediate metabolizers -- Extensive metabolizers – normal
metabolism
• Ultra-rapid metabolizers – fast metabolism → reduced efficacy
Common CYP enzymes include:CYP2D6
• CYP2C9
• CYP2C19
• CYP3A4
Knowing a patient’s CYP450 status helps clinicians to adjust drug dose
and avoid adverse reactions.
18.
Different Families ofEnzyme Polymorphism
Some drug-metabolizing enzymes show genetic polymorphism, leading
to variation in drug response and toxicity among individuals.
1. Thiopurine Methyltransferase (TPMT)
TPMT enzyme breaks down thiopurine drugs used in leukemia and autoimmune
disorders. Genetic deficiency of TPMT causes accumulation of thiopurines,
leading to severe toxicity. Therefore, blood testing is done before treatment.
2. UDP- glucuronosyltransferase family-1 member-1 (UGT1A1)Enzyme
UGT1A1 enzyme is responsible for metabolism of irinotecan used in colorectal
cancer. Deficiency of this enzyme leads to toxic drug accumulation causing
bone marrow suppression, infection, or death. Genetic testing helps in dose
customization.
3. Dihydropyrimidine Dehydrogenase (DPYD)
DPYD enzyme metabolizes 5-fluorouracil and related chemotherapy drugs.
Deficiency results in reduced breakdown of 5-FU, leading to severe or fatal
drug reactions.
19.
Focusing on Genomics– Three
Categories for PM :-
Optimizing Drug Response: Uses gene–drug
interaction to improve efficacy and reduce side effects.
Gene-Based Drug Targeting: Targets specific genes;
used in cancer and genetic diseases.
Prediction & Diagnosis: Helps predict disease risk and
enables early, accurate diagnosis.