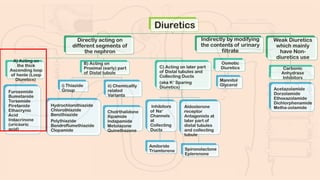
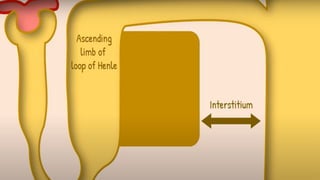
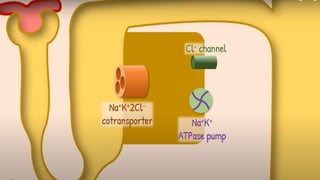
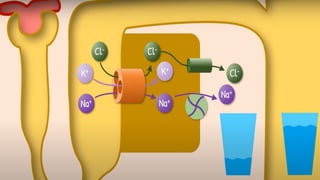
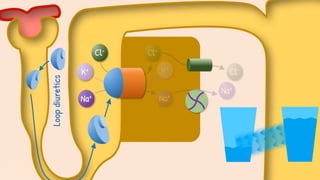
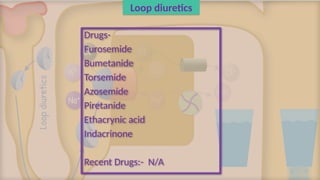
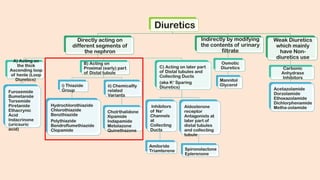
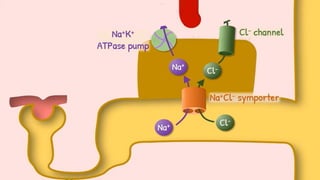
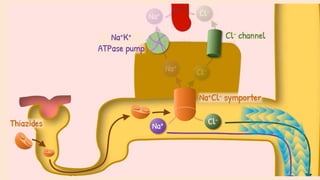
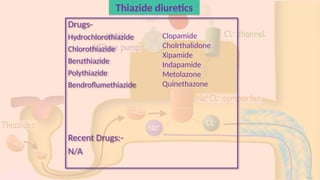
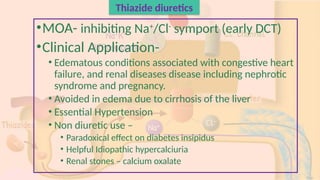
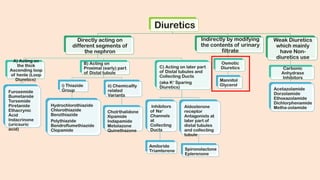
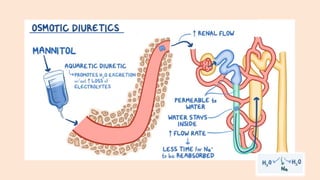
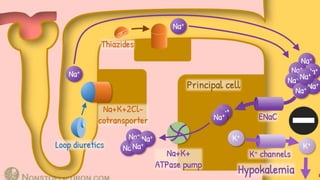
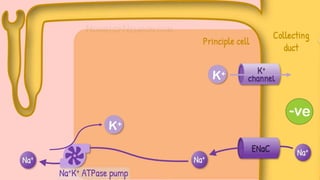
The document discusses various categories of diuretics including loop, thiazide, and osmotic diuretics, detailing their mechanisms of action, clinical applications, side effects, and drug interactions. It outlines the physiological impacts and therapeutic uses of these medications in conditions like congestive heart failure, hypertension, and renal disease. Additionally, it mentions combinations of diuretics and recent drugs related to their use.