Three key points about disorders of thought content:
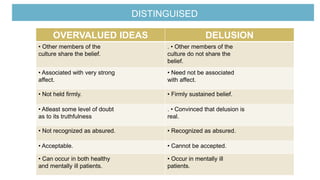
1. There are two main types - overvalued ideas and delusions. Overvalued ideas are abnormal beliefs that are neither delusional nor obsessional in nature but preoccupy the sufferer.
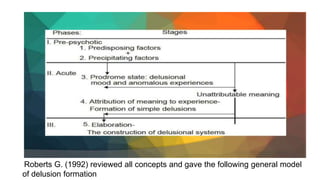
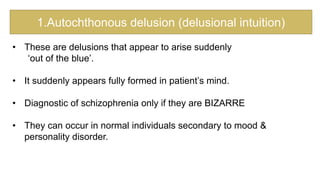
2. Delusions are defined as false beliefs that are firmly held despite evidence contradicting them, and are not shared by other members of the culture. They can be primary, arising from internal morbid processes, or secondary, arising from other psychological phenomena.
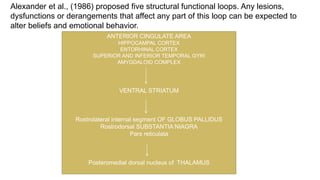
3. Factors involved in generating and maintaining delusions include dysfunction in brain regions, psychological mechanisms like maintaining self-esteem, and social factors like poverty of communication that reinforce the delusional beliefs