Downloaded 84 times

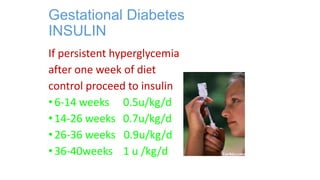
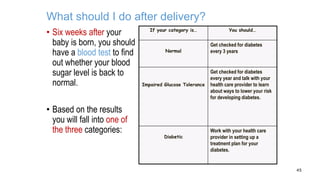


Gestational diabetes mellitus (GDM) affects 3-10% of pregnancies, primarily due to inadequate maternal insulin response leading to maternal and fetal complications. Screening is typically performed between 24-28 weeks, and management involves maintaining blood sugar levels through diet, physical activity, and possibly insulin therapy. Post-delivery, women are advised to undergo glucose testing to monitor for potential diabetes development.










![H:\Capp Diabetes In Pregnancy 04 08 3 With Monitoring[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hcappdiabetesinpregnancy04-083withmonitoring1-100304133925-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


















![H:\Diabetes In Pregnancy 1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hdiabetesinpregnancy11-100304134743-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















































