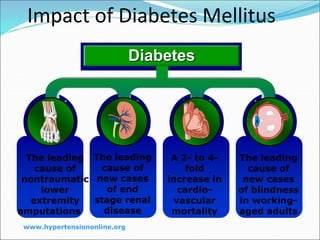
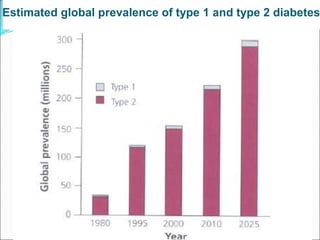
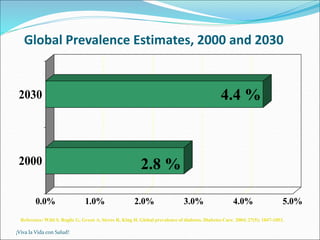
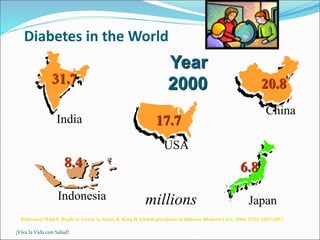
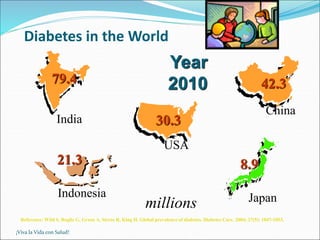
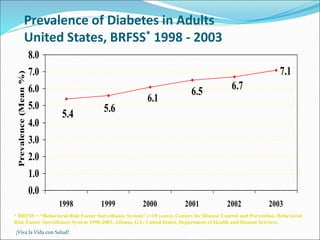
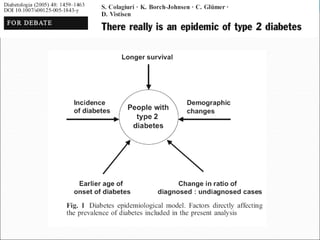
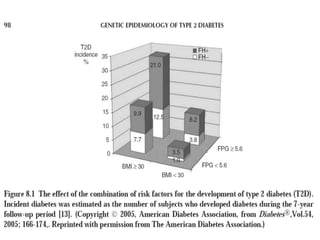
The document discusses diabetes trends globally and provides information on the classification, presentation, and risk factors of diabetes. It notes that worldwide diabetes prevalence is expected to increase significantly by 2030, with most of the growth occurring in developing regions. The two main types of diabetes - type 1 and type 2 - are described, with type 2 accounting for 90-95% of cases. Risk factors for type 2 diabetes include genetics, obesity, diet, and lifestyle factors. Carbohydrate intake and dietary fiber intake are discussed as dietary risk factors.


![ On the other hand, there is rather more support for
the suggestion that foods rich in slowly digested or
resistant starch or high in dietary fiber (nonstarch
polysaccharide) might be protective In controlled
experiments, diets high in soluble fiber-rich foods [20]
or foods with a low glycemic index are associated with
improved diurnal blood glucose profiles and long-term
overall improvement in glycemic control, as evidenced
by reduced levels of glycated hemoglobin](https://image.slidesharecdn.com/diabetesmellitusnew-230423034342-21508f81/85/Diabetes-Mellitus-ppt-38-320.jpg)
![ Some other studies provide indirect support for this
hypothesis. Diabetes risk appears to be lower in
Seventh-Day Adventists who are vegetarians than in
those who are not strict vegetarians [22].
The diet of vegetarians is characterized by a high
intake of dietary fiber, but differs in other ways from
that of nonvegetarians. In addition to not eating meat
and animal products, vegetarians also have less
saturated fat,more polyunsaturated fat and a diet
which differs in micronutrient composition when
compared with nonvegetarians.](https://image.slidesharecdn.com/diabetesmellitusnew-230423034342-21508f81/85/Diabetes-Mellitus-ppt-39-320.jpg)
![DIETARY FATS
More than 60 years ago,
Himsworth [23] suggested
that high intakes of fat
increased the risk of
diabetes in populations
and individuals.
In the San Luis Valley
Diabetes Study, a high fat
intake was associated with
an increased risk of type 2
diabetes and impaired
glucose tolerance (IGT)
[25];](https://image.slidesharecdn.com/diabetesmellitusnew-230423034342-21508f81/85/Diabetes-Mellitus-ppt-40-320.jpg)
![ The strong positive associations
between animal protein and saturated fatty acids
and vegetable protein and dietary fiber mean that
it is almost impossible to disentangle separate
effects in epidemiological studies.
High intakes of proteins, especially animal
protein, appear to be associated with an increased
risk of nephropathy in type 1 diabetes [44], so
restriction of protein may help to delay progression
of microalbuminuria to clinical nephropathy](https://image.slidesharecdn.com/diabetesmellitusnew-230423034342-21508f81/85/Diabetes-Mellitus-ppt-45-320.jpg)
![smooking
The role of smoking
as a risk factor for type 2 diabetes has received
relatively little attention. Smoking induces insulin
resistance [51], and cigarette smokers have
been shown to be relatively glucose intolerant and
Dyslipidemic
Thus, smokers might be expected to be at
considerably increased risk of type 2 diabetes.](https://image.slidesharecdn.com/diabetesmellitusnew-230423034342-21508f81/85/Diabetes-Mellitus-ppt-48-320.jpg)





















![Diabet med 2009_sep_26(9)_864-71[1]](https://cdn.slidesharecdn.com/ss_thumbnails/diabetmed2009sep269864-711-110509232950-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)















![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









