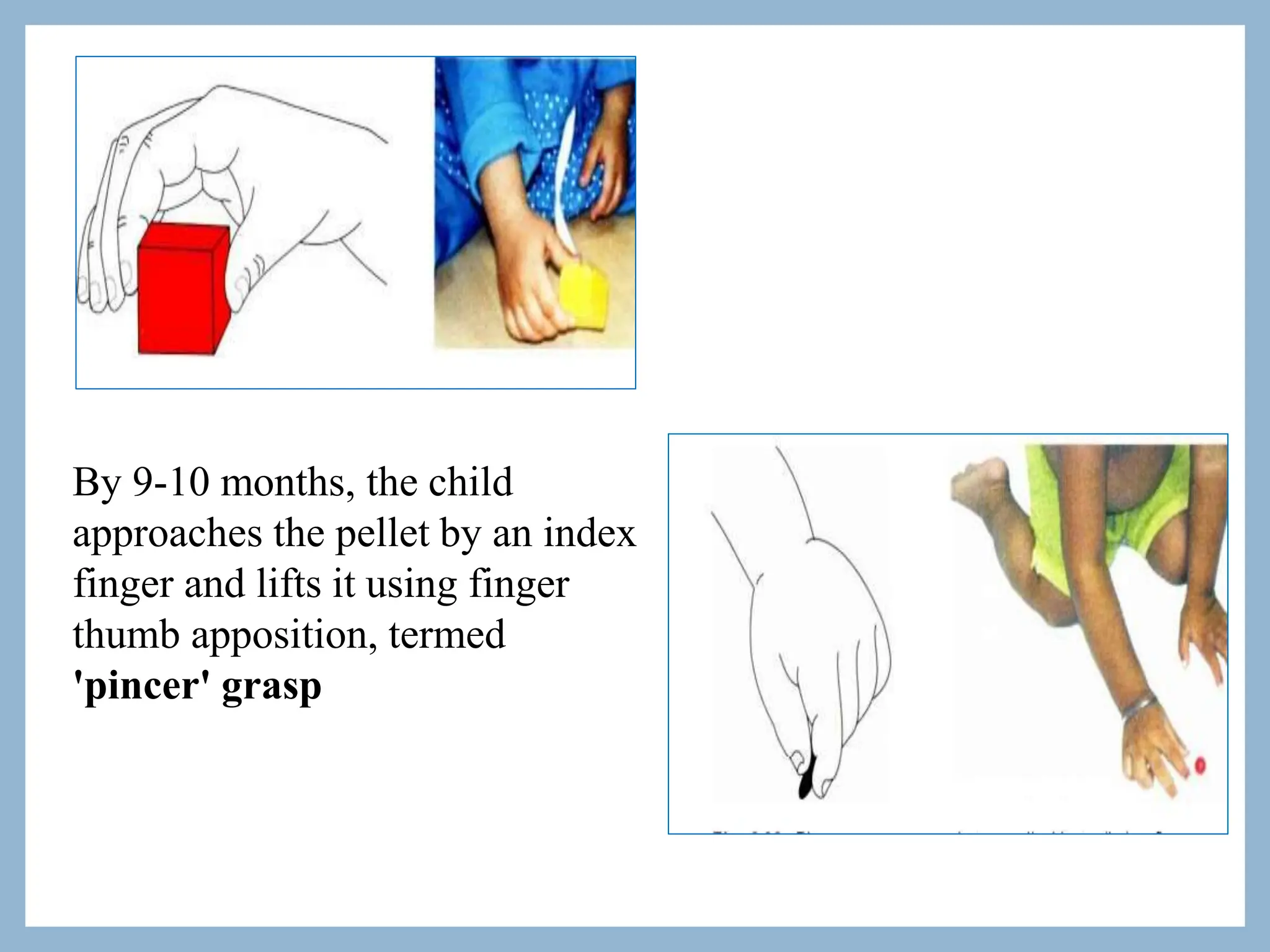
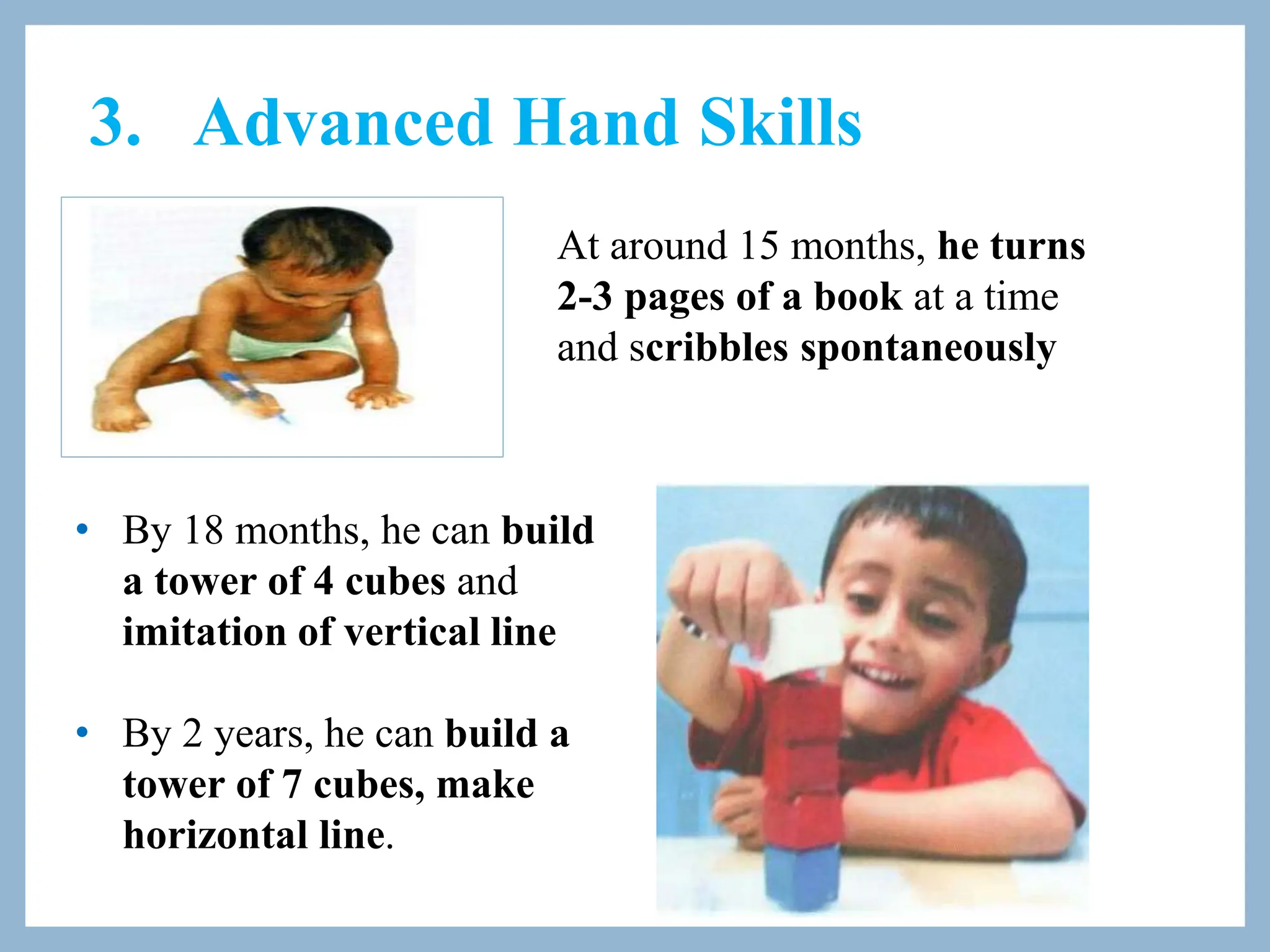
The document discusses the differences between growth and development in children, emphasizing that growth is quantitative and development is qualitative. It outlines various factors affecting development, such as genetics, maternal health, and social conditions, while detailing milestones in gross motor, fine motor, personal, social, and language development from birth to age five. Additionally, it highlights the importance of early stimulation, the impact of television on development, and challenges faced by children in developing countries.