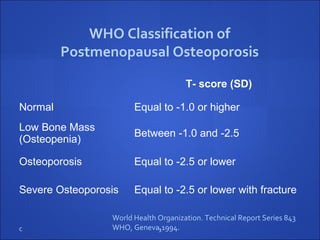
The document summarizes the WHO Classification of Postmenopausal Osteoporosis published in 1994. It establishes diagnostic criteria for normal bone mass, osteopenia, and osteoporosis based on T-scores measured by DXA of the spine, hip, or forearm in postmenopausal Caucasian females. Osteoporosis is defined as a T-score of -2.5 or lower. The classification system is intended to assess disease prevalence in populations and does not necessarily imply prior bone loss in individuals with low bone mass.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




