![DENGUE
SYNDROME
(DENGUE &
DENGUE
HEMORRHAGIC
FEVER)
DR. VISHAL BATHMA [MBBS,
MBA(HA),MD]](https://image.slidesharecdn.com/dengue2-200620042853/85/Dengue2-1-320.jpg)


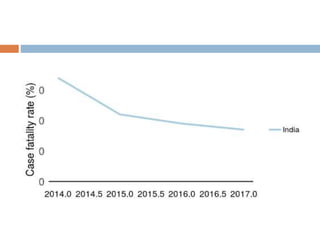
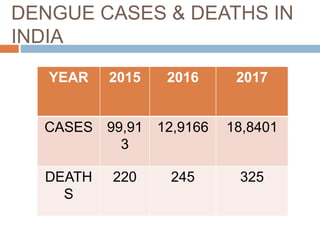
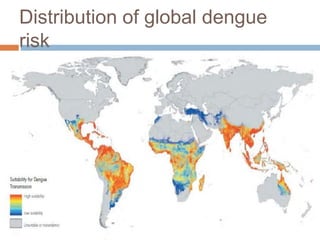



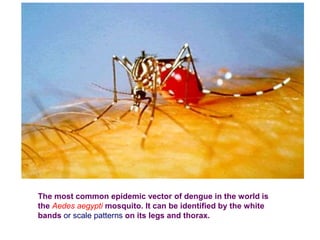



























Dengue is a mosquito-borne viral disease that has been an increasing problem in India. It is transmitted by the Aedes aegypti mosquito. There are typically two peaks of dengue outbreaks annually in India. The number of reported cases and deaths has been increasing, with over 99,000 cases and 220 deaths in 2015. The goal of the Global Strategy for Dengue Prevention and Control is to reduce dengue mortality by at least 50% and morbidity by 25% by 2020 through reducing mosquito populations, public education, and emergency response planning. Diagnosis involves virus isolation, antibody detection, or PCR testing. There is no vaccine for dengue prevention currently.



































































