Downloaded 70 times

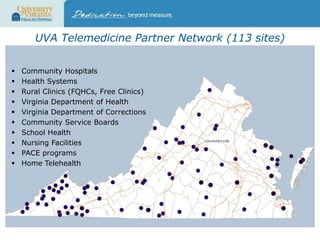
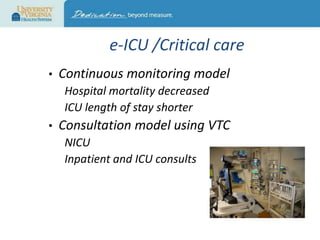
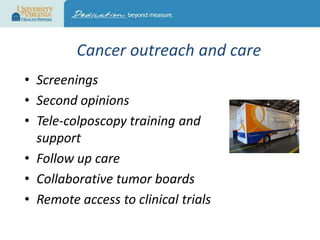



This document discusses telehealth and its role in an evolving healthcare environment. It provides definitions of telehealth and describes its benefits for patients, healthcare systems, and public health. The University of Virginia Center for Telehealth is presented as a model program that provides clinical services to over 33,000 patients annually across many specialties using live videoconferencing and remote patient monitoring. Opportunities for advancing telehealth include improving federal and state payment policies, streamlining licensing and credentialing, developing the telehealth workforce, and conducting more research on outcomes and best practices.























































































