Stopping Depression Killing the Medical Profession
•
0 likes•97 views

The document discusses mental health issues among medical professionals. It notes that doctors are almost twice as likely to die by suicide compared to the general population. The author argues that stigma, discrimination, and a lack of work-life balance are exacerbating depression within the medical field. To address this, the author calls for leadership from those with lived experience of mental health issues, similar to how civil rights leaders advocated for racial equality. Reform is needed to stop depression from negatively impacting the medical profession.
![decemBER 2014/JANUARY 2015 vicdoc
medical 11
“work/life balance”. I would argue
that if a medical career promises
almost twice the risk of suicide and
a working life that is heavily overlaid
with psychological stress, burn out
and depression we will find it much
harder to attract top candidates in
the future. Medicine is a profession
that is heavily dependent on a quality
workforce. Our current failings are
jeopardising the quality of our future
workforce.
The roadblocks
Mental health stigma, discrimination
and prejudice are not “medical
problems” but cultural phenomenon.
Stigma is not driven by “evidence”:
it is an arbitrary differentiation
between the acceptable “us” and the
unacceptable “them”. In fact stigma,
discrimination and prejudice are the
application of dogma, superstition
and fear, not evidence. I would
argue that you can’t “cure” stigma,
discrimination and prejudice by
dousing them with research-driven,
professionally detached “evidence”
because stigma, discrimination
and prejudice are “evidence-free
zones”. Resolution requires empathy,
understanding and connection, not
professional detachment.
A medically based “model of care”
approach does not work.
There are existing examples
of stigma, discrimination and
prejudice reduction models which
can be applied to mental health.
The US Civil Rights Movement
is such an example. Putting aside
the obvious differences between
racial discrimination and mental
health discrimination, there are
commonalities that allow the
resolution processes of racial stigma,
discrimination and prejudice that can
be used to build a scaffold for doctors
and mental health reform.
One of the crucial elements required
for the US Civil Rights Movement
is a critical mass of leaders with
authenticity gained from “lived
experience”.
Martin Luther King Jr. was a leader
who catalysed change in the area of
racial discrimination. He was not
a researcher or academic or policy
maker or administrator. He was
a leader who had the courage to
challenge the status quo to create a
better future for others.
The future
The question of whether depression
(and other mental health conditions)
is killing the medical profession
should not be in dispute. The
evidence concerning suicide,2
psychological distress and mental
health problems in the medical
profession1
is irrefutable; “business as
usual” is not a reasonable option. But
can we learn from the experiences of
others? The US has transformed from
the abolition of slavery in 1863, the
Civil Rights Movement in the 1960s
to Barack Obama as President in
2009.
The Emancipation Proclamation of
1863 provided a legislative framework
to outlaw slavery in the US. Abraham
Lincoln was a leader who saw the
need to unite a divided country. But
he had no authenticity. He was not a
slave. He could only enact legislation.
It took a further 100 years for leaders
like Martin Luther King Jr. to break
the chains of stigma, discrimination
and prejudice. Martin Luther King
Jr. had both lived experience and
the cultural authority to end slavery
morally. It is bittersweet irony that
both Abraham Lincoln and Martin
Luther King Jr. had a history of
depression.3
So as we look towards the future we
should reflect on the past. History
has demonstrated that leaders with
authenticity gained from lived
experience are an integral part of
delivering sustainable outcomes where
stigma, discrimination and prejudice
are major roadblocks to acceptance.
It remains to be seen as to whether
the medical profession is prepared
to accept leadership with lived
experience as valid co-contributors
to complement the existing
professionally detached and evidence-
based methods.
The medical profession has provided a
legal framework to outlaw workplace
discrimination concerning doctors
with a history of mental health issues.
But if it takes a further 100 years
to accept the need for the inclusion
of leaders with lived experience and
cultural authority to help break the
chains of stigma, discrimination
and prejudice then I fear we will
needlessly bury many friends and
work colleagues.
What our profession desperately
needs are these types of leaders to
drive cultural change in the space
of doctors and mental health.4
Depression (and other mental health
conditions) has been killing the
medical profession for long enough.
I think it is time for real change.
Dr David Noble,
MBBS FANZCA
David Noble is a consultant
anaesthetist in private practice in
Bendigo, Victoria. He is the Founder
of BDI health, a health innovation
and transformation company, an
Adjunct Research Fellow (honorary)
at Federation University and an
Ambassador for beyondblue.
Copyright remains with the author.
For those seeking support, contact
AMA Victoria’s Peer Support Service
(for doctors by doctors) 1300 853
338, Lifeline 13 11 14 or beyondblue
1300 22 4636.
1. beyondblue, National Mental Health Survey of Doctors and Medical Students October 2013 [cited 2014 Oct 14].
http://www.beyondblue.org.au/docs/default-source/default-document-library/bl1132-report---nmhdmss-full-report_web
2. Lubin G., “The 19 Jobs Where You’re Most Likely To Kill Yourself”, Business Insider Australia, 19 October 2011 [cited 2014 Oct 14].
http://www.businessinsider.com.au/most-suicidal-occupations-2011-10?op=1#19-natural-scientists-are-128-times-more-likely-to-commit-
suicide-than-average-1
3. Ghaemi N., A First-Rate Madness: Uncovering the Links Between Leadership and Mental Illness, New York, Penguin, 2011.
4. Evans K., “Treatment ills as doctors battle depression”, The Age. 26 September 2014 [cited 2014 Oct 14].
http://www.theage.com.au/national/treament-ills-as-doctors-battle-depression-20140925-10lupw.html](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Stopping Depression Killing the Medical Profession
Similar to Stopping Depression Killing the Medical Profession (11)
Stopping Depression Killing the Medical Profession
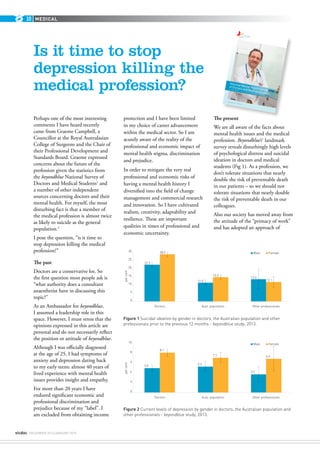
- 1. vicdoc deceMBER 2014/JANUARY 2015 medical10 Is it time to stop depression killing the medical profession? Perhaps one of the most interesting comments I have heard recently came from Graeme Campbell, a Councillor at the Royal Australasian College of Surgeons and the Chair of their Professional Development and Standards Board. Graeme expressed concerns about the future of the profession given the statistics from the beyondblue National Survey of Doctors and Medical Students1 and a number of other independent sources concerning doctors and their mental health. For myself, the most disturbing fact is that a member of the medical profession is almost twice as likely to suicide as the general population.2 I pose the question, “is it time to stop depression killing the medical profession?” The past Doctors are a conservative lot. So the first question most people ask is “what authority does a consultant anaesthetist have in discussing this topic?” As an Ambassador for beyondblue, I assumed a leadership role in this space. However, I must stress that the opinions expressed in this article are personal and do not necessarily reflect the position or attitude of beyondblue. Although I was officially diagnosed at the age of 25, I had symptoms of anxiety and depression dating back to my early teens: almost 40 years of lived experience with mental health issues provides insight and empathy. For more than 20 years I have endured significant economic and professional discrimination and prejudice because of my “label”. I am excluded from obtaining income protection and I have been limited in my choice of career advancement within the medical sector. So I am acutely aware of the reality of the professional and economic impact of mental health stigma, discrimination and prejudice. In order to mitigate the very real professional and economic risks of having a mental health history I diversified into the field of change management and commercial research and innovation. So I have cultivated realism, creativity, adaptability and resilience. These are important qualities in times of professional and economic uncertainty. The present We are all aware of the facts about mental health issues and the medical profession. Beyondblue’s1 landmark survey reveals disturbingly high levels of psychological distress and suicidal ideation in doctors and medical students (Fig 1). As a profession, we don’t tolerate situations that nearly double the risk of preventable death in our patients – so we should not tolerate situations that nearly double the risk of preventable death in our colleagues. Also our society has moved away from the attitude of the “primacy of work” and has adopted an approach of 10 Figure 1 Suicidal ideation by gender in doctors, the Australian population and other professionals prior to the previous 12 months - beyondblue study, 2013. Figure 2 Current levels of depression by gender in doctors, the Australian population and other professionals - beyondblue study, 2013. www.beyondblue.org.au 1300 22 4636 National Mental Health Survey of Doctors and Medical Students October 2013 3 Figure 1: Levels of very high psychological distress by gender in doctors, the Australian population and other Australian professionals aged 30 years and below 5.0 6.6 1.6 3.4 0 2 4 6 8 10 percent Doctors Aust. population Other professionals Male Female 0.4 0.6 Approximately 21% of doctors reported having ever been diagnosed with, or treated for, depression and 6% had a current diagnosis. Current levels of depression were similar in doctors in comparison to the general population, but higher than other Australian professionals (6.2% vs. 6.2% vs. 5.3%). (Figure 2). Approximately 9% of doctors reported having ever been diagnosed with or treated for an anxiety disorder (Australian population 5.9%), and 3.7% reported having a current diagnosis (Australian population 2.7%). Figure 2: Current levels of depression by gender in doctors, the Australian population and other professionals 5.0 5.3 3.7 8.1 7.1 6.9 0 2 4 6 8 10 percent Doctors Aust. population Other professionals Male Female Approximately a quarter of doctors reported having thoughts of suicide prior to the last 12 months (24.8%), and 10.4% reported having thoughts of suicide in the previous 12 months. As illustrated in Figure 3, thoughts of suicide are significantly higher in doctors compared to the general population and other professionals (24.8% vs. 13.3% vs 12.8%). Approximately 2% of doctors reported that they had attempted suicide. Figure 3: Suicidal ideation by gender in doctors, the Australian population and other professionals prior to the previous 12 months 22.3 11.5 13.6 28.5 15.0 12.1 percent Doctors Aust. population Other professionals Male Female 30 15 20 25 10 0 5 Figure 1: Levels of very high psychological distress by gender in doctors, the Australian population and other Australian professionals aged 30 years and below 5.0 6.6 1.6 3.4 0 2 4 6 8 10 percent Doctors Aust. population Other professionals Male Female 0.4 0.6 Approximately 21% of doctors reported having ever been diagnosed with, or treated for, depression and 6% had a current diagnosis. Current levels of depression were similar in doctors in comparison to the general population, but higher than other Australian professionals (6.2% vs. 6.2% vs. 5.3%). (Figure 2). Approximately 9% of doctors reported having ever been diagnosed with or treated for an anxiety disorder (Australian population 5.9%), and 3.7% reported having a current diagnosis (Australian population 2.7%). Figure 2: Current levels of depression by gender in doctors, the Australian population and other professionals 5.0 5.3 3.7 8.1 7.1 6.9 0 2 4 6 8 10 percent Doctors Aust. population Other professionals Male Female Approximately a quarter of doctors reported having thoughts of suicide prior to the last 12 months (24.8%), and 10.4% reported having thoughts of suicide in the previous 12 months. As illustrated in Figure 3, thoughts of suicide are significantly higher in doctors compared to the general population and other professionals (24.8% vs. 13.3% vs 12.8%). Approximately 2% of doctors reported that they had attempted suicide. Figure 3: Suicidal ideation by gender in doctors, the Australian population and other professionals prior to the previous 12 months 22.3 28.5 Male Female 30 20 25
- 2. decemBER 2014/JANUARY 2015 vicdoc medical 11 “work/life balance”. I would argue that if a medical career promises almost twice the risk of suicide and a working life that is heavily overlaid with psychological stress, burn out and depression we will find it much harder to attract top candidates in the future. Medicine is a profession that is heavily dependent on a quality workforce. Our current failings are jeopardising the quality of our future workforce. The roadblocks Mental health stigma, discrimination and prejudice are not “medical problems” but cultural phenomenon. Stigma is not driven by “evidence”: it is an arbitrary differentiation between the acceptable “us” and the unacceptable “them”. In fact stigma, discrimination and prejudice are the application of dogma, superstition and fear, not evidence. I would argue that you can’t “cure” stigma, discrimination and prejudice by dousing them with research-driven, professionally detached “evidence” because stigma, discrimination and prejudice are “evidence-free zones”. Resolution requires empathy, understanding and connection, not professional detachment. A medically based “model of care” approach does not work. There are existing examples of stigma, discrimination and prejudice reduction models which can be applied to mental health. The US Civil Rights Movement is such an example. Putting aside the obvious differences between racial discrimination and mental health discrimination, there are commonalities that allow the resolution processes of racial stigma, discrimination and prejudice that can be used to build a scaffold for doctors and mental health reform. One of the crucial elements required for the US Civil Rights Movement is a critical mass of leaders with authenticity gained from “lived experience”. Martin Luther King Jr. was a leader who catalysed change in the area of racial discrimination. He was not a researcher or academic or policy maker or administrator. He was a leader who had the courage to challenge the status quo to create a better future for others. The future The question of whether depression (and other mental health conditions) is killing the medical profession should not be in dispute. The evidence concerning suicide,2 psychological distress and mental health problems in the medical profession1 is irrefutable; “business as usual” is not a reasonable option. But can we learn from the experiences of others? The US has transformed from the abolition of slavery in 1863, the Civil Rights Movement in the 1960s to Barack Obama as President in 2009. The Emancipation Proclamation of 1863 provided a legislative framework to outlaw slavery in the US. Abraham Lincoln was a leader who saw the need to unite a divided country. But he had no authenticity. He was not a slave. He could only enact legislation. It took a further 100 years for leaders like Martin Luther King Jr. to break the chains of stigma, discrimination and prejudice. Martin Luther King Jr. had both lived experience and the cultural authority to end slavery morally. It is bittersweet irony that both Abraham Lincoln and Martin Luther King Jr. had a history of depression.3 So as we look towards the future we should reflect on the past. History has demonstrated that leaders with authenticity gained from lived experience are an integral part of delivering sustainable outcomes where stigma, discrimination and prejudice are major roadblocks to acceptance. It remains to be seen as to whether the medical profession is prepared to accept leadership with lived experience as valid co-contributors to complement the existing professionally detached and evidence- based methods. The medical profession has provided a legal framework to outlaw workplace discrimination concerning doctors with a history of mental health issues. But if it takes a further 100 years to accept the need for the inclusion of leaders with lived experience and cultural authority to help break the chains of stigma, discrimination and prejudice then I fear we will needlessly bury many friends and work colleagues. What our profession desperately needs are these types of leaders to drive cultural change in the space of doctors and mental health.4 Depression (and other mental health conditions) has been killing the medical profession for long enough. I think it is time for real change. Dr David Noble, MBBS FANZCA David Noble is a consultant anaesthetist in private practice in Bendigo, Victoria. He is the Founder of BDI health, a health innovation and transformation company, an Adjunct Research Fellow (honorary) at Federation University and an Ambassador for beyondblue. Copyright remains with the author. For those seeking support, contact AMA Victoria’s Peer Support Service (for doctors by doctors) 1300 853 338, Lifeline 13 11 14 or beyondblue 1300 22 4636. 1. beyondblue, National Mental Health Survey of Doctors and Medical Students October 2013 [cited 2014 Oct 14]. http://www.beyondblue.org.au/docs/default-source/default-document-library/bl1132-report---nmhdmss-full-report_web 2. Lubin G., “The 19 Jobs Where You’re Most Likely To Kill Yourself”, Business Insider Australia, 19 October 2011 [cited 2014 Oct 14]. http://www.businessinsider.com.au/most-suicidal-occupations-2011-10?op=1#19-natural-scientists-are-128-times-more-likely-to-commit- suicide-than-average-1 3. Ghaemi N., A First-Rate Madness: Uncovering the Links Between Leadership and Mental Illness, New York, Penguin, 2011. 4. Evans K., “Treatment ills as doctors battle depression”, The Age. 26 September 2014 [cited 2014 Oct 14]. http://www.theage.com.au/national/treament-ills-as-doctors-battle-depression-20140925-10lupw.html