HMCS Max Bernays Pre-Deployment Brief (May 2024).pptx
DAY CARE Form masterlist spf2
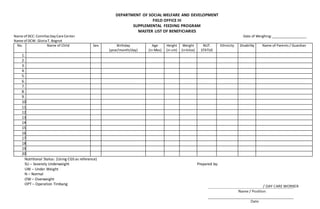
1. DEPARTMENT OF SOCIAL WELFARE AND DEVELOPMENT
FIELD OFFICE III
SUPPLEMENTAL FEEDING PROGRAM
MASTER LIST OF BENEFICIARIES
Name of DCC: ComillasDayCare Center Date of Weighing:___________________
Name of DCW: GloriaT. Bognot
No. Name of Child Sex Birthday
(year/month/day)
Age
(in Mos)
Height
(in cm)
Weight
(inkilos)
NUT.
STATUS
Ethnicity Disability Name of Parents / Guardian
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
Nutritional Status: (Using CGS as reference)
SU – Severely Underweight Prepared by:
UW – Under Weight
N – Normal
OW – Overweight
OPT – Operation Timbang