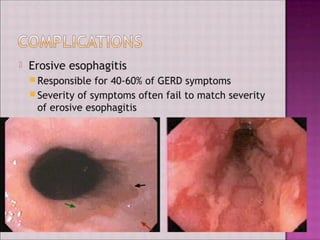
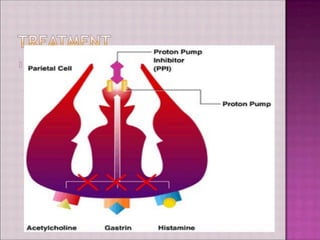
GERD is common, affecting 10-20% of people in western countries weekly. It occurs most commonly in those over age 40. The pathophysiology involves decreased LES pressure, disruption of anatomical barriers like hiatal hernia, impaired esophageal clearance, and impaired mucosal resistance. Clinical manifestations include typical symptoms of heartburn and regurgitation, as well as atypical symptoms. Diagnostic evaluation includes endoscopy and pH monitoring. Treatment involves lifestyle changes, antacids, H2 blockers, PPIs, and sometimes surgery. Complications include erosive esophagitis, stricture, Barrett's esophagus, and cancer.