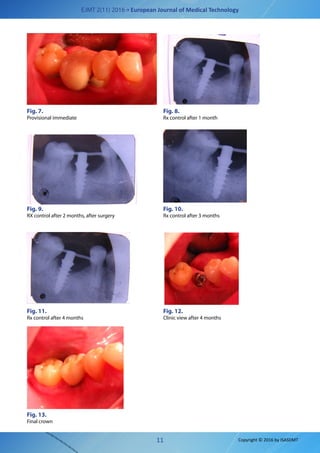
This document summarizes a case study on the usage of a monophasic dental implant. A 56-year-old male patient was treated for an edentulous area in his lower right jaw through a flapless insertion of a single POWER implant from IMMEDIATELOAD SA. The implant was immediately loaded with a temporary crown. Monthly x-rays over 3 months showed gradual bone consolidation around the implant. After osseointegration, a final alloy-composite crown was placed. The case demonstrated promising results for using the latest generation monophasic implant design for an immediate loading solution.