

![554 M. Rall and P. Dieckmann
REFERENCES
1. Berkow LC. Strategies for airway mangement. Best Pract Res Clin Anaesthesiol 2004; 18: 531–548.
2. Brambrink AM, Meyer RR & Krez FJ. [Management of pediatric airway—anatomy, physiology and new
developments in clinical practice]. Anaesthesiol Reanim 2003; 28: 144–151.
3. Brambrink AM & Koerner IP. Advanced trauma life support: how should we manage the airway, and who
should do it? Crit Care 2004; 8: 3–5.
4. Clancy M & Nolan J. Airway management in the emergency department. Emerg Med J 2002; 19: 2–3.
5. Heidegger T, Gerig HJ & Keller C. Comparison of algorithms for management of the difficult airway.
Anaesthesist 2003; 52: 381–392.
6. Hillman PR & Platt PR. Upper airway during anaesthesia. Br J Anaesth 2003; 91: 31–39.
7. Kuczkowski KM, Reisner LS & Benumof JL. Airway problems and new solutions for the obstetric patient.
J Clin Anesth 2003; 15: 552–563.
8. Mayhew JF. Airway management for oral and maxillofacial surgery. Int Anesthesiol Clin 2003; 41: 57–65.
9. McNiece WL & Dierdorf SF. The pediatric airway. Semin Pediatr Surg 2004; 13: 152–165.
10. Munnur U & Suresh MS. Airway problems in pregnancy. Crit Care Clin 2004; 20: 617–642.
11. Rosenblatt WH. Preoperative planning of airway management in critical care patients. Crit Care Med 2004;
32: S186–S192.
12. Wheeler M. Management strategies for the difficult pediatric airway. Middle East J Anesthesiol 2004; 17:
845–873.
13. Ezri T, Szmuk P, Warters RD. et al. Difficult airway management practice patterns among
anesthesiologists practicing in the United States: have we made any progress? J Clin Anesth 2003; 15:
418–422.
14. Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic
attempts. Anesth Analg 2004; 99: 607–613.
15. Rosenblatt WH. The Airway Approach Algorithm: a decision tree for organizing preoperative airway
information. J Clin Anesth 2004; 16: 312–316.
16. Columbia Accident Investigation Board. Columbia Accident Investigation Board Report Vol 1. 2003.
http://www.nasa.gov/columbia/home/CAIB_Vol1.html.
17. Rall M & Gaba D. In Miller R (ed.) Patient Simulators, Miller’s Anesthesia, 6th edn. Philadelphia: Elsevier
Churchill Livingstone, 2005, pp 3073–3104.
18. Gaba DM, Fish KJ & Howard SK. Crisis Management in Anesthesiology. New York: Churchill Livingstone
1994.
19. Howard SK, Gaba DM, Fish KJ et al. Anesthesia crisis resource management training: teaching
anesthesiologists to handle critical incidents. Aviat Space Environ Med 1992; 63: 763–770.
20. Kohn LT, Corrigan JM & Donaldson MS. To Err is Human—Building a Safer Health System. Washington:
National Academy Press; 1999.
21. Gaba DM. Improving anesthesiologists’ performance by simulating reality (editorial). Anesthesiology 1992;
76: 491–494.
22. Weick KE, Sutcliffe KM & Obstfeld D. Organizing for high reliability: processes of collective mindfulness.
Res Organ Behav 1999; 21: 81–123.
23. Klein RL, Bigley GA & Roberts KH. Organizational culture in high reliability organizations: an extension.
Hum Relat 1995; 48: 1–23.
24. Weick KE. South canyon revisited: lessons from high reliability organizations. Wildfire 1995; 4: 54–68.
25. Roberts KH, Stout SK & Halpern JJ. Decision dynamics in two high reliability military organizations. Manag
Sci 1994; 40: 614–624.
26. Roberts KH, Rousseau DM & La Porte TR. The culture of high reliability: quantitative and qualitative
assessment aboard nuclear powered aircraft carriers. J High Technol Manag Res 1994; 5: 141–161.
27. Roberts KH. Some characteristics of high reliability organizations. Organ Sci 1990; 1: 160–177.
28. Roberts KH. Managing high reliability organizations. Calif Manag Rev 1990; 32: 101–114.
29. Roberts KH. New challenges in organizational research: high reliability organizations. Ind Crisis Quart
1989; 3: 111–125.
30. Rochlin TR & La Porte KH. Self-designing high reliability organization: aircraft carrier flight operations at
sea. Nav War Coll Rev 1987; 42(Autumn): 76–90.](https://image.slidesharecdn.com/crmevadpdieckmanbprca051-100910084556-phpapp01/75/Artigo-Safety-culture-and-crisis-resource-management-in-airway-management-16-2048.jpg)
![Safety culture and crisis resource management 555
31. Weick KE. Organizational culture as a source of high reliability. Calif Manag Rev21987; 112–127.
32. Rall M & Gaba D. In Miller R (ed.) Human Performance and Patient Safety, Miller’s Anesthesia, 6th edn.
Philadelphia: Elsevier Churchill Livingstone, 2005, pp 3021–3072.
33. Gaba DM. Anaesthesiology as a model for patient safety in health care. Br Med J 2000; 320: 785–788.
34. Flin R, Fletcher G, McGeorge P, et al. Anaesthetists’ attitudes to teamwork and safety. Anaesthesia 2003;
58: 233–242.
35. Singer SJ, Gaba DM, Geppert JJ, et al. The culture of safety: results of an organization-wide survey in 15
California hospitals. Qual Saf Health Care 2003; 12: 112–118.
36. Berwick DM. Patient safety: lessons from a novice. Adv Neonatal Care 2002; 2: 121–122.
37. Shojania KG, Wald H & Gross R. Understanding medical error and improving patient safety in the
inpatient setting. Med Clin North Am 2002; 86: 847–867.
38. Rall M, Manser T, Guggenberger H, et al. Patient safety and errors in medicine: development,
prevention and analyses of incidents. Anasthesiol Intensivmed Notfallmed Schmerzther 2001; 36:
321–330.
39. Gaba DM. Gaba: Safety first: ensuring quality care in the intensely productive environment—the HRO
model. APSF Newsletter 2003; 18 [www.apsf.org].
40. Dunn D. Incident reports—correcting processes and reducing errors. AORN J 2003; 78: 212 [see also
214–20, passim].
41. Takeda H, Matsumura Y, Nakajima K et al. Health care quality management by means
of an incident report system and an electronic patient record system. Int J Med Inf 2003; 69:
285–293.
42. Thomas AN, Pilkington CE & Greer R. Critical incident reporting in UK intensive care units: a postal
survey. J Eval Clin Pract 2003; 9: 59–68.
43. Dunn D. Incident reports—their purpose and scope. AORN J 2003; 46: 46–49.
44. Yong H & Kluger MT. Incident reporting in anaesthesia: a survey of practice in New Zealand. Anaesth
Intensive Care 2003; 31: 555–559.
45. Wu AW, Pronovost P & Morlock L. ICU incident reporting systems. J Crit Care 2002; 17: 86–94.
46. Kluger MT & Bullock MF. Recovery room incidents: a review of 419 reports from the Anaesthetic
Incident Monitoring Study (AIMS). Anaesthesia 2002; 57: 1060–1066.
47. Webster CS & Anderson DJ. A practical guide to the implementation of an effective incident reporting
scheme to reduce medication error on the hospital ward. Int J Nurs Pract 2002; 8: 176–183.
48. Wu AW, Pronovost P & Morlock L. ICU incident reporting systems. J Crit Care 2002; 17: 86–94.
49. Lawton R & Parker D. Barriers to incident reporting in a healthcare system. Qual Saf Health Care 2002; 11:
15–18.
50. Staender S. Incident reporting as a tool for error analysis in medicine. Z Arztl Fortbild Qualitatssich 2001;
95: 479–484.
51. Secker-Walker J & Taylor-Adams S. In Vincent C (ed.) Clinical Incident Reporting, Clinical Risk Management-
Enhancing Patient Safety, 2nd edn. London: BMJ Books, 2001, pp 419–438.
52. Sinclair M, Simmons S & Cyna A. Incidents in obstetric anaesthesia and analgesia: an analysis of 5000 AIMS
reports. Anaesth Intensive Care 1999; 27: 275–281.
53. Billings CE. Appendix B. Incident Reporting Systems in Medicine, and Experience with the Aviation Safety
Reporting System. Chicago: National Patient Safety Foundation; 1998.
54. Buckley TA, Short TG, Rowbottom YM & Oh TE. Critical incident reporting in the intensive care unit.
Anaesthesia 1997; 52: 403–409.
55. Beckmann U, Baldwin I, Hart GK & Runciman WB. The Australian incident monitoring study in intensive
care: AIMS-ICU. An analysis of the first year of reporting [see comments]. Anaesth Intensive Care 1996; 24:
320–329.
56. Williamson JA, Webb RK, Sellen A, et al. The Australian incident monitoring study. Human failure: an
analysis of 2000 incident reports. Anaesth Intensive Care 2000; 21: 678–683.
57. Runciman WB, Webb RK, Lee R & Holland R. System failure: an analysis of incident reports. Anaesth Intens
Care 2000; 21: 684–695.
58. Runciman WB, Webb RK, Lee R & Holland R. The Australian incident monitoring study. System failure: an
analysis of 2000 incident reports. Anaesth Intensive Care 2000; 21: 684–695.
59. Billings CE & Reynard WD. Human factors in aircraft incidents: results of a 7-year study. Aviat Space
Environ Med 1984; 55: 960–965.](https://image.slidesharecdn.com/crmevadpdieckmanbprca051-100910084556-phpapp01/75/Artigo-Safety-culture-and-crisis-resource-management-in-airway-management-17-2048.jpg)
![556 M. Rall and P. Dieckmann
60. Bagian JP, Gosbee J, Lee CZ, et al. The veterans affairs root cause analysis system in action. Jt Comm J Qual
Improv 2002; 28: 531–545.
61. Carroll JS, Rudolph JW & Hatakenaka S. Lessons learned from non-medical industries: root cause analysis
as culture change at a chemical plant. Qual Saf Health Care 2002; 11: 266–269.
62. Shinn JA. Root cause analysis: a method of addressing errors and patient risk. Prog Cardiovasc Nurs 2000;
15: 24–25.
63. Amo MF. Root cause analysis. A tool for understanding why accidents occur. Balance 1998; 2: 12–15.
64. Root Cause Analysis RCA VA NCPS. http://www.va.gov/ncps/rca.html. 2005.
65. Root Cause Analysis RCA Toolkit NPSA. http://www.npsa.nhs.uk/health/resources/root_cause_analysis/
conditions. 2005.
66. An introduction to FMEA. Using failure mode and effects analysis to meet JCAHO’s proactive risk
assessment requirement. Failure modes and effect analysis. Health Dev 2002; 31: 223–226.
67. Passey RD. Foresight begins with FMEA. Delivering accurate risk assessments. Med Device Technol 1999;
10: 88–92.
68. VA NCPS. Healthcare Failure Mode and Effect Analysis Course Materials (HFMEAe) 2005 [http://www.va.gov/
ncps/HFMEA.html].
69. Maurino DE, Reason J, Johnston N & Lee RB. Beyond Aviation Human Factors. Aldershot, England: Ashgate
Publishing Limited 1995.
70. Reason JT, Carthey J & de Leval MR. Diagnosing ‘vulnerable system syndrome’: an essential prerequisite
to effective risk management. Qual Health Care 2001; 10(supplement 2): ii21–ii25.
71. Reason J. Human error: models and management. Br Med J 2000; 320: 768–770.
72. Reason J. Managing the Risks of Organizational Accidents. Aldershot, England: Ashgate Publishing Limited
1997.
73. Sexton JB, Thomas EJ & Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross
sectional surveys. Br Med J 2000; 320: 745–749.
74. Howard SK, Rosekind MR, Katz JD & Berry AJ. Fatigue in anesthesia: implications and strategies for
patient and provider safety. Anesthesiology 2002; 97: 1281–1294.
75. Gaba DM & Howard SK. Patient safety: fatigue among clinicians and the safety of patients. N Engl J Med
2002; 347: 1249–1255.
76. Gaba DM, Singer SJ, Sinaiko AD, et al. Differences in safety climate between hospital personnel and naval
aviators. Hum Factors 2003; 45: 173–185.
77. Grissinger M & Rich D. JCAHO: Meeting the standards for patient safety. Joint Commission on
Accreditation of Healthcare Organizations. J Am Pharm Assoc (Wash.) 2002; 42: S54–S55.
78. Reason JT. Human Error. Cambridge: Cambridge University Press 1990.
79. Rosekind MR, Boyd JN, Gregory KB, et al. Alertness management in 24/7 settings: lessons from aviation.
Occup Med 2002; 17: 247–259.
80. Dismukes K. Cockpit interruptions and distractions. ASRS Directline 1998; 10(4–9): 4–9.
81. Helmreich RL. On error management: lessons from aviation. Br Med J 2000; 320: 781–785.
82. Helmreich RL & Merritt AC. Culture at Work in Aviation and Medicine. Aldershot, UK: Ashgate Publishing
Limited, 1998, pp 172–174.
83. Helmreich R. Managing threat and error (syllabus/powerpoint).
84. Degani A & Wiener EL. Procedures in complex systems: the airline cockpit. IEEE Trans Syst Man Cybern A
Syst Hum 1997; 27: 302–312.
85. Wiegmann DA & Shappell SA. A Human Error Approach to Aviation Accident Analysis. Burlington: Ashgate,
2003.
86. Reason J. Human error: models and management. Western J Med 2000; 172: 393–396.
87. Rasmussen J. Skills, rules, knowledge: signals, signs and symbols and other distinctions in human
performance models. IEEE Trans Sys Man Cyber 1983; SMC-13: 257–267.
88. Reason J. Managing the Risks of Organizational Accidents. Aldershot: Ashgate, 1997.
89. Perrow C. Normal Accidents. Princeton: Princeton University Press, 1999.
91. Wiener E, Kanki B & Helmreich R. Cockpit Resource Management. San Diego: Academic Press; 1993.
93. Reznek M, Smith-Coggins R, Howard S, et al. Emergency Medicine Crisis Resource Management
(EMCRM): Pilot Study of a Simulation-based Crisis Management Course for Emergency Medicine. Acad
Emerg Med 2003; 10: 386–389.](https://image.slidesharecdn.com/crmevadpdieckmanbprca051-100910084556-phpapp01/75/Artigo-Safety-culture-and-crisis-resource-management-in-airway-management-18-2048.jpg)


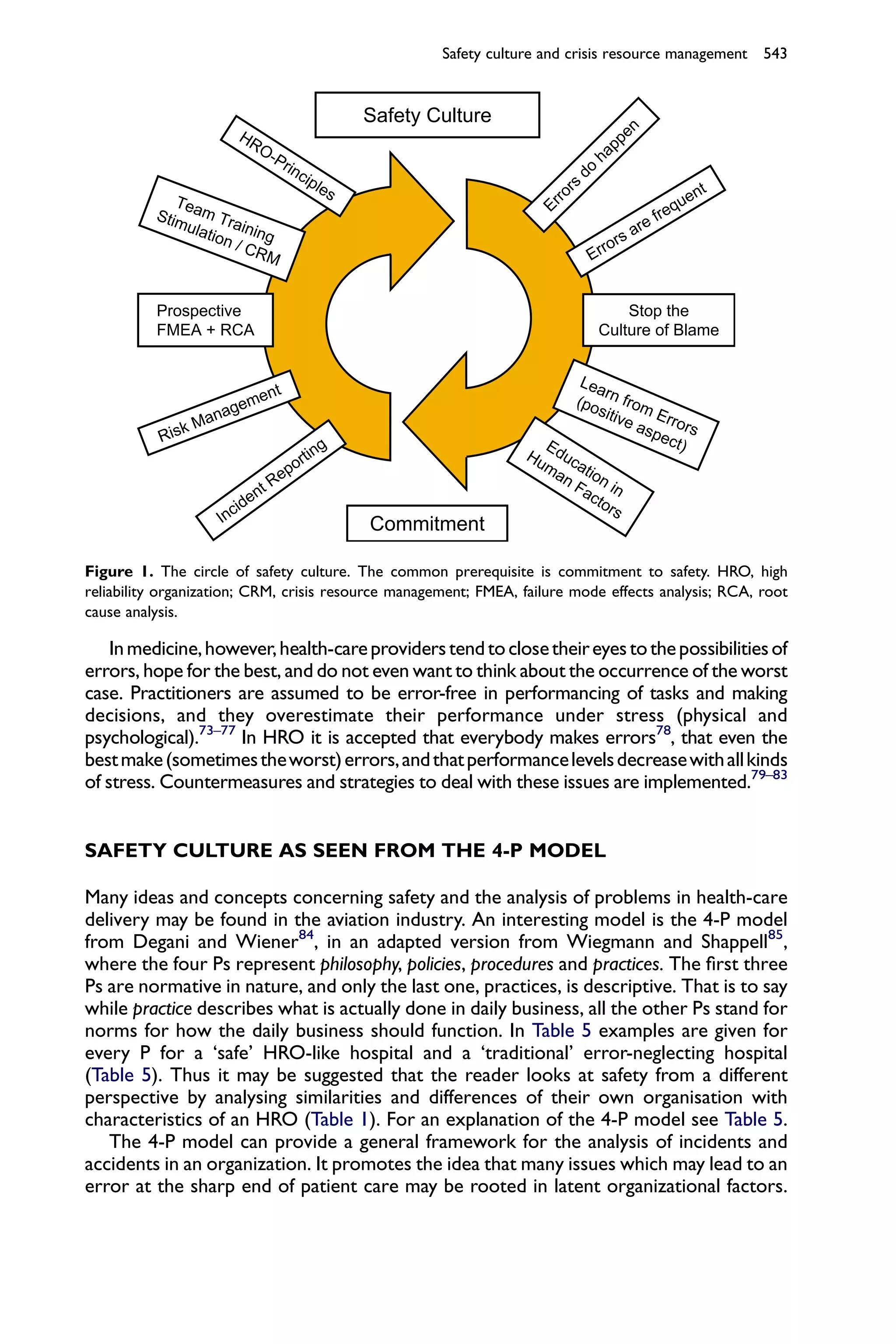
The document discusses the critical importance of airway management in anesthesiology and emergency care, emphasizing its role as a high-risk, high-reliability procedure essential for patient safety. It introduces concepts from high reliability organizations (HRO) and crisis resource management (CRM) to enhance safety culture, outlining strategies such as simulation training, incident reporting systems, and root cause analysis to prepare healthcare professionals for difficult airway situations. Ultimately, the authors argue for the adaptation of HRO principles in healthcare to minimize risks and promote a proactive safety culture.










































































