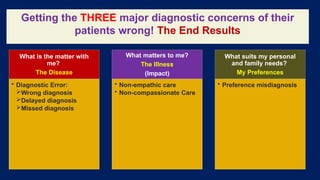
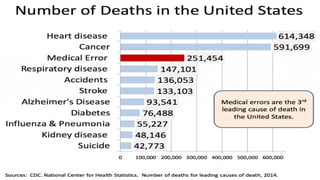
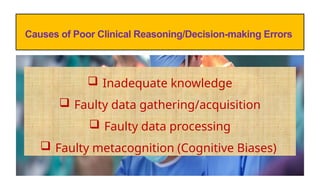
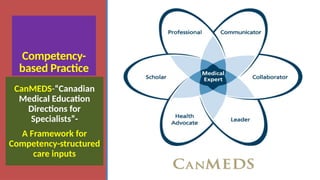
The document outlines advanced concepts in medical decision-making and critical thinking, emphasizing a competence-by-design approach to train healthcare professionals. It discusses the importance of integrating cognitive schemes, diagnostic routes, and patient-centered care in clinical practice. Additionally, it highlights the necessity for effective decision-making to enhance patient quality of care and avoid diagnostic errors.
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










