Critical Care Nursing
•As the specialty that manages human responses to
actual or potential life-threatening problems.
• Is the field of nursing with a focus on the utmost
care of the critically or unstable patients
following extensive injury, surgery or life-
threatening diseases.
• Or intensive care unit (ICU) nursing, is a specialty
focused on the care of unstable, chronically ill or
post-surgical patients and those at risk of life-
threatening diseases.
3.
Conceptual Foundation ofCritical
Care
FOCUS:
-Concepts of Critical Care
-Standards of Practice
-Competencies
4.
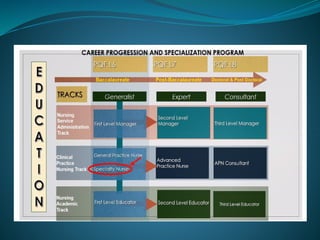
Concepts
Specialty Practice
Education
Competencies
Experience
Manage, Focus,Care,
Deals
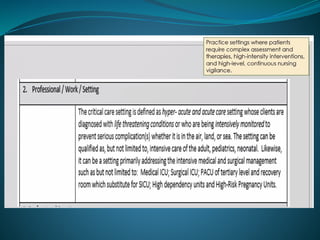
Practice settings where patients
require complex assessment,
high intensity interventions,
and high-level continuous
nursing vigilance
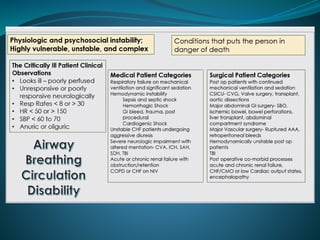
Human Responses
Physiologic and psychosocial
instability, highly vulnerable
unstable and complex
Life-threatening
problems
Conditions that puts the person
in danger of death
14.
COMPETENCIES FOR
CRITICAL CARENURSES
1. Safe and Quality Nursing Care
2. Management of Resources
3. Legal Responsibilities
4. Ethico-Moral Responsibilities
5. Collaboration and Teamwork
6. Personal and Professional Development
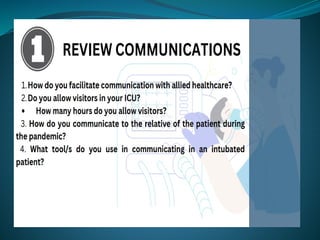
7. Communication
8. Health Education
9. Quality Improvement
10. Research
11. Record Management
Goals and Objectives
•Discuss the etiology and natural history
of common pediatric emergencies:
-Respiratory failure
-Shock
-Trauma
• Recognize the acuity and implement
appropriate emergency management
20.
What we learnedin PALS...
• Adult and pediatric etiologies of
cardiopulmonary arrest differ, a different
approach to assessment and intervention is
required in the pediatric population.
• Pediatric cardiopulmonary arrest results
when respiratory failure or shock is not
identified and treated in the early stages.
21.
Etiologies of
Cardiopulmonary Arrest
inChildren
• Bronchospasm, Burns, Congenital
cardiac abnormalities, Drowning,
Dysrhythmias, Foreign body aspiration,
Gastroenteritis, Seizures, Sepsis,
Trauma, Upper and lower respiratory
tract infection
• The etiologies of respiratory failure,
shock, cardiopulmonary arrest and
dysrhythmias in children differ from
22.
• Approximately 10percent of children who
progress to cardiopulmonary arrest are
successfully resuscitated.
• Children who only have respiratory arrest
have a 75 to 93 percent survival rate when
resuscitated.
• 92 percent of such children had no neurologic
impairment .
• Pediatric advanced life support begins with
early recognition and management of
respiratory failure and shock.
23.
How are kidsdifferent?
• Cardiac arrest is usually due to
progressive respiratory failure, shock or
both
• Once you have cardiac arrest---
Outcome is poor
-5-12% survive to discharge
-In-hospital not much better with
27% survival
History Taking
-Reason forseeking care
-Present illness
-Previous illness
-Family history
-Social history
Physical Examination
-Respiratory Assessment (I-P-P-A)
The Assessment
COUGH
Onset -sudden, gradual
Duration
Nature - dry, moist, hacking, barking
Sputum - amount, color, odor
Severity - disrupts activities?
Associated symptoms - sneezing, dyspnea, fever,
chills, congestion, gagging
What brings it on? - anxiety, talking, activity
What makes it better?
What has been tried? - medications, treatments
Anything similar in the past
66.
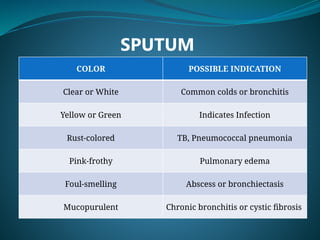
SPUTUM
COLOR POSSIBLE INDICATION
Clearor White Common colds or bronchitis
Yellow or Green Indicates Infection
Rust-colored TB, Pneumococcal pneumonia
Pink-frothy Pulmonary edema
Foul-smelling Abscess or bronchiectasis
Mucopurulent Chronic bronchitis or cystic fibrosis
67.
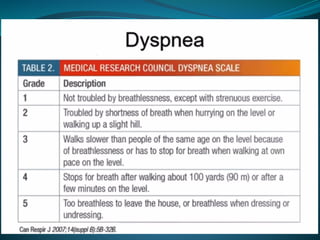
SHORTNESS OF BREATHOR DYSPNEA
Onset - sudden, gradual
Duration
Severity - disrupts activities
Associated symptoms - night sweats, pain, chest
pressure, discomfort, ankle edema, diaphoresis, cyanosis
What brings it on? - position, time of day, exercise,
allergens, emotions
What makes it better?
What has been tried? - medications, inhalers, oxygen
Anything similar in the past?
70.
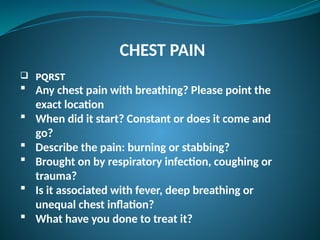
CHEST PAIN
PQRST
Any chest pain with breathing? Please point the
exact location
When did it start? Constant or does it come and
gо?
Describe the pain: burning or stabbing?
Brought on by respiratory infection, coughing or
trauma?
Is it associated with fever, deep breathing or
unequal chest inflation?
What have you done to treat it?
71.
History
Personal andSocial History
Tobacco
Alcohol
Drugs
Home, Occupation or Travel Environment
Health Promotional Activities
Wearing of mask, routine checks,
vaccination
72.
Additional History
Infantsand children
Frequency of cough and/or colds
History of allergy in the family
Child-proofing of home
Smokers in the home or in the car with child
Aging Adult
SOB on ADLs
Routine physical activities
Coping mechanisms (COPD, PTB, Lung Ca)
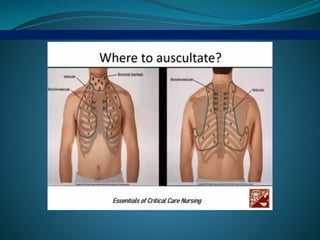
Anterior Thorax
Inspection
Appearance
-Symmetry, deformities
Posturing
Respiratory rate, effort and pattern
Skin, nails and lips color
Palpation
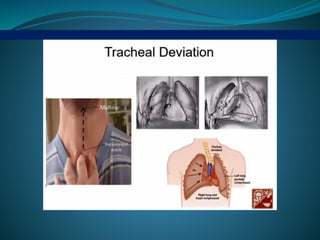
Tracheal position
Chest expansion
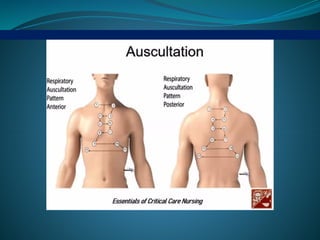
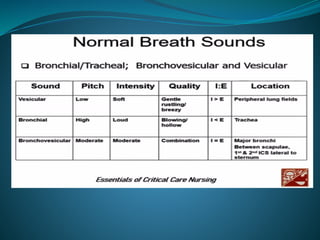
Auscultation
Duration, pitch and intensity of 1 & E sounds
in one breathing cycle
Normal and Adventitious Sounds
75.
Posterior Thorax
Inspection
Contour,symmetry and deformity, skin
Palpation
Areas of tenderness
Chest expansion
Tactile fremitus
Percussion - "ladder pattern"
Diaphragmatic Excursion
Auscultation
Duration, pitch and intensity of I & E sounds
in one breathing cycle
Normal and Adventitious Sounds
76.
Inspection
Altered rhythmsmay indicate underlying disorder:
Kussmaul's respirations - rapid, deep with sighing breaths,
occurs in patients with DKA
Cheyne-Stokes respirations - have a regular cycle of change
in the rate & depth of breathing; periods of deep breathing
alternating with periods of apnea
Biot's respirations (Ataxic) - unpredictable breaths
irregularity, rapid deep breaths that alternate it abrupt periods
of apnea
77.
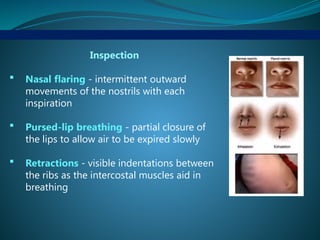
Inspection
Nasal flaring- intermittent outward
movements of the nostrils with each
inspiration
Pursed-lip breathing - partial closure of
the lips to allow air to be expired slowly
Retractions - visible indentations between
the ribs as the intercostal muscles aid in
breathing
78.
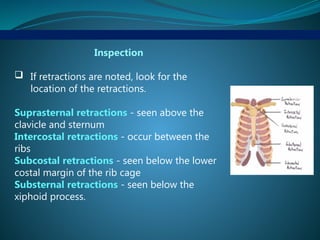
Inspection
If retractionsare noted, look for the
location of the retractions.
Suprasternal retractions - seen above the
clavicle and sternum
Intercostal retractions - occur between the
ribs
Subcostal retractions - seen below the lower
costal margin of the rib cage
Substernal retractions - seen below the
xiphoid process.
79.
Palpation
Trachea -slightly movable & quickly returns to
midline after displacement
Tactile fremitus - transmission of vibration of air
movement through chest wall during phonation
(99 method)
Chest Expansion - symmetry of chest movement
81.
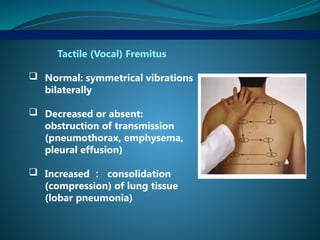
Tactile (Vocal) Fremitus
Normal: symmetrical vibrations
bilaterally
Decreased or absent:
obstruction of transmission
(pneumothorax, emphysema,
pleural effusion)
Increased : consolidation
(compression) of lung tissue
(lobar pneumonia)
82.
Assessment of ChestExpansion
Normal : bilateral,
symmetric expansion
Abnormal: unilateral or
unequal (atelectasis, lobar
pneumonia, pleural
effusion, pneumothorax)
83.
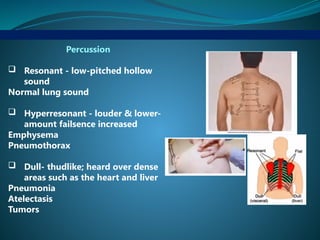
Percussion
Resonant -low-pitched hollow
sound
Normal lung sound
Hyperresonant - louder & lower-
amount failsence increased
Emphysema
Pneumothorax
Dull- thudlike; heard over dense
areas such as the heart and liver
Pneumonia
Atelectasis
Tumors
88.
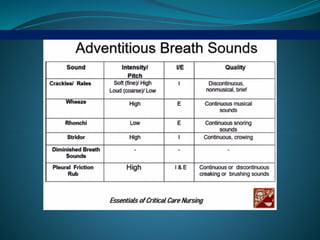
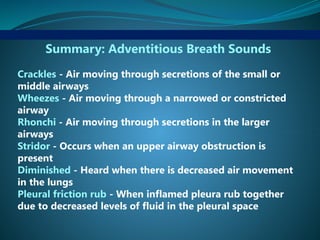
Summary: Adventitious BreathSounds
Crackles - Air moving through secretions of the small or
middle airways
Wheezes - Air moving through a narrowed or constricted
airway
Rhonchi - Air moving through secretions in the larger
airways
Stridor - Occurs when an upper airway obstruction is
present
Diminished - Heard when there is decreased air movement
in the lungs
Pleural friction rub - When inflamed pleura rub together
due to decreased levels of fluid in the pleural space
89.
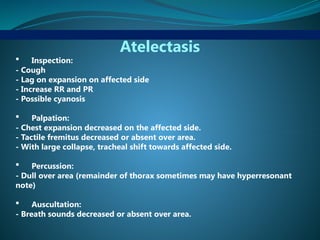
Atelectasis
Inspection:
- Cough
-Lag on expansion on affected side
- Increase RR and PR
- Possible cyanosis
Palpation:
- Chest expansion decreased on the affected side.
- Tactile fremitus decreased or absent over area.
- With large collapse, tracheal shift towards affected side.
Percussion:
- Dull over area (remainder of thorax sometimes may have hyperresonant
note)
Auscultation:
- Breath sounds decreased or absent over area.
90.
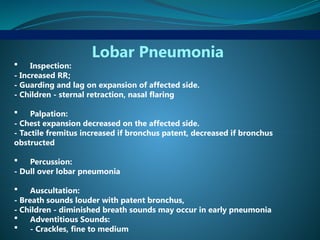
Lobar Pneumonia
Inspection:
-Increased RR;
- Guarding and lag on expansion of affected side.
- Children - sternal retraction, nasal flaring
Palpation:
- Chest expansion decreased on the affected side.
- Tactile fremitus increased if bronchus patent, decreased if bronchus
obstructed
Percussion:
- Dull over lobar pneumonia
Auscultation:
- Breath sounds louder with patent bronchus,
- Children - diminished breath sounds may occur in early pneumonia
Adventitious Sounds:
- Crackles, fine to medium
91.
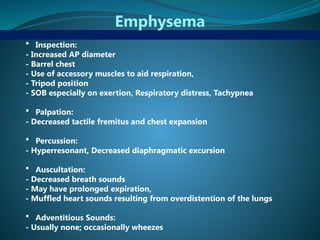
Emphysema
Inspection:
- IncreasedAP diameter
- Barrel chest
- Use of accessory muscles to aid respiration,
- Tripod position
- SOB especially on exertion, Respiratory distress, Tachypnea
Palpation:
- Decreased tactile fremitus and chest expansion
Percussion:
- Hyperresonant, Decreased diaphragmatic excursion
Auscultation:
- Decreased breath sounds
- May have prolonged expiration,
- Muffled heart sounds resulting from overdistention of the lungs
Adventitious Sounds:
- Usually none; occasionally wheezes
92.
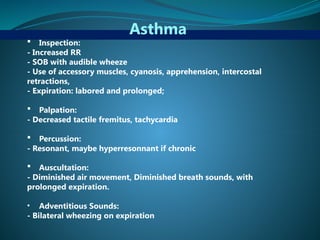
Asthma
Inspection:
- IncreasedRR
- SOB with audible wheeze
- Use of accessory muscles, cyanosis, apprehension, intercostal
retractions,
- Expiration: labored and prolonged;
Palpation:
- Decreased tactile fremitus, tachycardia
Percussion:
- Resonant, maybe hyperresonnant if chronic
Auscultation:
- Diminished air movement, Diminished breath sounds, with
prolonged expiration.
• Adventitious Sounds:
- Bilateral wheezing on expiration
93.
Pleural Effusion (Fluid)or Thickening
Inspection:
- Increased respirations, dyspnea;
- may have dry cough, tachycardia, cyanosis and abdominal distention
Palpation:
- Tactile fremitus decreased or absent;
- Tracheal shift away from affected side.
- Chest expansion decreased on affected side.
Percussion:
- Dull to flat. No diaphragmatic excursion on affected side
Auscultation:
- Breath sounds decreased or absent; When remainder of the lung is
compressed near the effusion, may have bronchial breath sounds over the
compression
Adventitious Sounds:
- None
94.
Pneumothorax
Inspection:
- Unequalchest expansion,
- If large, tachypnea, cyanosis, apprehension, bulging in interspaces
Palpation:
- Tactile fremitus decreased or absent.
- Tracheal shift to opposite side (unaffected side).
- Chest expansion decreased on affected side, Tachycardia,
decreased BP
Percussion:
- Hyperresonnant. Decreased diaphragmatic excursion
Auscultation:
- Breath sounds decreased or absent
Adventitious Sounds:
- None
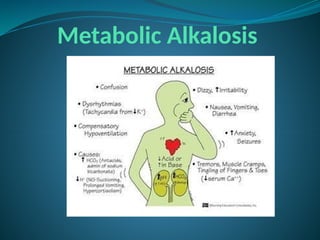
Steps in ABGInterpretation
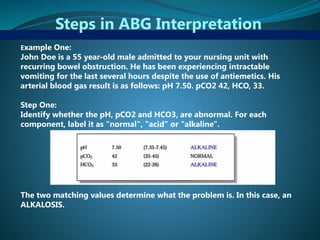
Example One:
John Doe is a 55 year-old male admitted to your nursing unit with
recurring bowel obstruction. He has been experiencing intractable
vomiting for the last several hours despite the use of antiemetics. His
arterial blood gas result is as follows: pH 7.50. pCO2 42, HCO, 33.
Step One:
Identify whether the pH, pCO2 and HCO3, are abnormal. For each
component, label it as "normal", "acid" or "alkaline".
The two matching values determine what the problem is. In this case, an
ALKALOSIS.
100.
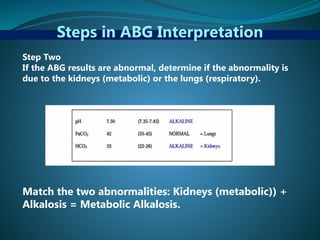
Steps in ABGInterpretation
Step Two
If the ABG results are abnormal, determine if the abnormality is
due to the kidneys (metabolic) or the lungs (respiratory).
Match the two abnormalities: Kidneys (metabolic)) +
Alkalosis = Metabolic Alkalosis.
101.
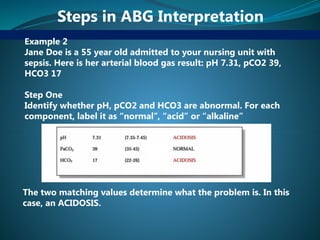
Steps in ABGInterpretation
Example 2
Jane Doe is a 55 year old admitted to your nursing unit with
sepsis. Here is her arterial blood gas result: pH 7.31, pCO2 39,
HCO3 17
Step One
Identify whether pH, pCO2 and HCO3 are abnormal. For each
component, label it as “normal”, “acid” or “alkaline”
The two matching values determine what the problem is. In this
case, an ACIDOSIS.
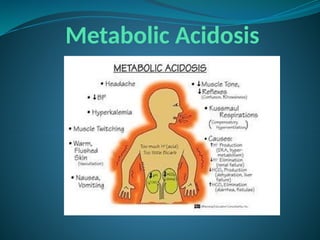
102.
Steps in ABGInterpretation
Step Two
If the ABG results are abnormal, determine if the abnormality is
due to the kidneys (metabolic) or the lungs (respiratory).
Match the two abnormalities: Kidneys (metabolic) + Acidosis =
Metabolic Acidosis.
Physical Assessment of
theCardiovascular System
Techniques
• Inspection
• Palpation
• Percussion
• Auscultation
109.
Specific Areas ofthe
Cardiovascular Assessment
• Inspection of the face and lips
• Inspection of the jugular veins
• Inspection of the carotid arteries
• Inspection of the hands and fingers
• Inspection of the chest, abdomen, legs and
skeletal structures
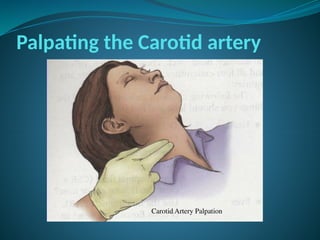
Palpating the Carotidartery
• Keep the patient’s head elevated at 30°
• Place your middle and index fingers on the
right then left carotid arteries, and palpate the
carotid upstroke
• NEVER palpate right and left carotid arteries
simultaneously
112.
Percussion
• More often,it is used as part of clinical
evaluation of the lungs and abdomen.
• Percussion of the heart can be useful in
estimating a patient’s heart size and/or
pericardial effusion.
113.
Auscultation
• Listen inall 5 listening areas of the heart for S1
and S2 using the diaphragm of the stethoscope
• Then listen at the apex with the bell
• The diaphragm is best for detecting high-pitched
sounds like S1, S2 and also S4 and most murmurs
• The bell is best for detecting low-pitched sounds
like S3 and the rumble of mitral stenosis.
• Erb’s point is the auscultation location for heart
sounds and heart murmurs located at the third
intercoastal space and the left lower sternal
boarder
Myocardial Infarction
• Alsoknown as Heart Attack
• Newest term: Acute Coronary Syndrome
• Leading cause of death in many countries
• Reduced blood flow through one of the
coronaries in myocardial ischemia and
necrosis
• Usually affects the LV – “workhorse” of the
heart
• Good collateral circulation limits the size of an
MI
117.
Myocardial Infarction
• Deathusually results from cardiac damage or
complications
• Mortality is high when treatment is delayed
• Almost half of sudden death from MI occur
before hospitalization, within 1hr of the onset
of symptoms.
• Prognosis improves if vigorous treatment
begins immediately
• Early recognition and aggressive treatment is
vital
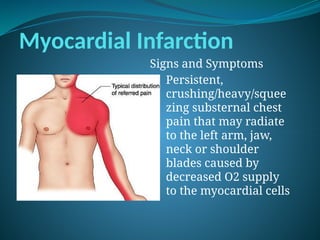
Myocardial Infarction
Signs andSymptoms
• Persistent,
crushing/heavy/squee
zing substernal chest
pain that may radiate
to the left arm, jaw,
neck or shoulder
blades caused by
decreased O2 supply
to the myocardial cells
120.
Myocardial Infarction
Signs andSymptoms
• Cool extremities, perspiration, anxiety and
restlessness
• BP and HR initially elevated
• Decreased UO
• Fatigue and weakness
• SOB and crackles – reflects Heart Failure
• Bradycardia
121.
Myocardial Infarction
Diagnosis
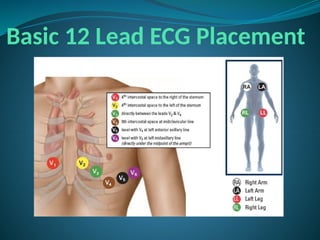
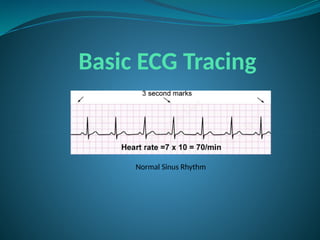
• Serial12 lead ECG
• Serial cardiac enzymes – serum cardiac
markers
myoglobin, CK-MB, Trop.I, Trop. T
• Echocardiography
• Coronary angiography
122.
Myocardial Infarction
TREATMENT
• Thrombolytictherapy
most effective within the first 3hours after onset of symptoms
• Heparin
• Limitation of physical activities
• M = Morphine or Meperidine
• O = Oxygen
• N = Nitrates (do not give for SBP<90, HR<50
• A = Aspirin
• Coronary Angioplasty
• Bypass (CABG)
123.
Myocardial Infarction
NURSING CARE
•Establish an IV line
• VS and Cardiac Monitoring
• NPO except sips of water until stable
• Diet: Low salt, low fat
• Complete bed rest without bathroom
privileges
• Oxygen: 2-3lpm via nasal cannula
• Stool softener as prescribed
124.
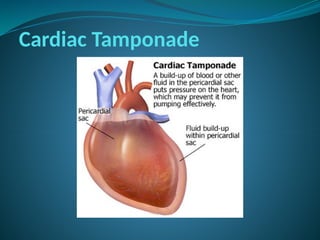
Cardiac Tamponade
• Arapid, unchecked increase in pressure in the
pericardial sac that compresses the heart
impairs diastolic filling and reduce cardiac
output
• Usually results from blood or fluid
accumulating in the pericardial sac
• Rapid collection of fluid in the pericardial sac
interferes with ventricular filling and
pumping, critically reducing cardiac output.
• Considered a medical emergency – therefore,
must be aggressively treated to preserve life
Cardiac Tamponade
CAUSES
• Idiopathic
•Effusion – from CA, Bacterial infxn, TB, RH
fever
• Hemorrhage – from traumatic causes
• Hemorrhage – from non-traumatic causes e.g
anticoagulant therapy
• Viral or post radiation pericarditis
• Chronic renal failure requiring dialysis
• Connective tissue disorder
• AMI
127.
Cardiac Tamponade
Signs andSymptoms
• Elevated CVP with jugular vein distention
• Muffled heart sounds
• Diaphoresis and cool, clammy skin
• Anxiety, restlessness and syncope
• Cyanosis
• Weak, rapid pulses
• Cough, dyspnea, orthopnea
• Pulsus Parodoxus – classic manifestation of
cardiac tamponade
- A decrease in SBP>15 during
inspiration
128.
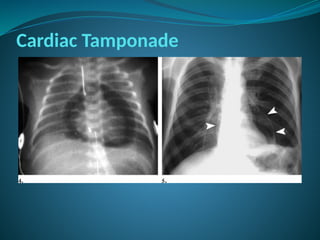
Cardiac Tamponade
DIAGNOSIS
• CXR
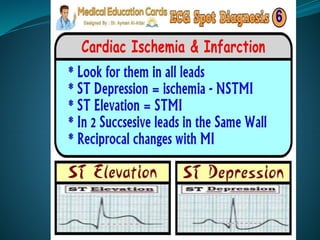
•ECG – may show a low amplitude QRS
complex and generalized ST segment
elevation is noted in all leads
• PA Catheterization
• Echocardiography
Cardiac Tamponade
NURSING CARE
•Collaborative management
• Report significant changes or trends in
hemodynamic parameters and dysrrhythmias.
• Maintain atleast 1 patient IV access site
• Prepare for emergency pericardiocentesis
and/or emergency surgery as necessary.
• Support client towards independence
131.
Cardiac Tamponade
TREATMENT
• Supplementalo2
• Continuous ECG and hemodynamic monitoring
• Trial volume loading crystalloids – to maintain SBP
• Inotropic drugs
• NSAIDS
• Pericardial window – surgical creation of opening
• Pericardiocentesis – needle aspiration
• Administration of heparin antagonist (Protamine)
-to stop bleeding in heparin-induced tamponade
• Use of Vit.K in warfarin-induced tamponade
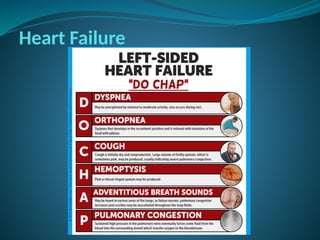
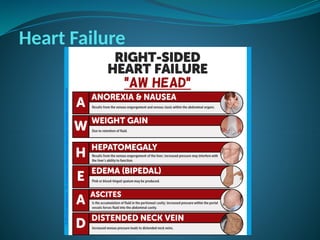
Heart Failure
PATIENT TEACHING
•Avoid foods high in Na+ to curb fluid overload
• Replace K+ loss through diuretics
• Weigh patient daily and record
• Stress the importance of taking meds as
prescribed
• Instruct patient to check his own pulse and
report if <60bpm
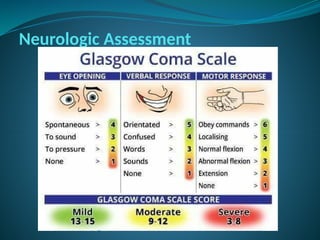
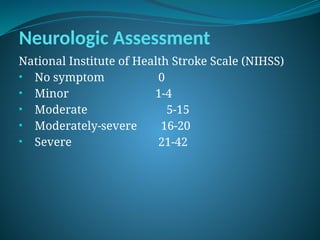
Neurologic Assessment
NIHSS 11categories
• Level of consciousness
Orientation
Commands
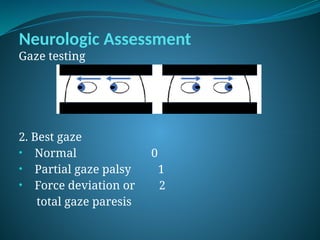
• Best Gaze
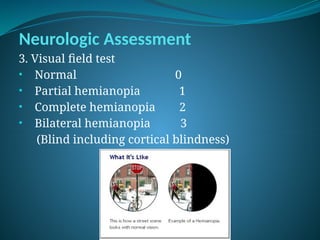
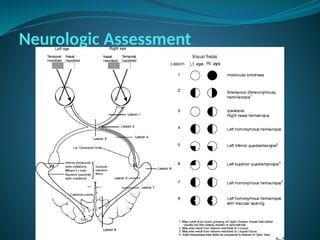
• Visual fields
• Facial palsy
• Motors (R&L) – Arms and Legs
• Limb ataxia
• Sensation
• Best language
• Dysarthria
• Extinction and inattention
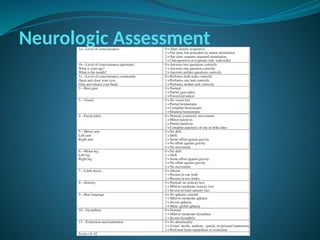
188.
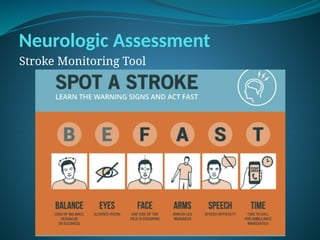
Neurologic Assessment
1A. Levelof consciousness (LOC)
• Alert 0
• Arousable by minor stimulation 1
• Not alert, requires repeated 2
stimulation; Obtunded
• Unresponsive 3
189.
Neurologic Assessment
1B. LOCquestions
• Answers both correctly 0
• Answers one correctly 1
• Both incorrect 2
• Standard questions
• A. What month is it today?
• B. How old are you?
190.
Neurologic Assessment
1C. LOCCommands
• Obeys both correctly 0
• Obeys one correctly 1
• Both incorrect 2
• Standard Commands
• A. Can you open and close your eyes?
• B. Can you make a fist?
Neurologic Assessment
4. Facialpalsy
• Normal 0
• Minor paralysis 1
• Partial paralysis 2
• Complete paralysis 3
• Observe for nasolabial fold
195.
Neurologic Assessment
5A and5B Motor (Arm)
• Normal 0
• Drifts before 10secs 1
• Falls before 10 seconds 2
• No effort against gravity 3
• No movement 4
196.
Neurologic Assessment
6A and6B Motor (Leg)
• Normal 0
• Drifts before 10secs 1
• Falls before 10 seconds 2
• No effort against gravity 3
• No movement 4
Neurologic Assessment
7. Limbataxia
• No ataxia 0
• Present in one limb 1
• Present in two limbs 2
• Using:
• Arms: finger to nose test
• Legs: heel to shin test
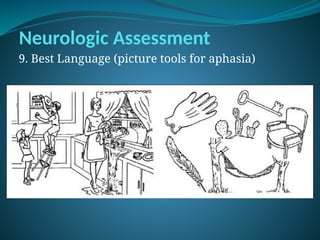
Neurologic Assessment
9. BestLanguage
• Normal 0
• Mild to moderate aphasia 1
• Severe aphasia 2
• Mute, global aphasia 3
• Ask the patient to name items on the picture
tools.
Neurologic Assessment
11. Extinctionand Inattention
• Normal 1
• Visual, tactile, auditory or 2
personal inattention
• Profound hemi-attention or 3
extinction to more than one modality
Neurologic Assessment
Stroke- TreatmentPathway
1. Rapid patient recognition and reaction to stroke
warning signs
2. Rapid emergency medical services (EMS)
dispatch
3. Rapid EMS system transport and hospital pre-
notification
4. Delivery direct to imaging
5. Rapid in-hospital diagnosis and treatment
*Effective EMS system can minimize delays in pre-
hospital dispatch, assessment and transport & increase
the number of patients reaching hospital and receiving
thrombolytic therapy w/in the approved time window.
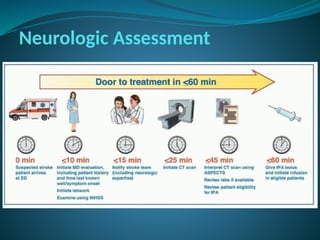
Neurologic Assessment
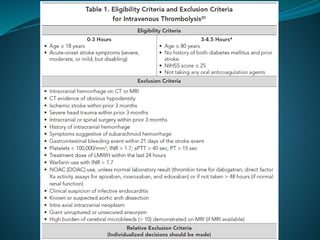
Intravenous Thrombolysis(rTpa)
- Is a treatment to dissolve dangerous clots to
improve blood flow and prevent damage to
tissue and organs
- May involve the injection of clot-busting drugs
through an IV line or through a long catheter
that delivers drug directly to the site of blockage.
- It also involves the use of long catheter with
mechanical device attached to the tip that either
removes the clot or physically breaks it up.
- It is given to patients with ischemic stroke,
arrived at the ER within the Golden period from
the onset of stroke (3 to 4.5 hours).
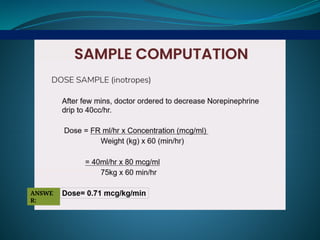
209.
Neurologic Assessment
Computation forrTpa
*obtain weight of patient in kilograms
Dose = 0.9mg/kg (not to exceed 90mg)
*initial 10% given as iv bolus for 1 minute
*remaining 90% as infusion drip over 60minutes