CORNEAL ULCERS
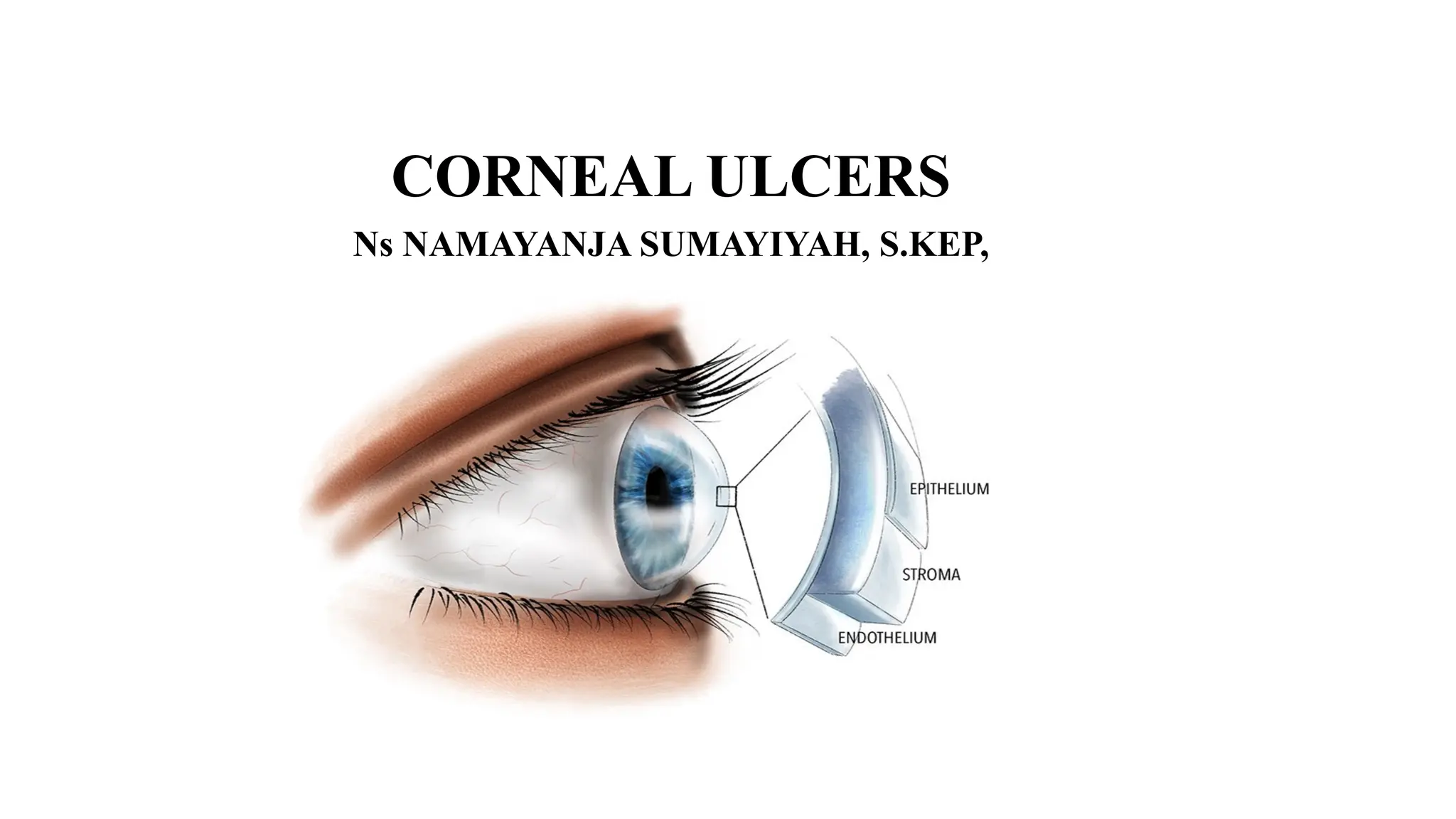
• Cornealulcers are open sores or epithelial defects with underlying inflammation
on the cornea, the transparent front part of the eye that covers the iris and pupil.
• These ulcers are often visible as grey to white opaque or translucent areas on the
normally clear cornea. In some cases, they may be too small to detect without
adequate magnification.
3.
CORNEAL ULCER
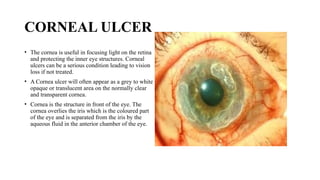
• Thecornea is useful in focusing light on the retina
and protecting the inner eye structures. Corneal
ulcers can be a serious condition leading to vision
loss if not treated.
• A Cornea ulcer will often appear as a grey to white
opaque or translucent area on the normally clear
and transparent cornea.
• Cornea is the structure in front of the eye. The
cornea overlies the iris which is the coloured part
of the eye and is separated from the iris by the
aqueous fluid in the anterior chamber of the eye.
4.
CAUSES OF CORNEALULCERS
Infections:
•Bacterial Infections: Commonly caused by bacteria like Staphylococcus and Pseudomonas. These
bacteria can invade the cornea, especially if the surface is disrupted. Contact lens wearers are
particularly at risk, especially with improper hygiene or prolonged wear.
•Viral Infections: Herpes simplex virus (responsible for cold sores) and varicella-zoster virus
(causing chickenpox and shingles) can lead to corneal ulcers. These viruses can cause recurrent
infections, leading to chronic corneal ulceration.
•Fungal Infections: These occur mainly due to improper contact lens care or prolonged use of
corticosteroid eye drops. Fusarium and Candida species are common culprits.
5.
CAUSES OF CORNEALULCERS
• Trauma
Mechanical : tiny cuts or piercings
Chemical: acids or strong alkalis
•Pre-existing Eye Conditions:
Dry Eye Syndromes: Conditions like keratoconjunctivitis sicca reduce the protective tear film,
making the cornea more susceptible to injury and infection.
•Eyelid Disorders: Conditions that prevent the eyelid from closing completely, such as Bell's palsy,
can leave the cornea exposed and prone to ulceration. Entropion (inward-turning eyelid) and
trichlasis (ingrown eyelashes) can cause constant irritation and lead to ulcer formation
6.
CAUSES OF CORNEALULCERS
•Immunological Disorders:
Autoimmune Diseases: Conditions like rheumatoid arthritis and lupus can predispose individuals to
corneal ulcers, either through direct inflammation or secondary infection. Immune-mediated
conditions like scleritis can also contribute to ulcer formation.
7.
CLINICAL MANIFESTATIONS
•Redness: Theconjunctiva and the anterior chamber may appear red due to dilated blood vessels.
•Eye Pain: Ranges from mild to severe, often worsening with bright light exposure (photophobia).
•Hypopyon
•Visual Disturbance: Blurred vision, especially if the ulcer is centrally located.
•Tearing and Discharge: Excessive tearing, pus, or thick discharge from the affected eye.
•Foreign Body Sensation: A constant feeling that something is in the eye.
•Swelling: The eyelids may be swollen, and there may be noticeable edema around the ulcer.
INVESTIGATIONS
•Slit Lamp Examination:A slit lamp microscope is used to examine the
•eye in detail. A fluorescein dye is often applied to highlight the ulcer, making it more visible under
blue light.
•Microbial Cultures: Swabs or scrapings from the ulcer are sent for microscopy, culture, and
sensitivity testing to identify the causative organism and guide treatment.
•Corneal Sensitivity Test: This assesses the sensitivity of the cornea, which may be reduced in cases
of viral ulcers or chronic conditions.
10.
MANAGEMENT
Medical Treatment:
•Anti-Infective Agents:Antibiotic, antiviral, or antifungal eye drops/ointments are used depending
on the cause. For viral ulcers, oral antiviral medications may also be prescribed.
•Cycloplegics: These are eye drops like cyclopentolate or atropine, used to dilate the pupil and
relieve pain from ciliary muscle spasms.
11.
MANAGEMENT
Surgical Management:
•Eyelash Removal:If an ingrown eyelash is causing the ulcer, it may be removed
along with its root. Recurrent cases may require electrolysis to destroy the hair
follicle.
•Eyelid Surgery: In cases where an inward-turning eyelid (entropion) is causing the
ulcer, corrective surgery may be necessary.
•Corneal Transplant (Keratoplasty): If the ulcer causes significant thinning of the
cornea, a corneal transplant may be required to restore the integrity of the eye.
12.
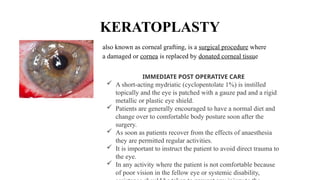
KERATOPLASTY
also known ascorneal grafting, is a surgical procedure where
a damaged or cornea is replaced by donated corneal tissue
IMMEDIATE POST OPERATIVE CARE
A short-acting mydriatic (cyclopentolate 1%) is instilled
topically and the eye is patched with a gauze pad and a rigid
metallic or plastic eye shield.
Patients are generally encouraged to have a normal diet and
change over to comfort
able body posture soon after the
surgery.
As soon as patients recover from the effects of anaesthesia
they are permitted regular activities.
It is important to instruct the patient to avoid direct trauma to
the eye.
In any activity where the patient is not comfortable because
of poor vision in the fellow eye or systemic disability,
13.
KERATOPLASTY
Post operative care
•Many patients may request for a mild analgesic on the first day. Stronger
medications are almost never needed, and the need for them should alert the
surgeon to the presence of possible complications.
• In the eyes suspected to have postoperative rise of intraocular pressure (IOP)
including when viscoe
lastic substances such as sodium hyaluronate have been left
in the anterior chamber during surgery, systemic oral acetazolamide 250 mg is
administered.
• There is no routine need for systemic antibiotics after the corneal transplant.
14.
KERATOPLASTY
Follow up care
Itis mandatory to evaluate the eye on slit-lamp for wound integrity, epithelial
defects, corneal oedema, IOP, iritis, and the possibility of infection on the first
postoperative day.
If any of these complications manifest or persist, evaluation of the operated eye
should be continued on a daily basis for a few more days.
As soon as the condition becomes normal, further evaluation may be at the end
of a week followed by every two weeks for one month and then every month for
the first year.
In the absence of any complications, scheduled evaluations at increasing
intervals of once or twice a year are adequate.
15.
CORNEAL ULCERS
Preventative measures
EyeProtection: Always wear protective eyewear when working with tools,
chemicals, or in environments with flying debris.
Proper Contact Lens Care: Wash hands before handling lenses,
avoid using saliva to wet lenses, never use tap water for cleaning, and do not
wear lenses overnight unless they are specifically designed for extended wear.
Lubrication: Individuals with dry eyes or incomplete eyelid closure should use
artificial tears to keep the cornea moist.
Eye Protection: Always wear protective eyewear when working with tools,
chemicals, or in environments with flying debris.
Proper Contact Lens Care: Wash hands before handling lenses,
avoid using saliva to wet lenses, never use tap water for cleaning, and do not
wear lenses overnight unless they are specifically designed for extended wear.
Lubrication: Individuals with dry eyes or incomplete eyelid closure should use
artificial tears to keep the cornea moist.
16.
CORNEAL ULCERS
Complications
• CornealScarring: A healed ulcer may leave a scar, leading to permanent visual impairment if the
scar is centrally located.
• Secondary Infections: An untreated ulcer can lead to secondary infections, worsening the
prognosis.
• Corneal Perforation: in severe cases, the ulcer may perforate the cornea, potentially leading to loss
of the eye.
• Endophthalmitis: This is a severe infection of the interior of the eye, which can result from
untreated corneal ulcers.
• Blindness: If not treated adequately, corneal ulcers can lead to significant vision loss or complete
blindness.