Download to read offline

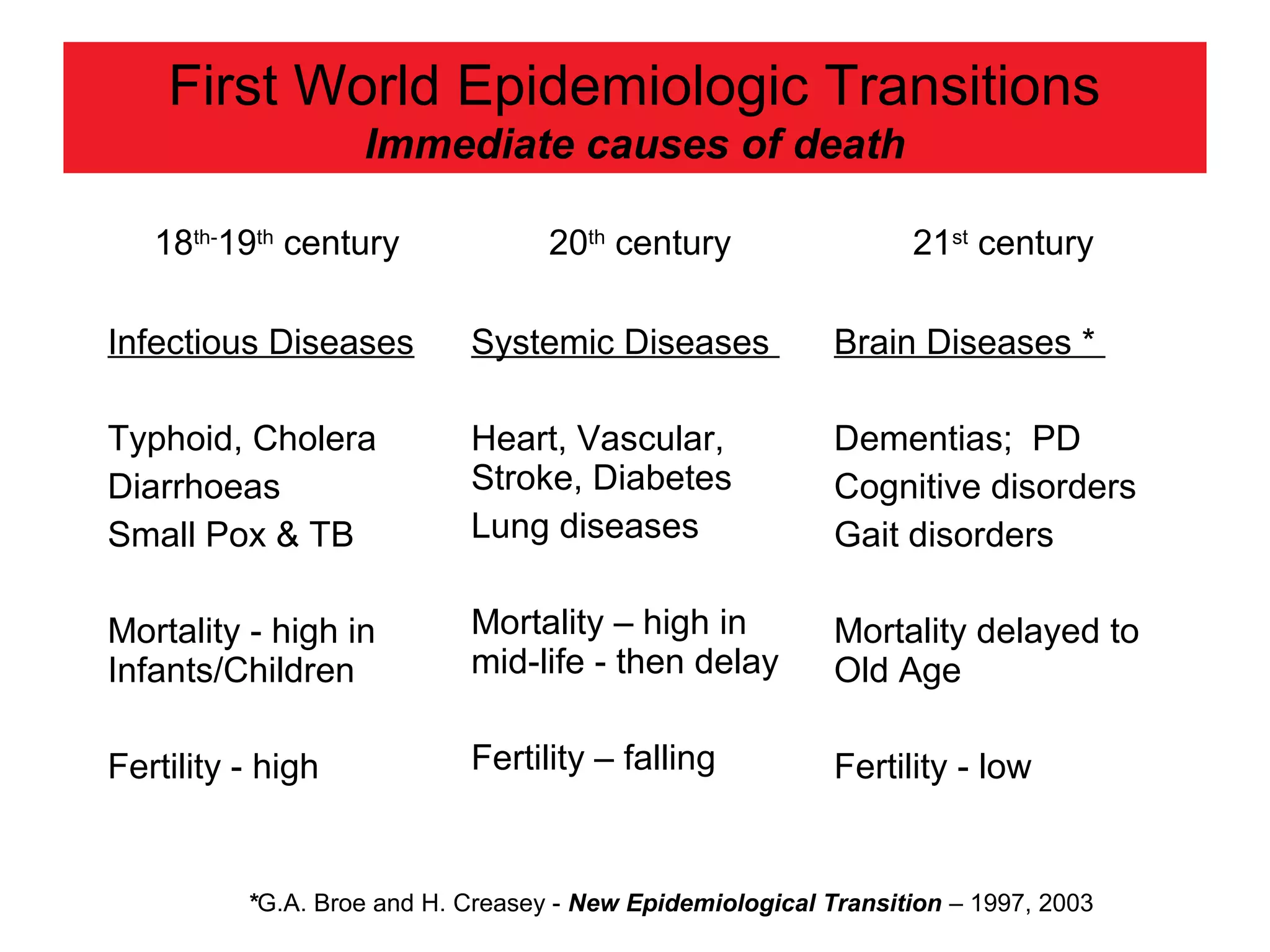
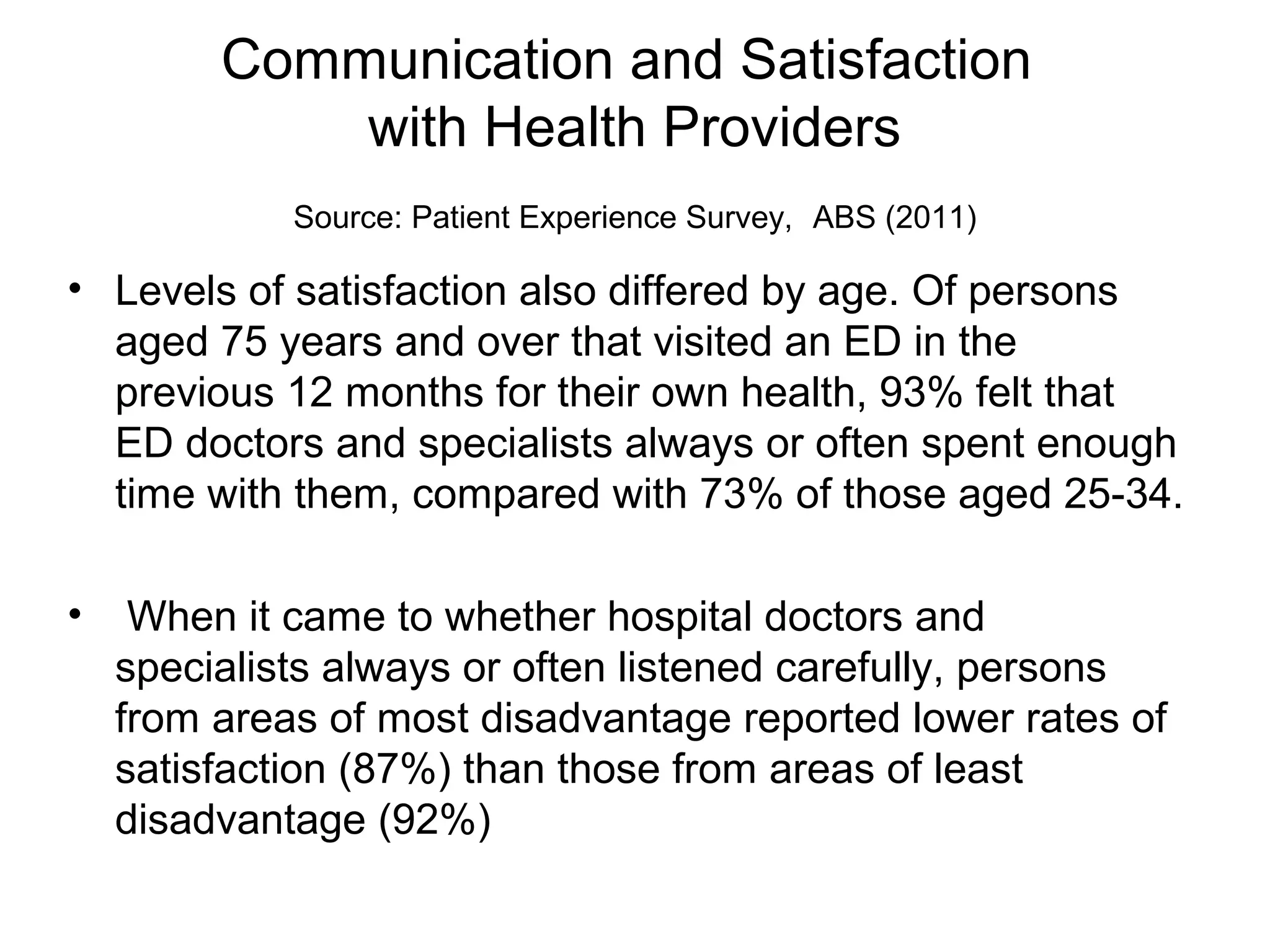
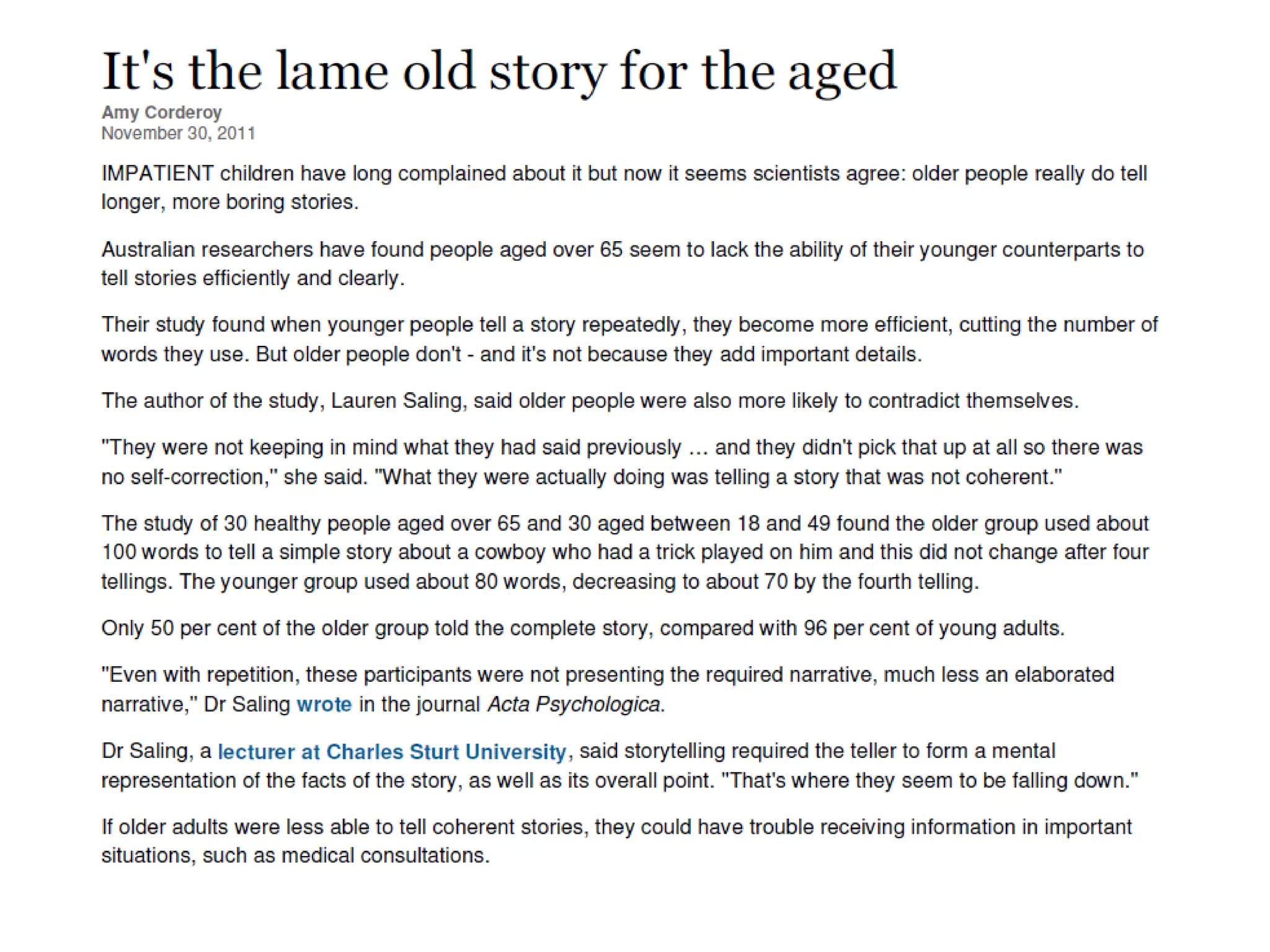
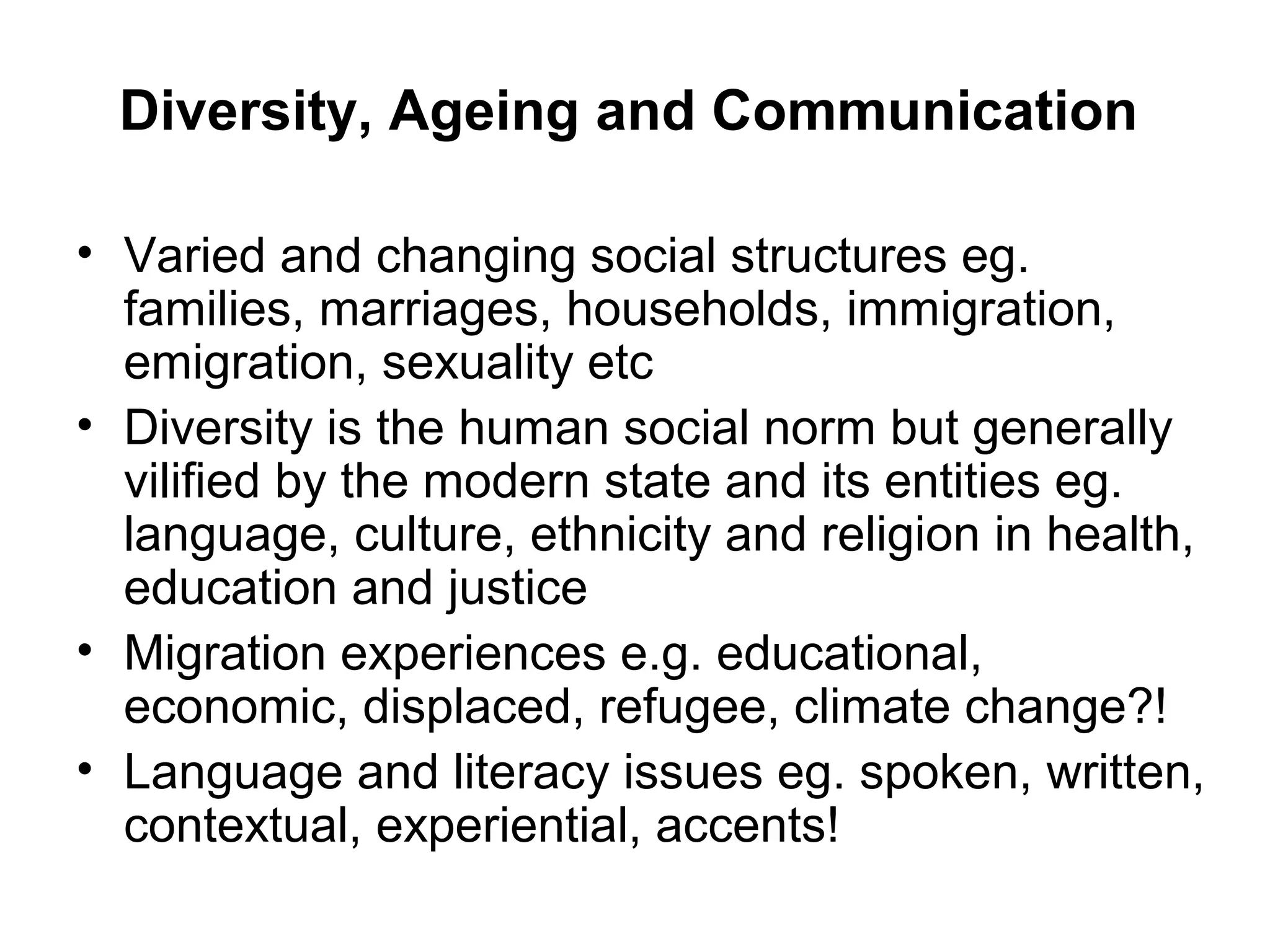
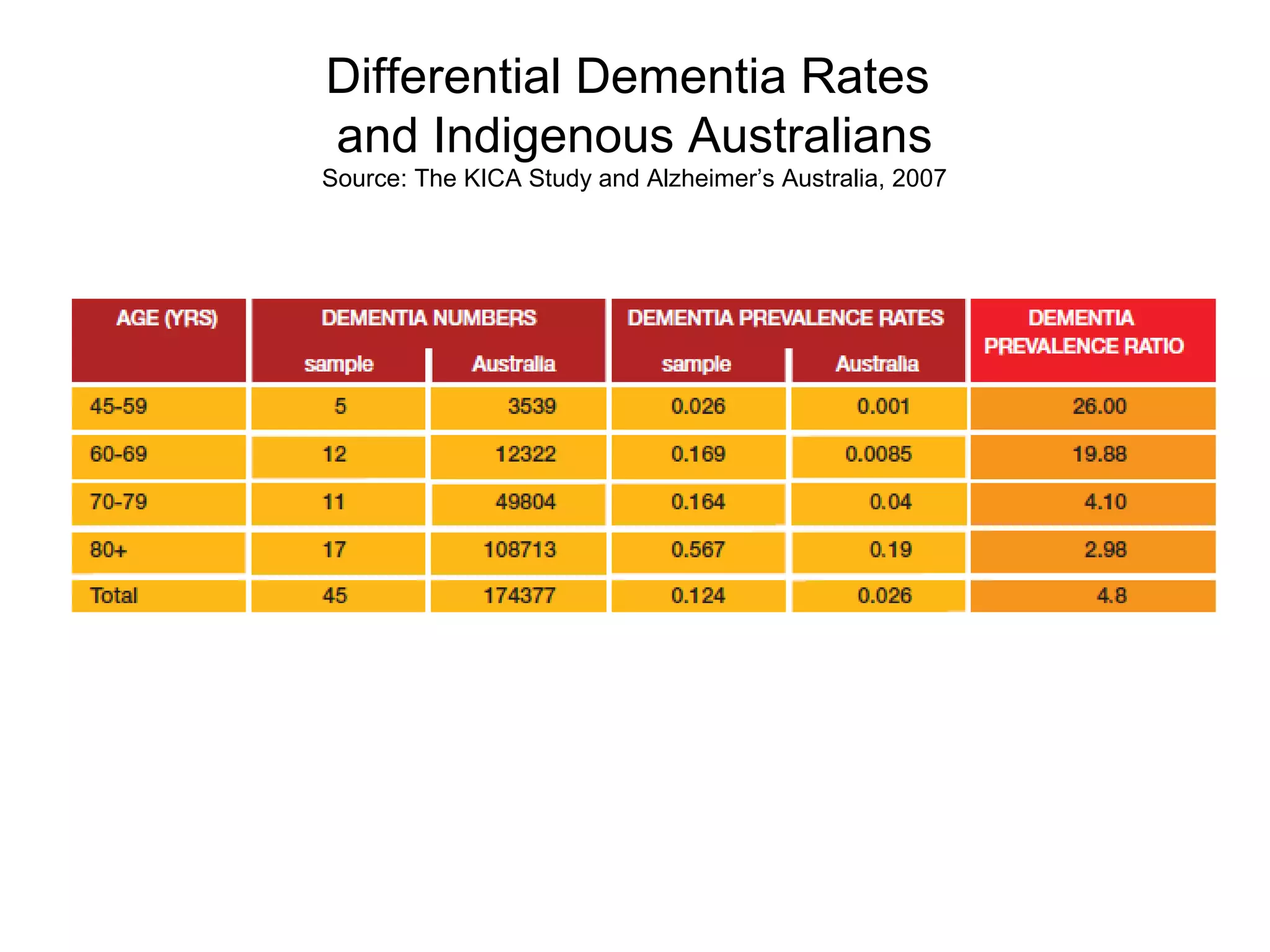

The document discusses the implications of an ageing population on communication practices in society, with a focus on the Asia-Pacific region. It highlights the rising prevalence of dementia and other neurodegenerative diseases, the challenges of communicating effectively with older adults, and the need for healthcare professionals to adapt to diverse patient needs. Ethical communication issues in healthcare and the impact of social diversity on ageing populations are emphasized as critical areas for improvement.











![Frail elderly [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/frailelderlycompatibilitymode-180419115003-thumbnail.jpg?width=640&height=640&fit=bounds)



































![Syllabus [Gerontology (GTY-154 A) - Aging in American Society]](https://cdn.slidesharecdn.com/ss_thumbnails/ef83b54f-b791-424c-8179-cbfdc332476d-160415174142-thumbnail.jpg?width=640&height=640&fit=bounds)














































