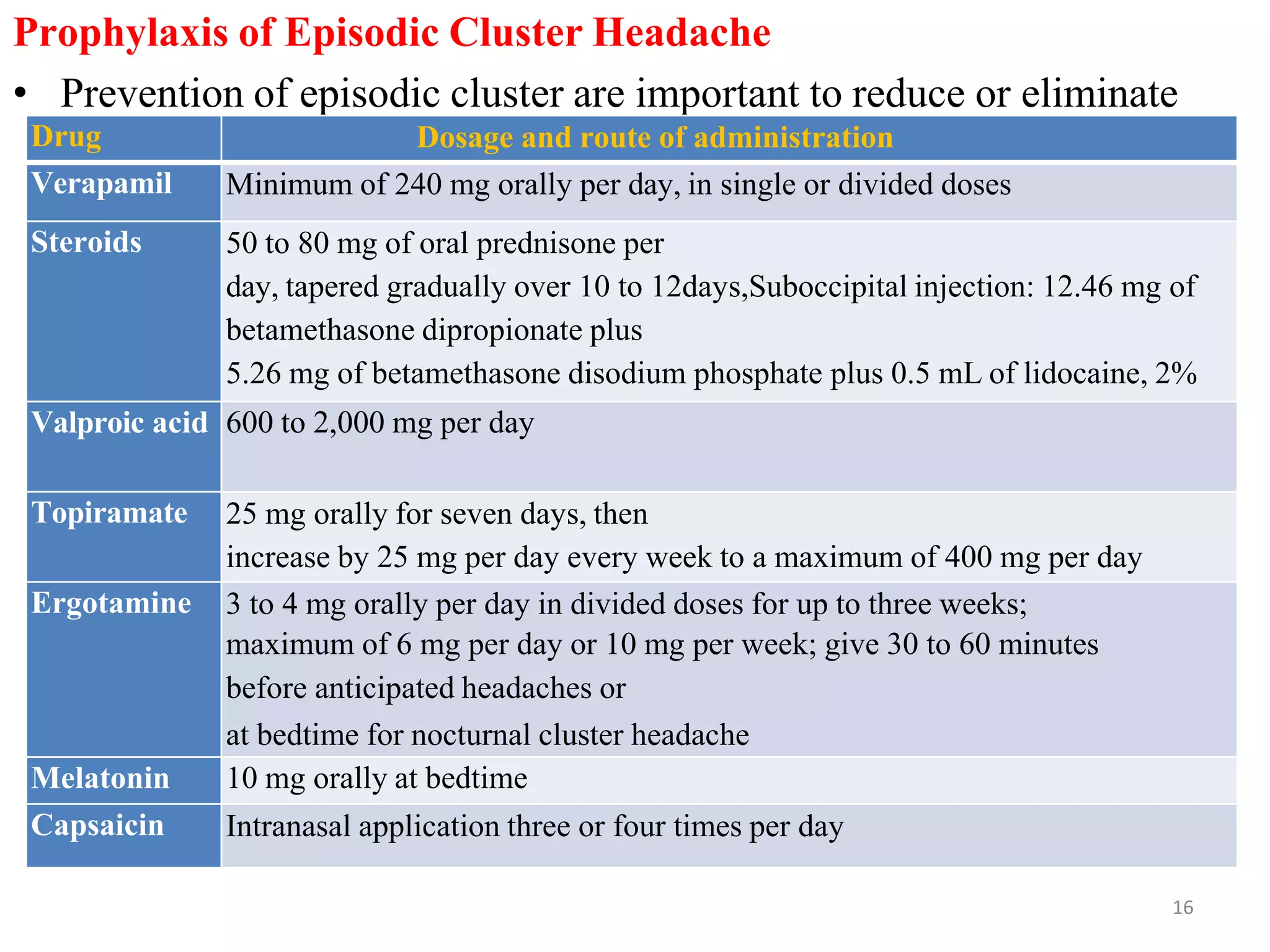
Cluster headaches are severe headaches that occur in cycles. They are characterized by intense, unilateral pain around the eye and lasting 15 minutes to 3 hours. There are two main types - episodic cluster headaches which occur in cycles lasting 7 days to a year, and chronic cluster headaches which occur for longer than a year. Treatment involves oxygen therapy, triptans like sumatriptan, and preventative medications like verapamil, lithium, or topiramate depending on whether the headaches are episodic or chronic.