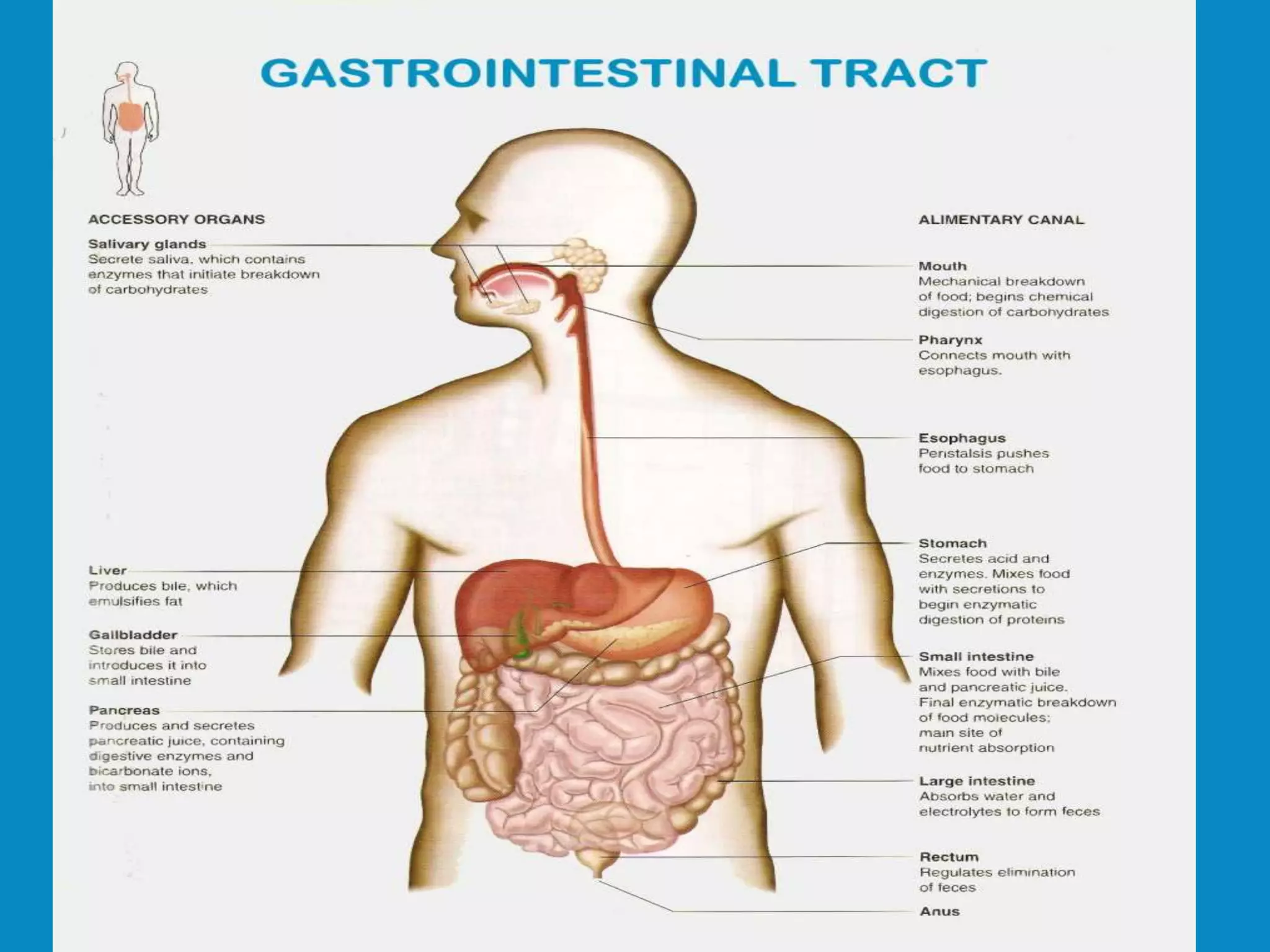
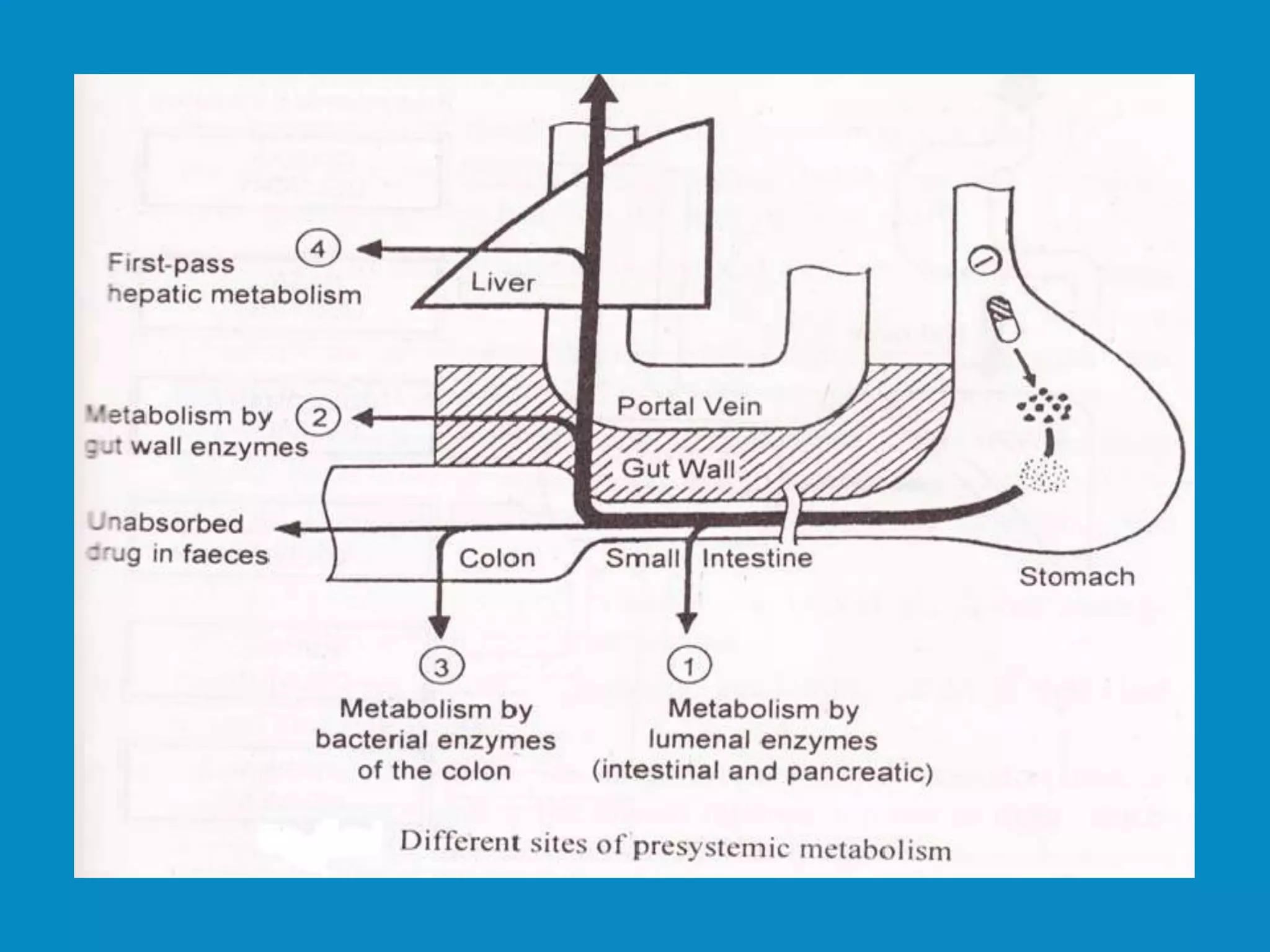
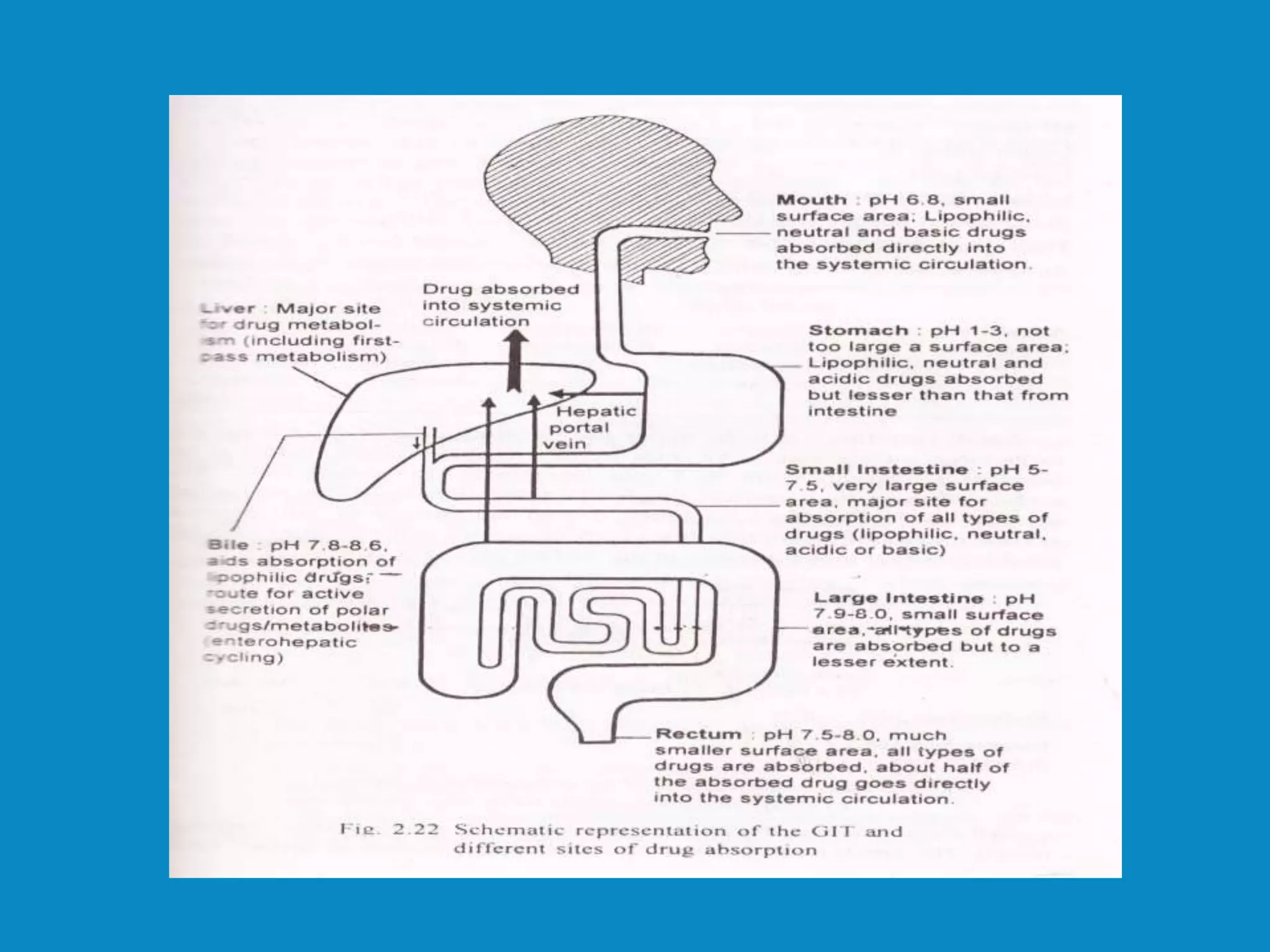
The document discusses the Ayurvedic therapy of Virechana, a purgation method primarily used for Paittika diseases involving the expulsion of vitiated pitta through the anal route. It details the procedural steps, classifications of Virechana drugs based on their origin, mode of action, and intensity, as well as the gastrointestinal anatomy relevant to the therapy. Additionally, it outlines the contraindications and indications for Virechana, emphasizing its application in various gastrointestinal ailments.











































![The digestive system [ Disease & Disorders]](https://cdn.slidesharecdn.com/ss_thumbnails/thedigestivesystem-190425064702-thumbnail.jpg?width=640&height=640&fit=bounds)





![GI PHYSIOLOGY new].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/giphysiologynew-230405152805-b9462356-thumbnail.jpg?width=640&height=640&fit=bounds)
























![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















