Downloaded 18 times

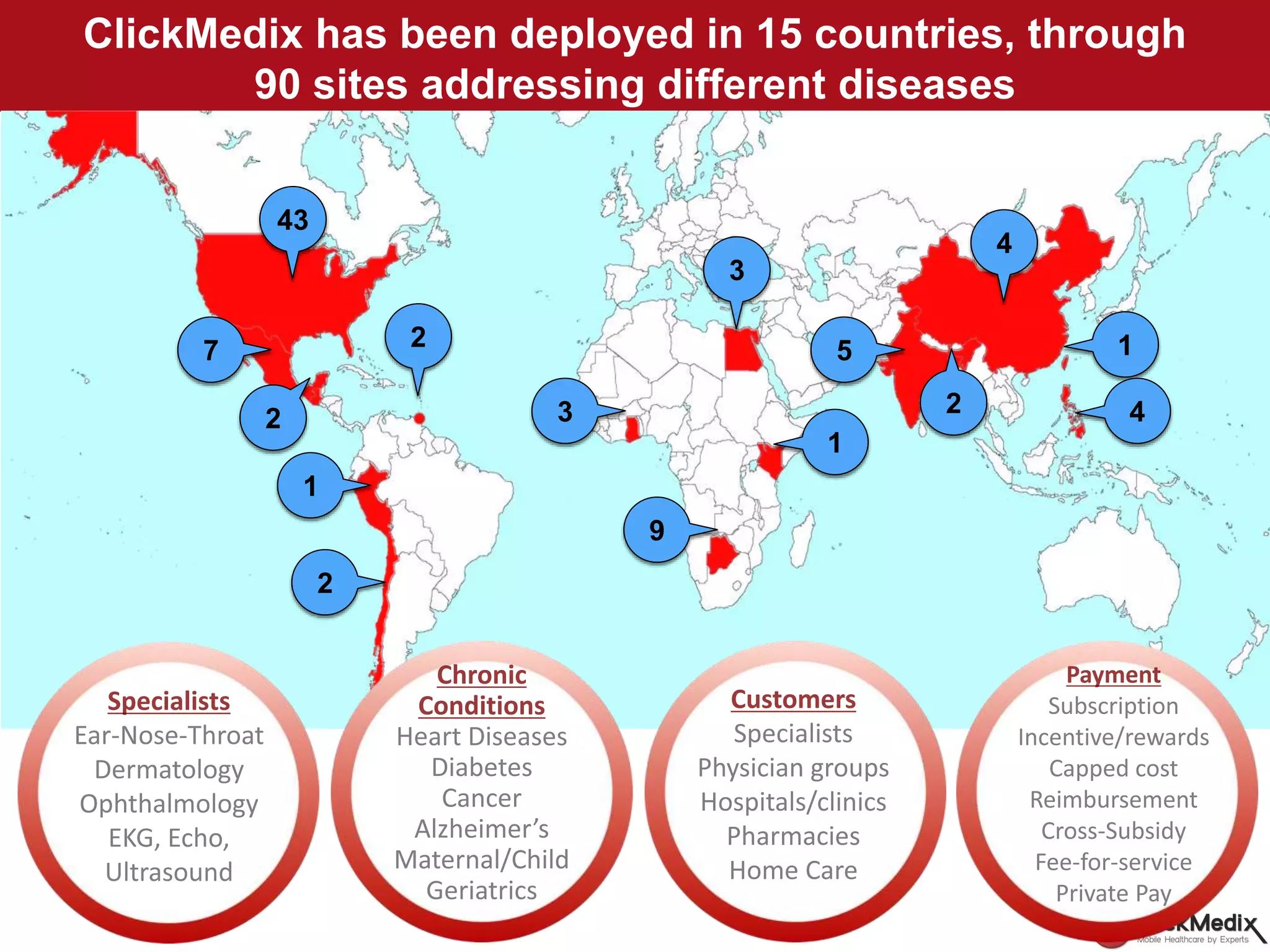
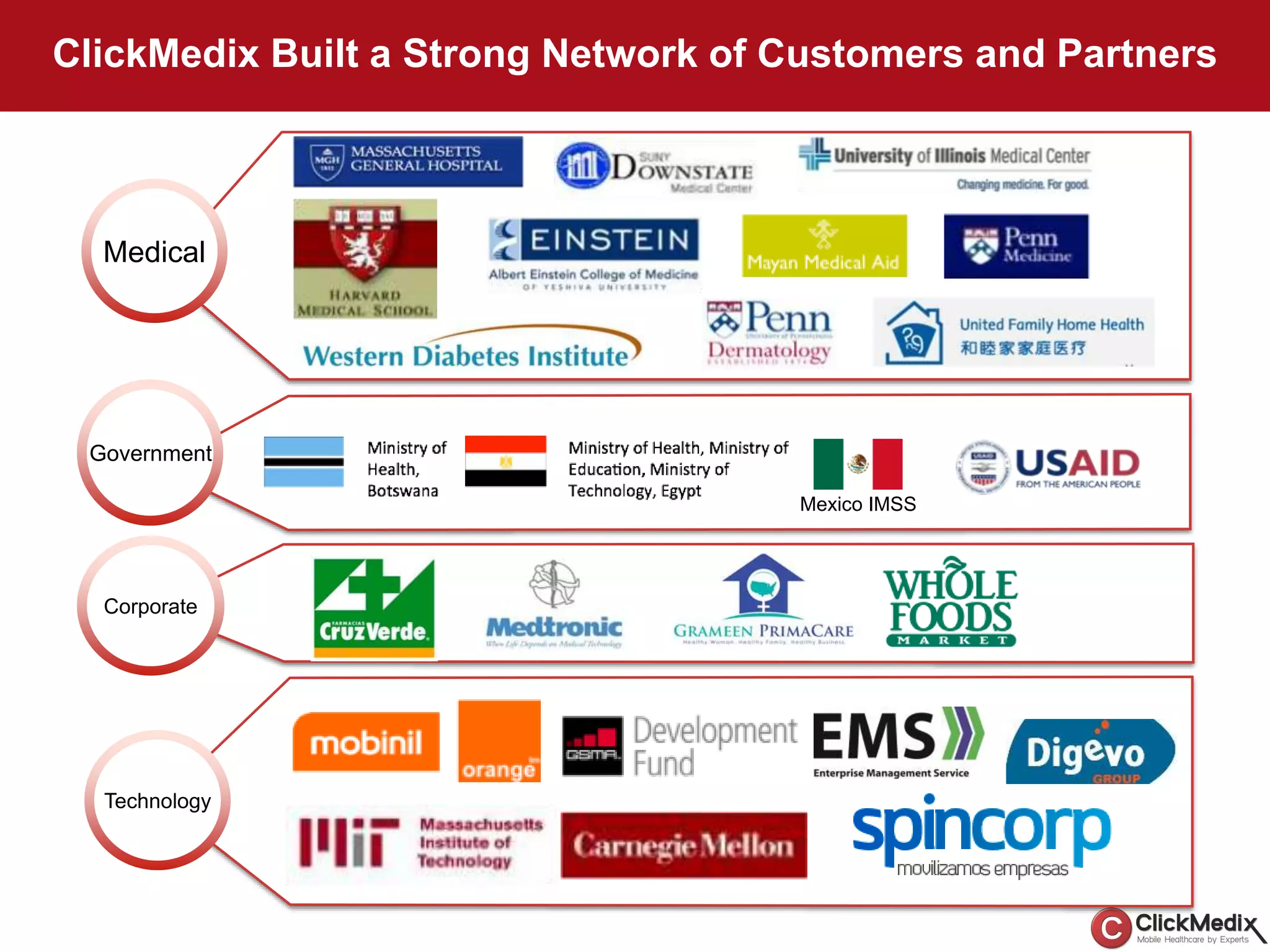
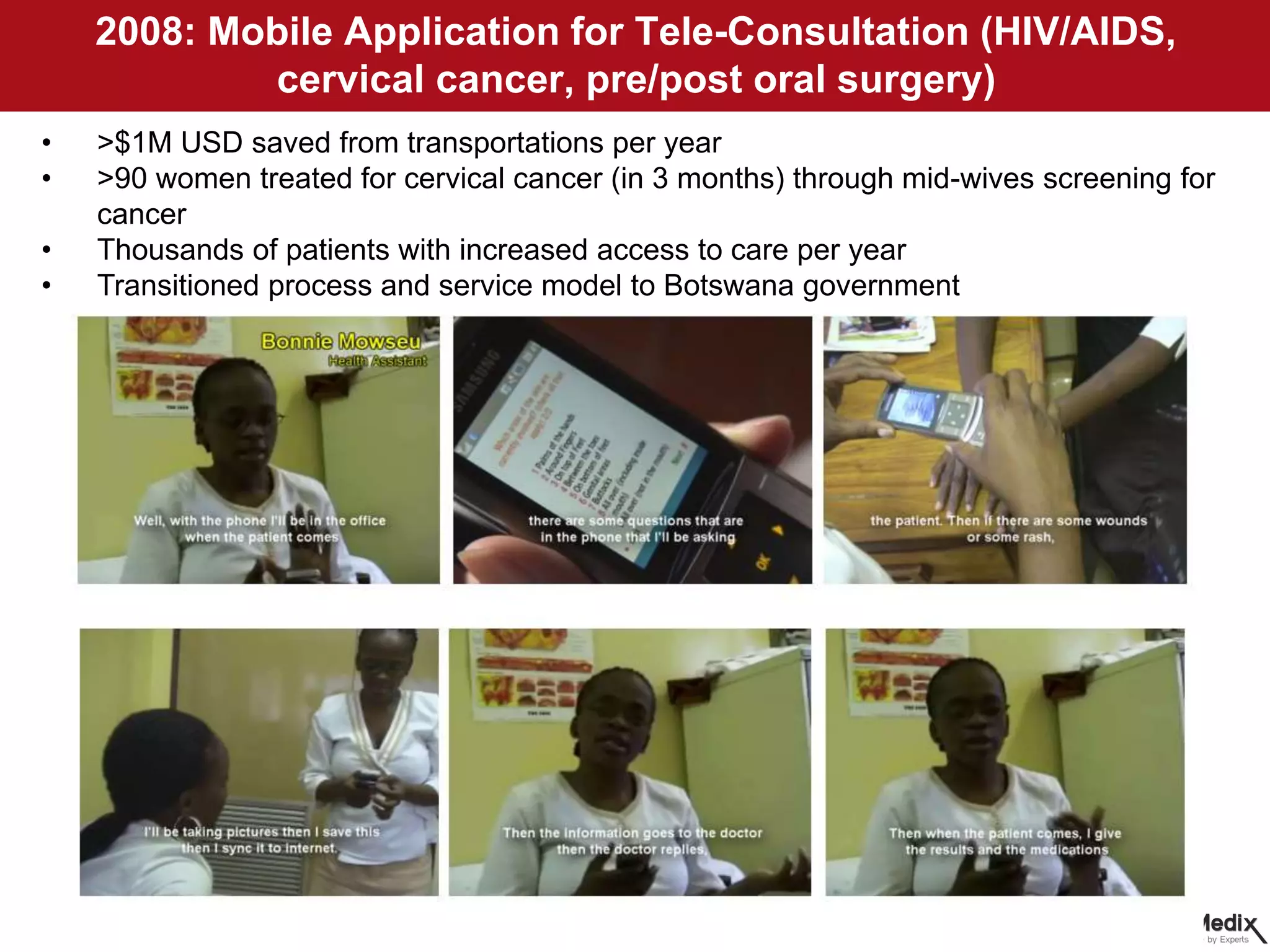
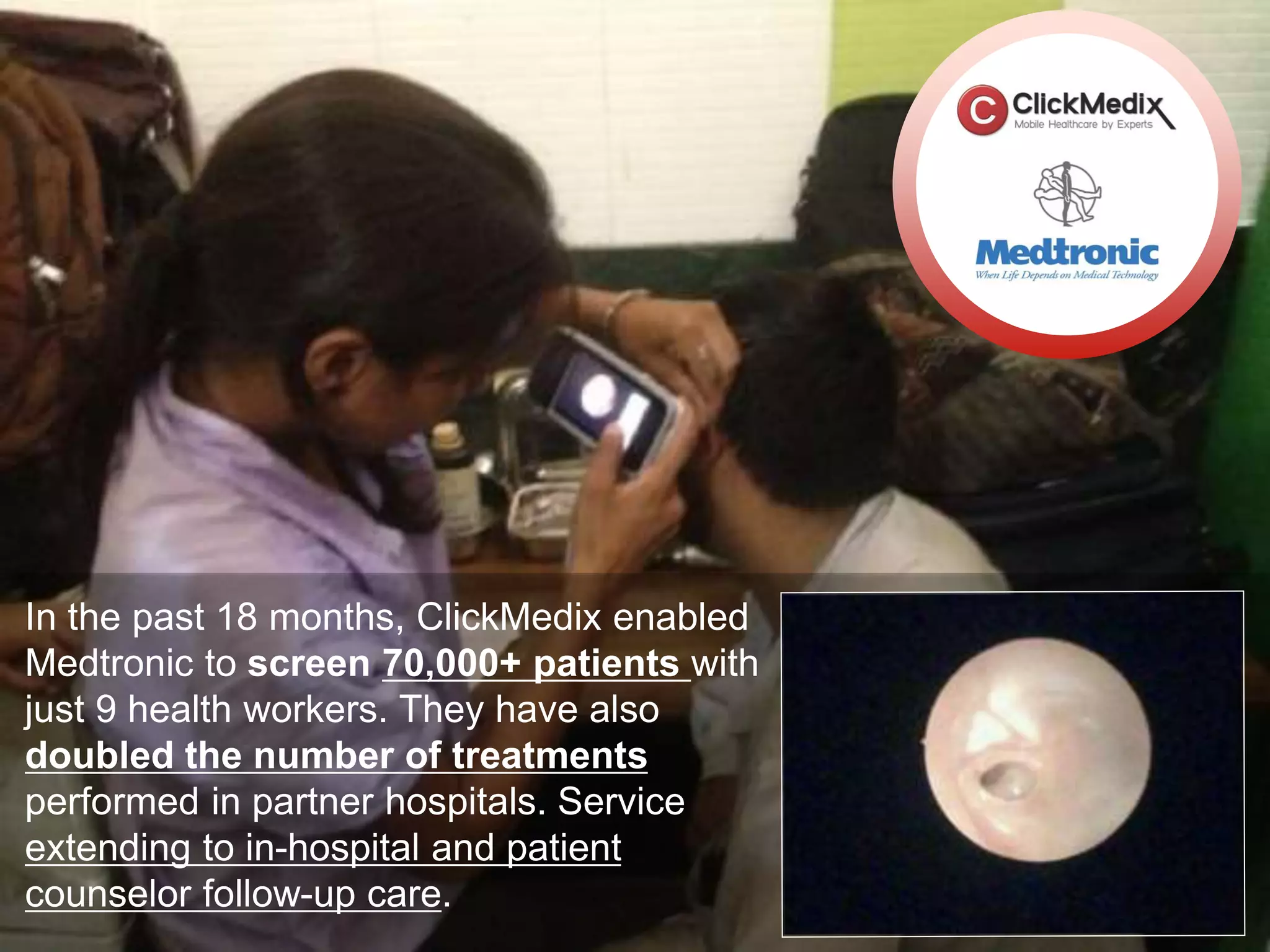
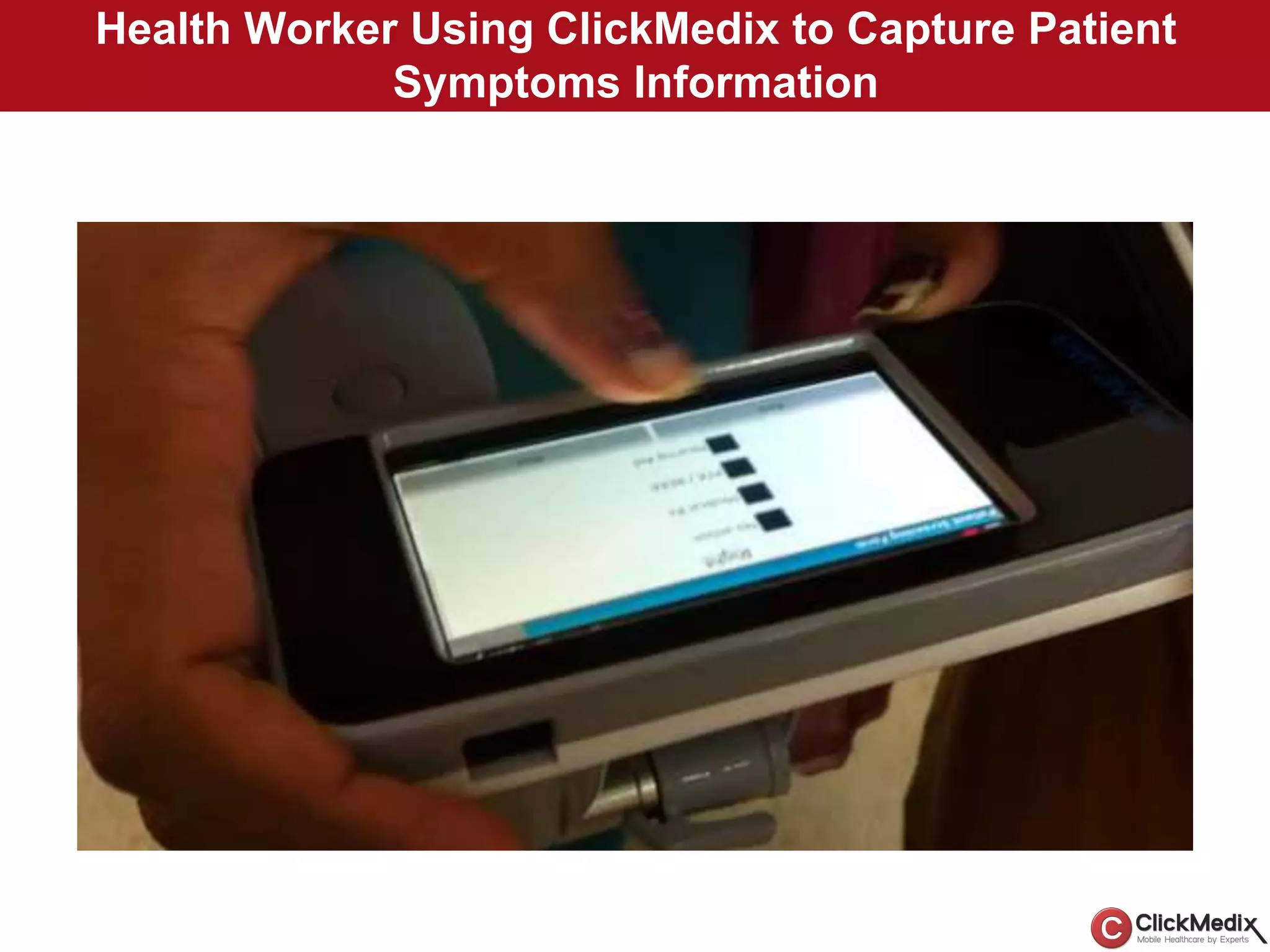

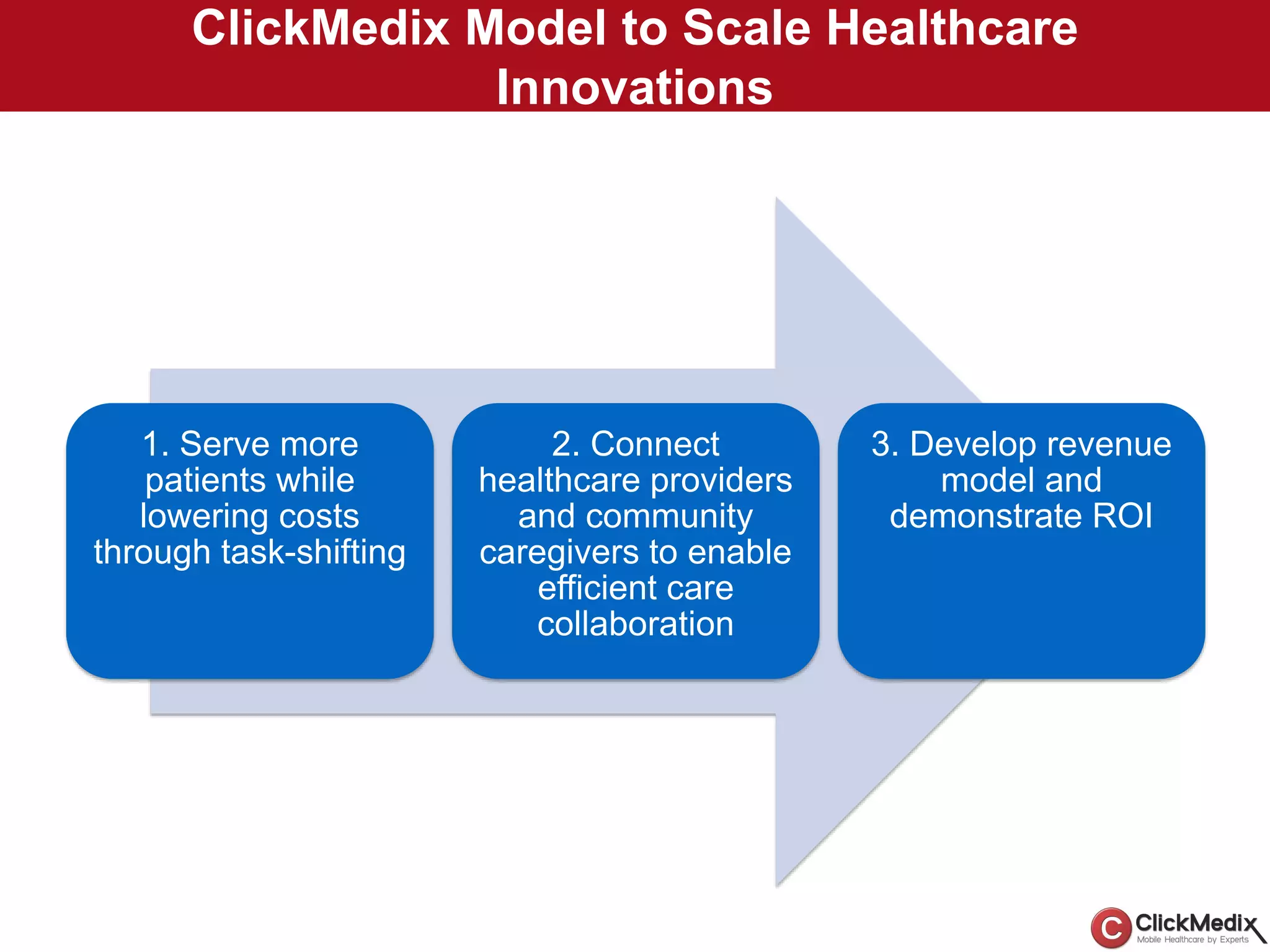
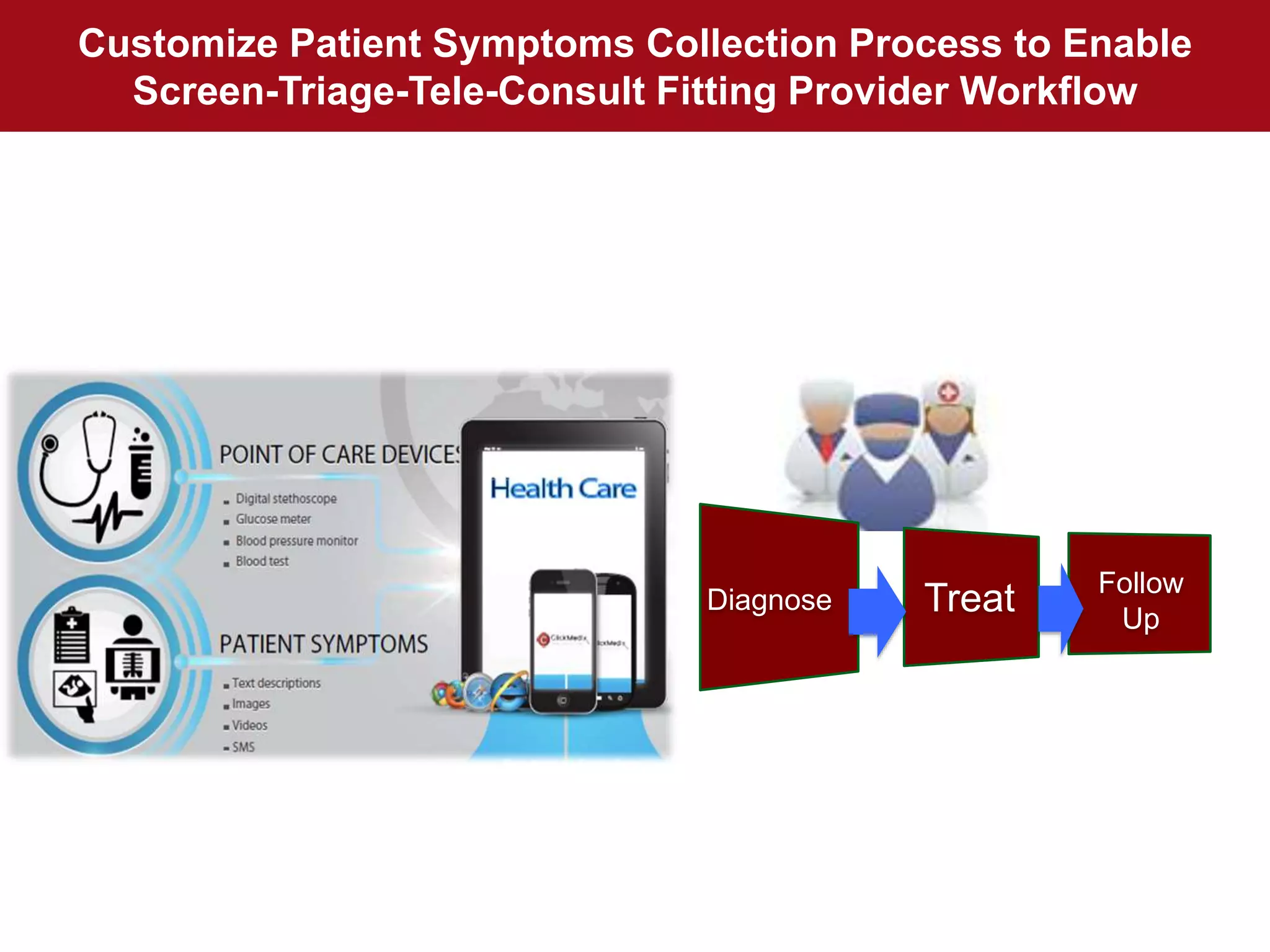

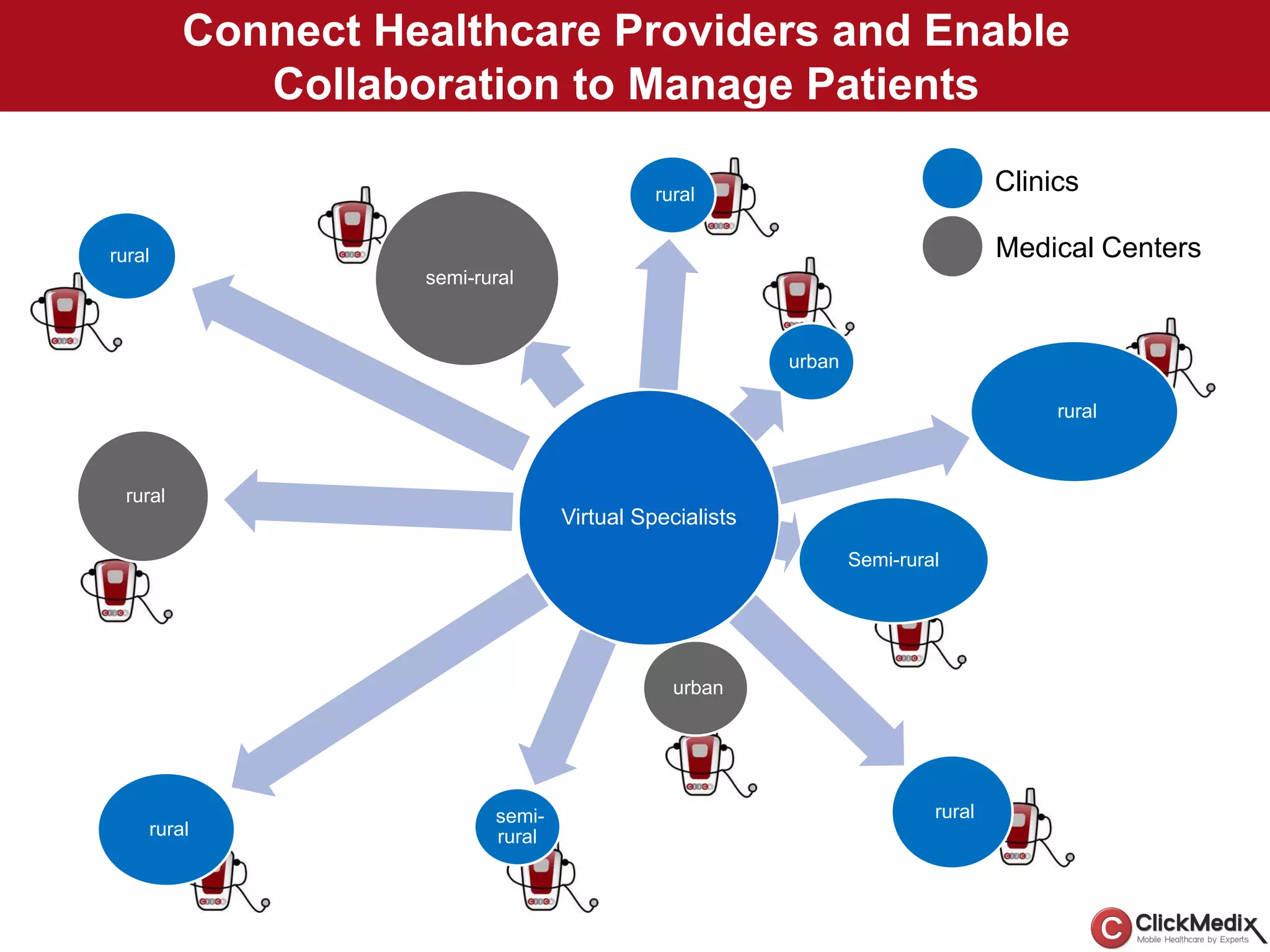
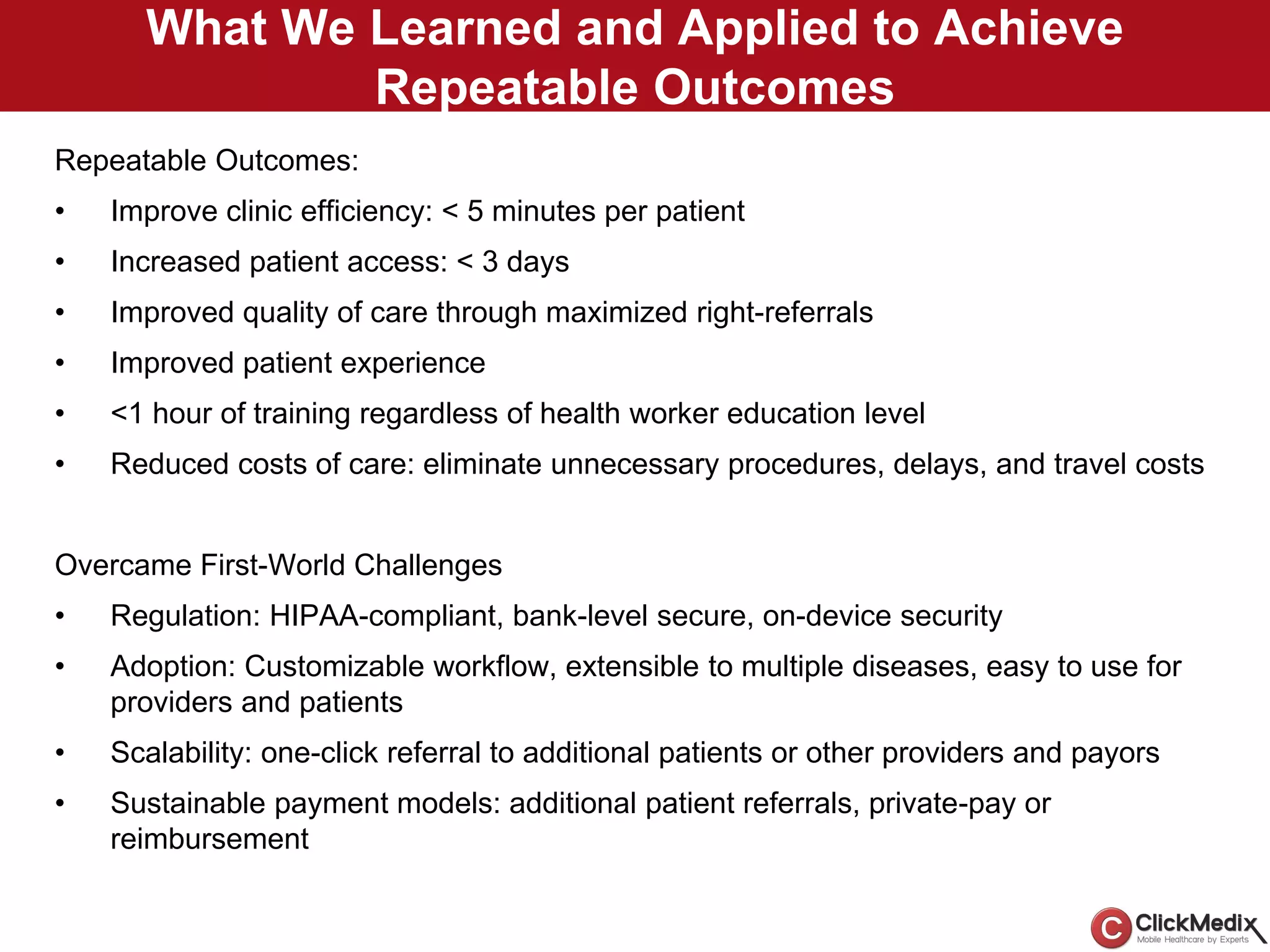
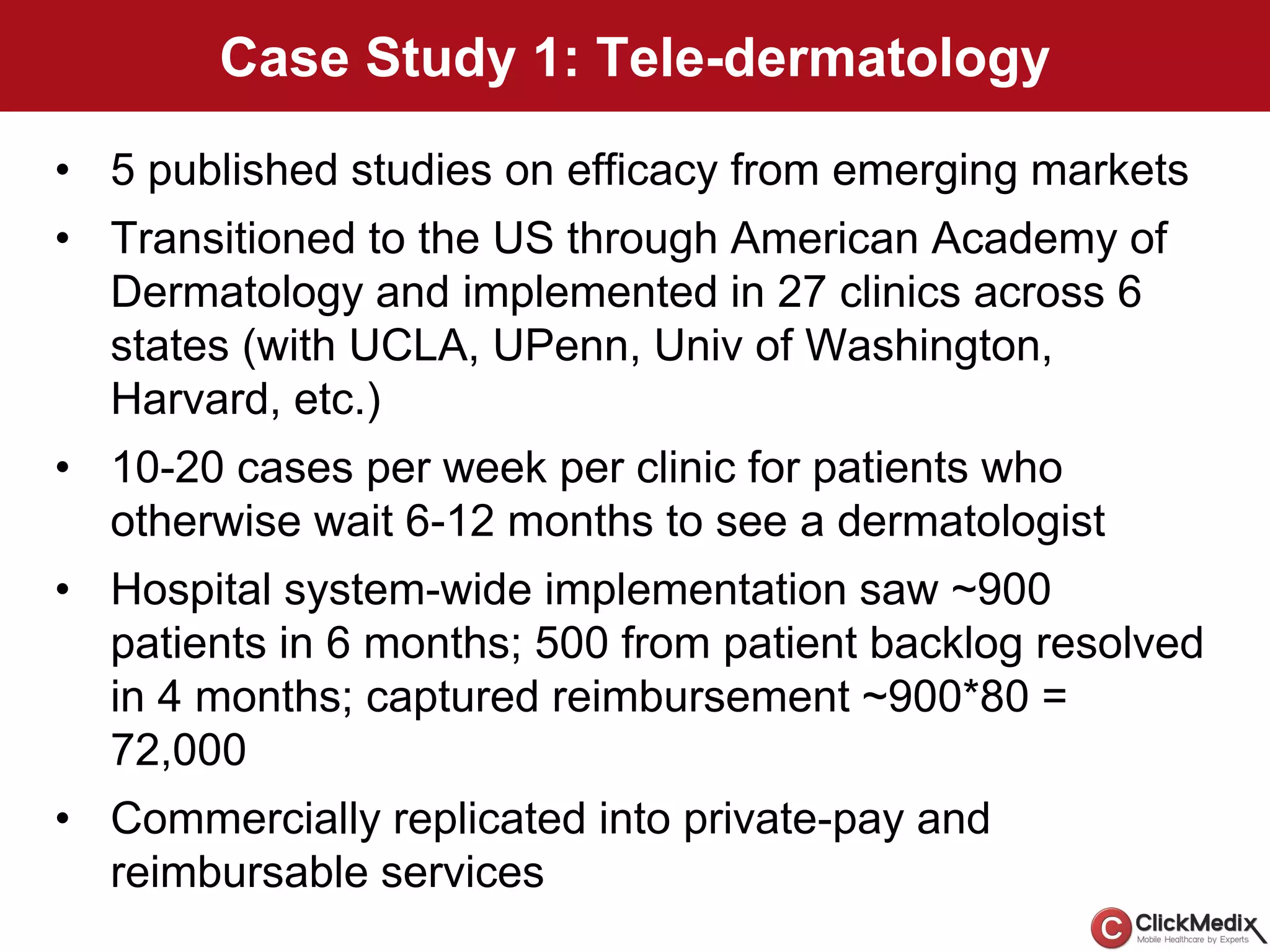

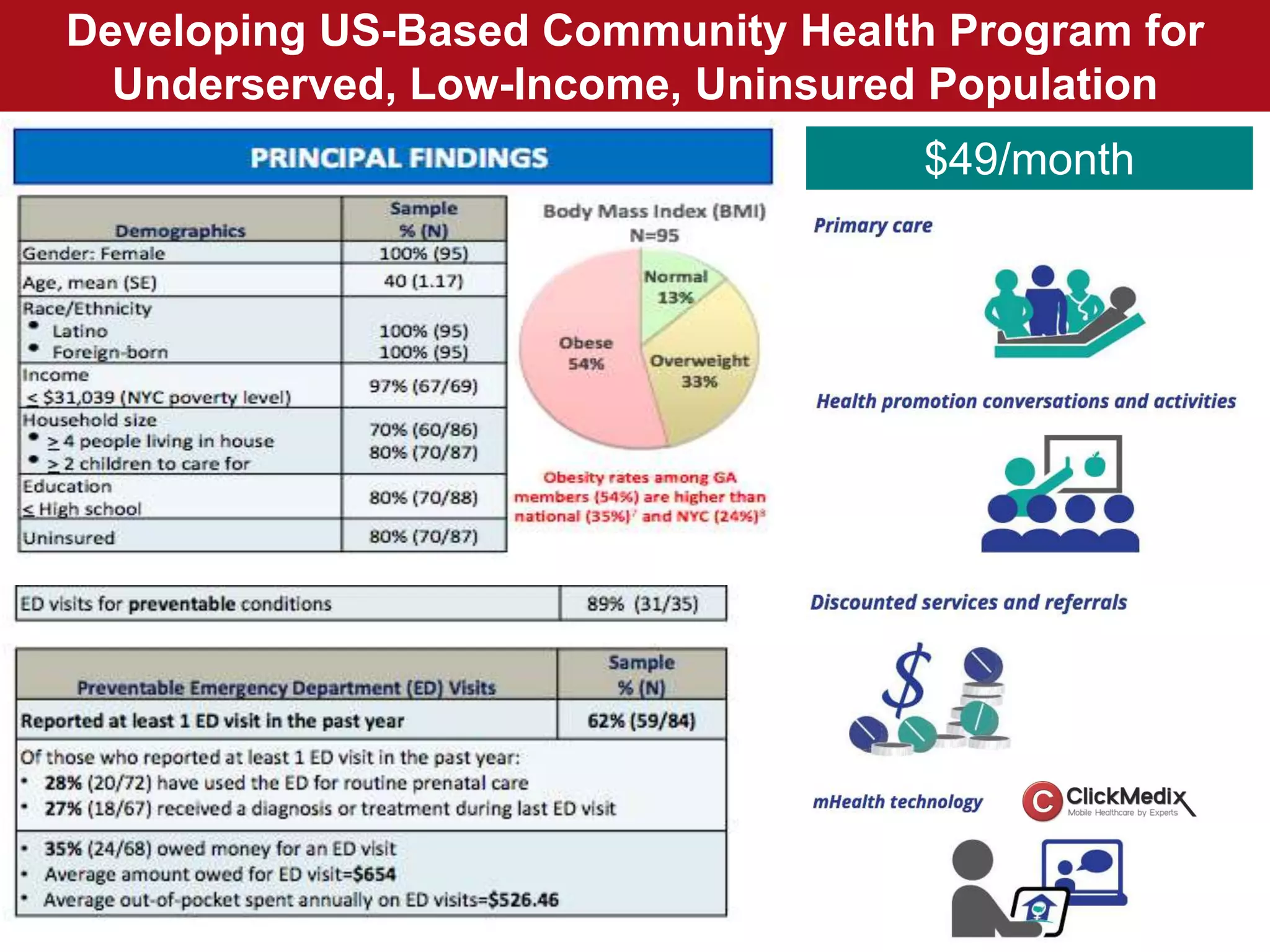

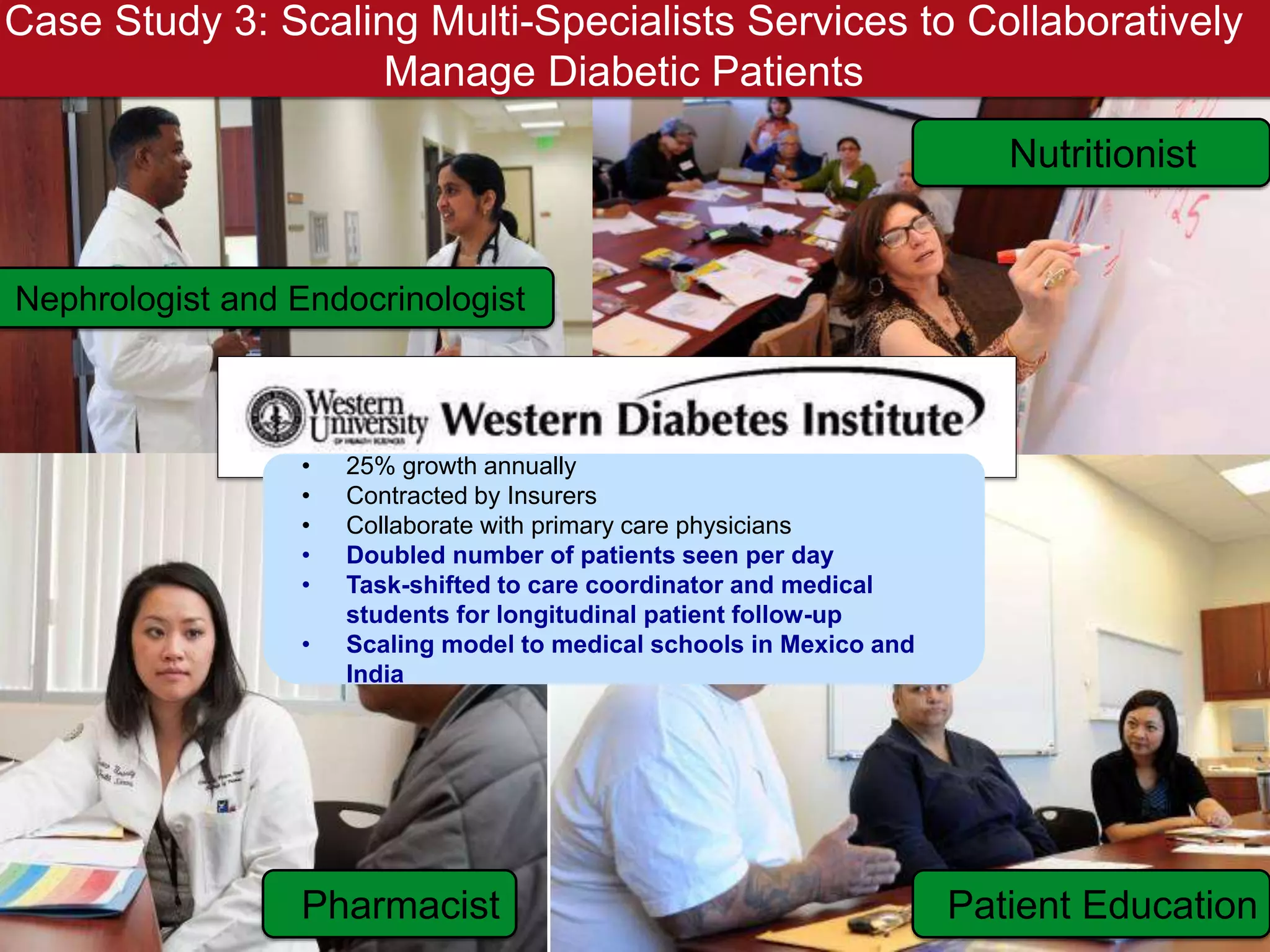
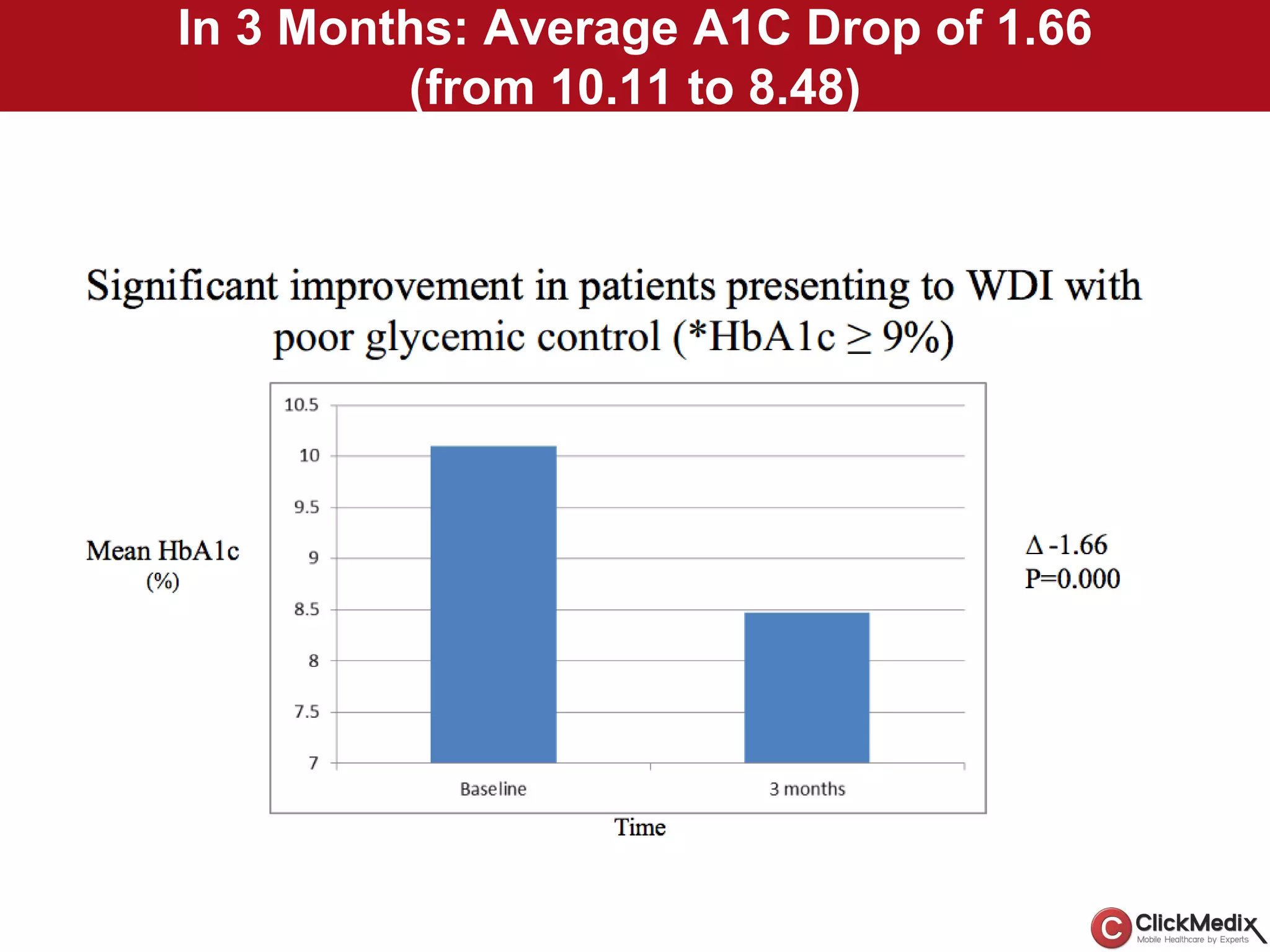
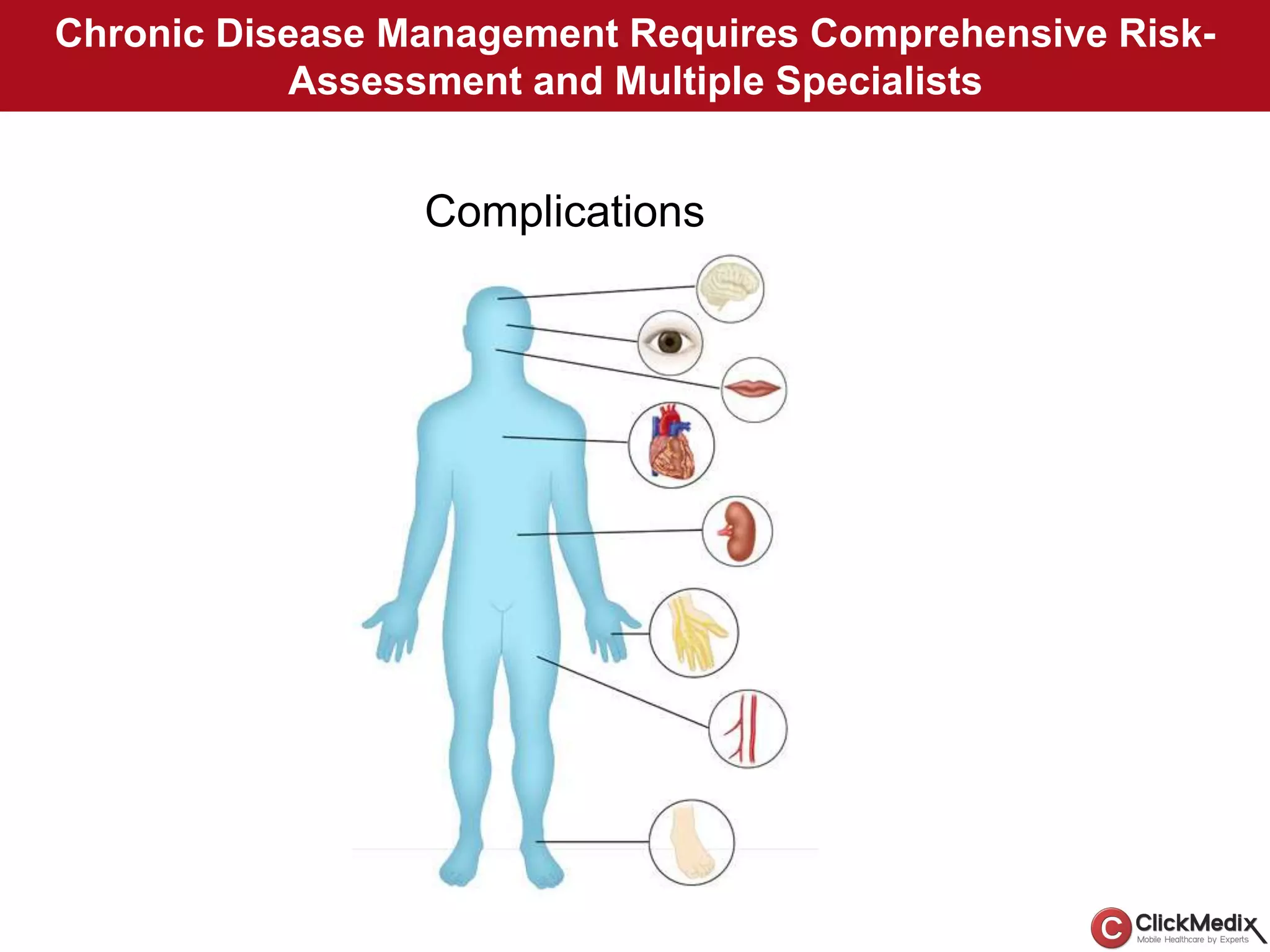


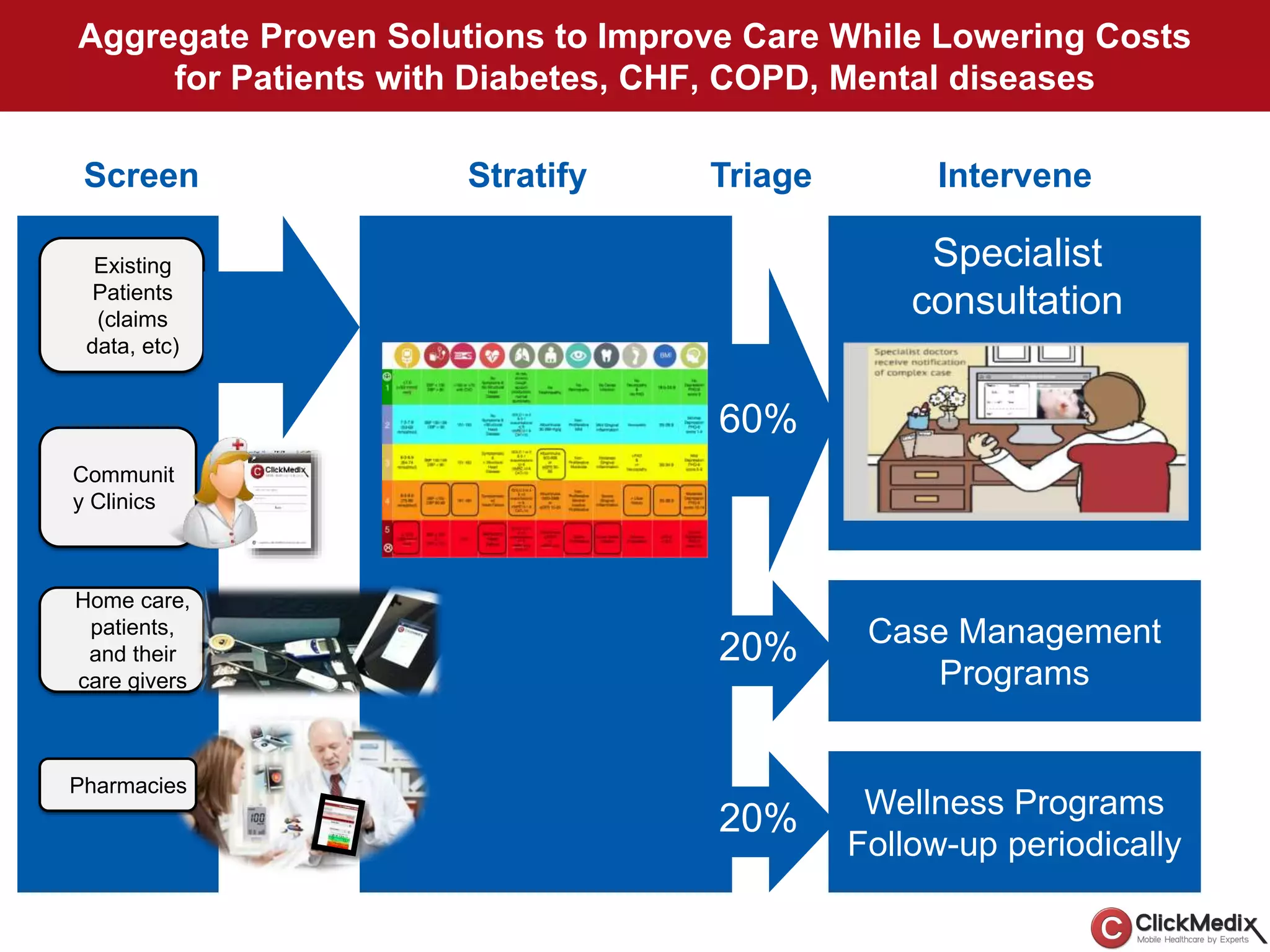
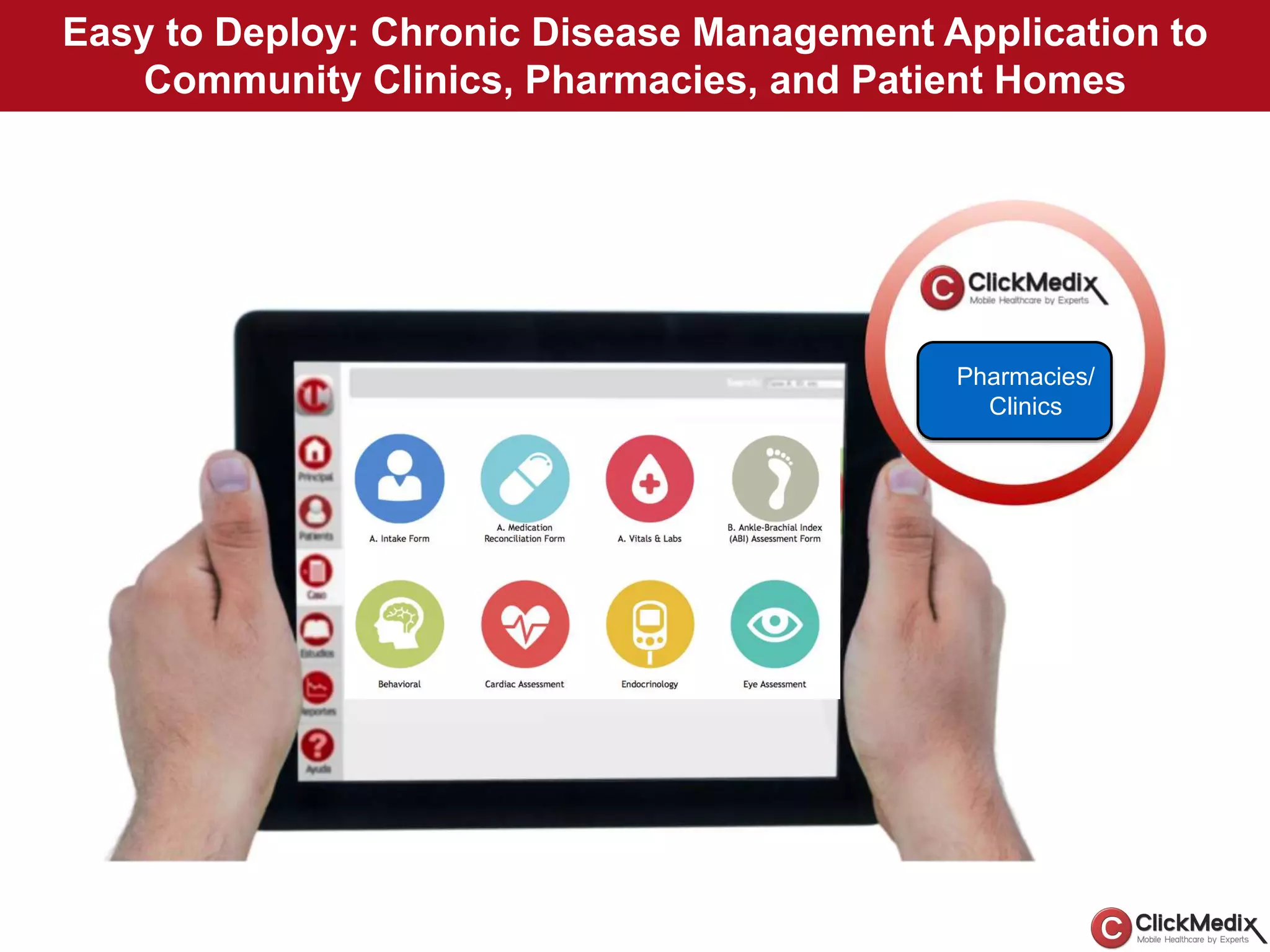
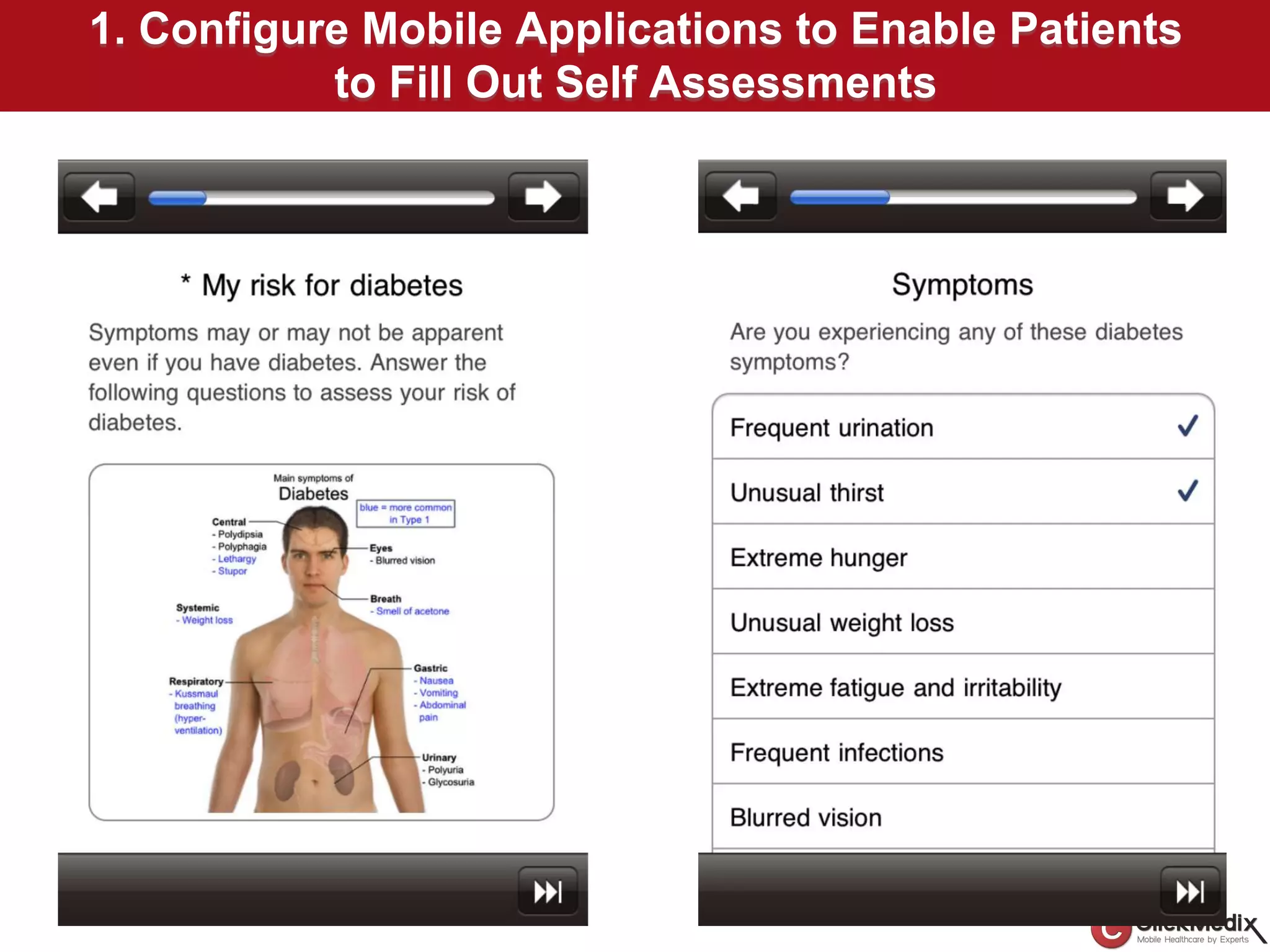

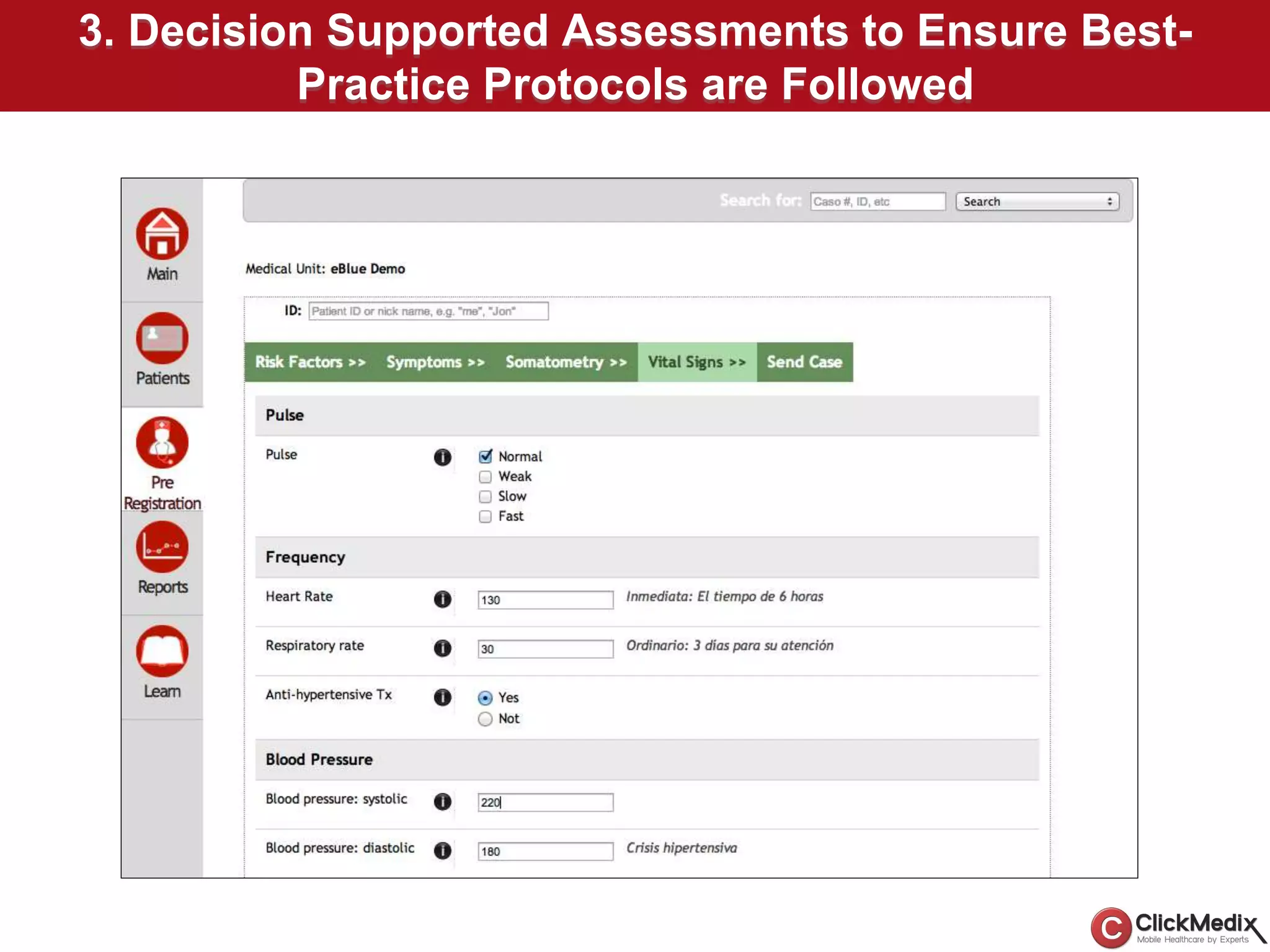


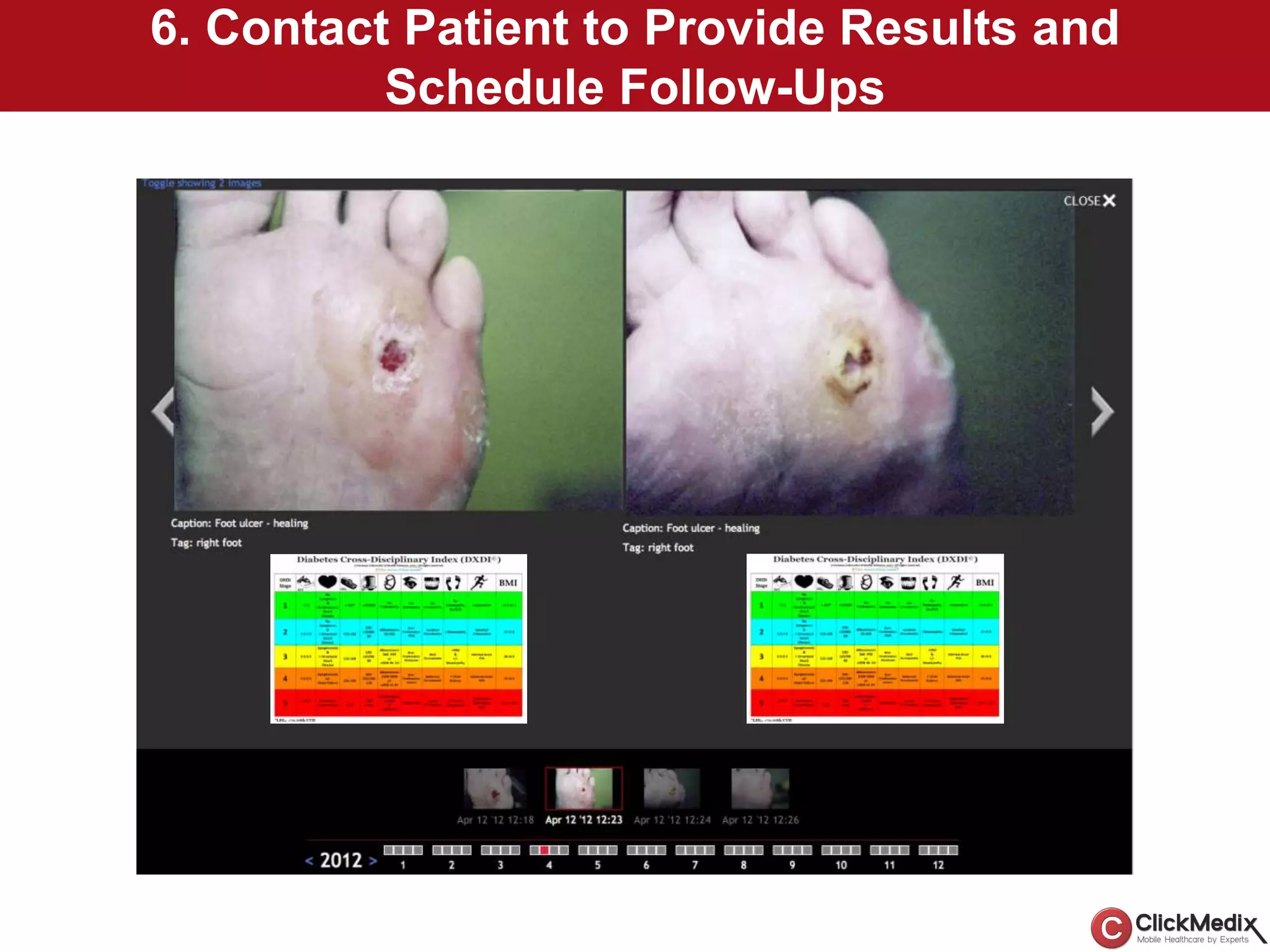

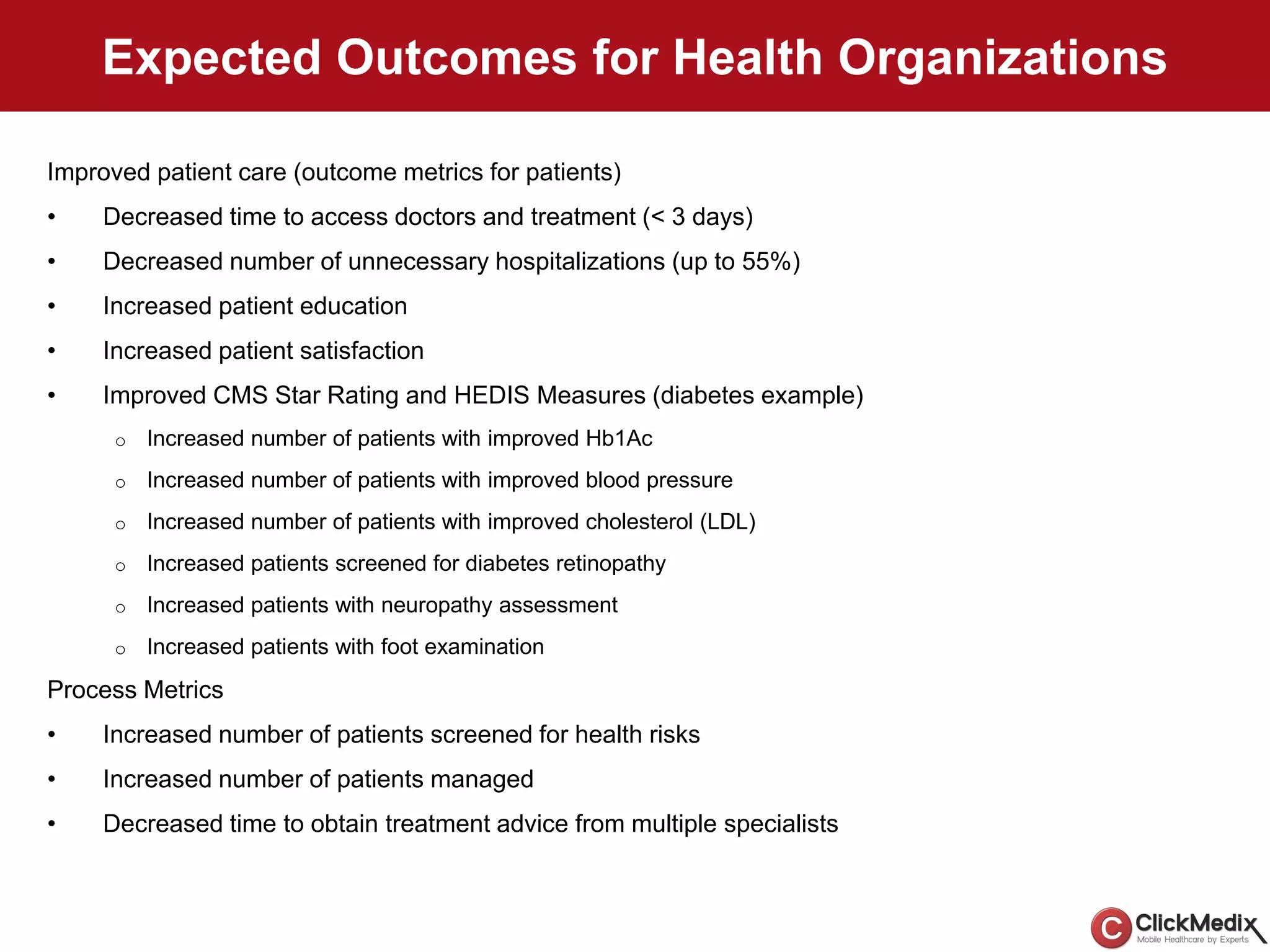
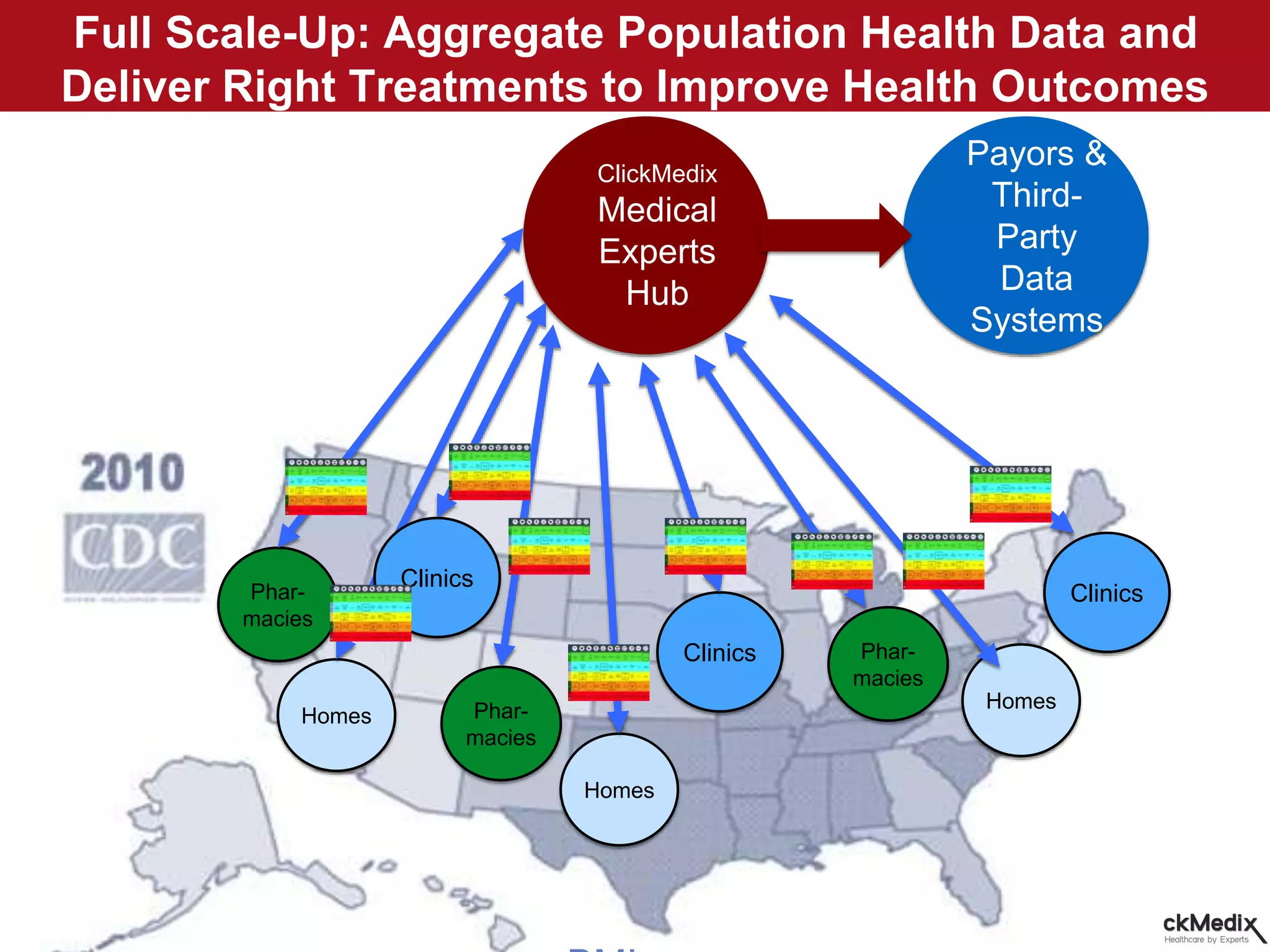

ClickMedix is a connected mHealth platform that enables healthcare organizations to serve more patients better, faster, and at lower costs. It has been deployed in 16 countries through over 90 sites addressing different diseases. ClickMedix provides case studies on scaling tele-dermatology, community-based care for low-income populations, and managing diabetic patients collaboratively with multiple specialists. The platform aims to improve access to care through task-shifting to nurses and community health workers while lowering costs.








































































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)