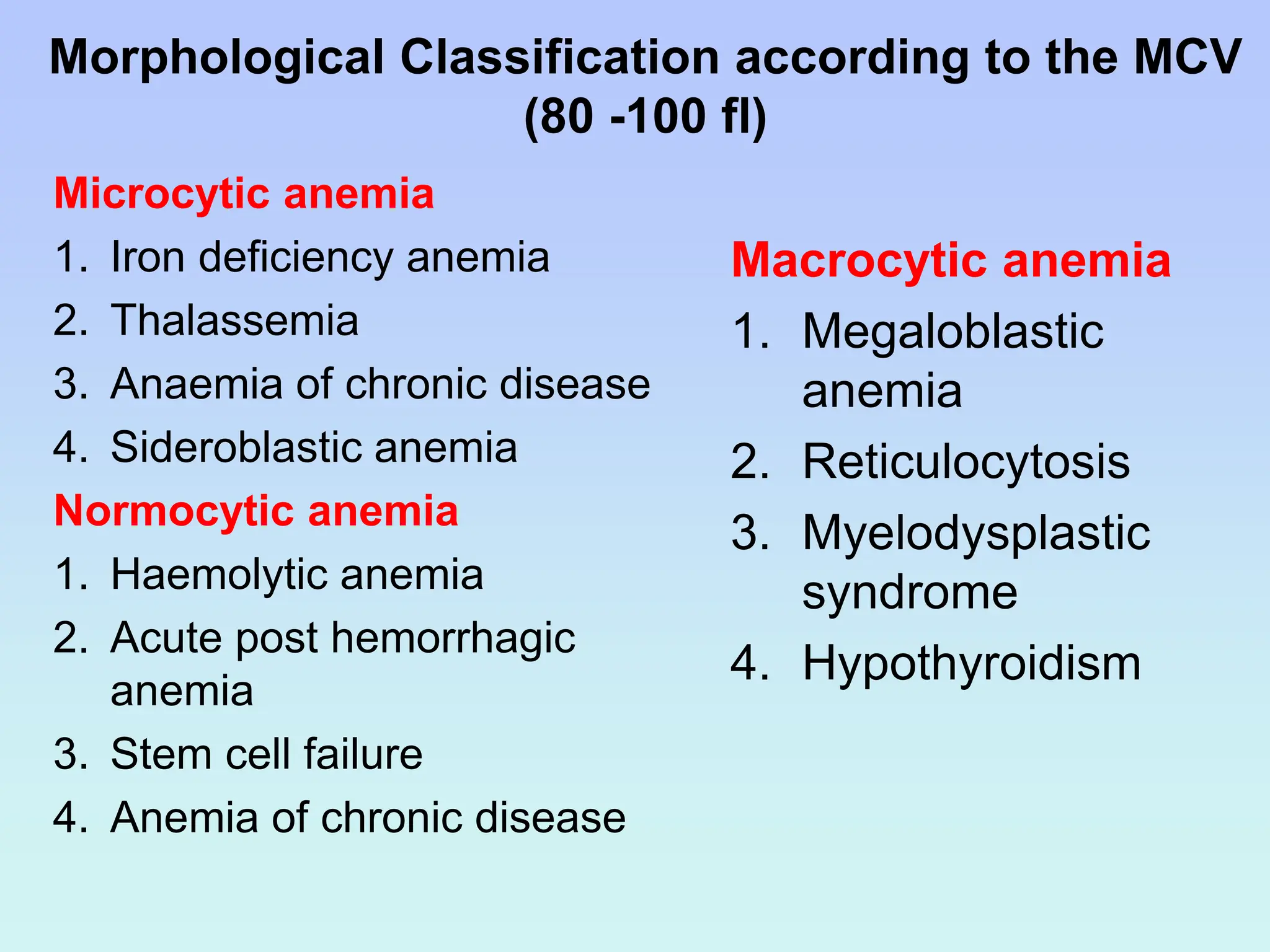
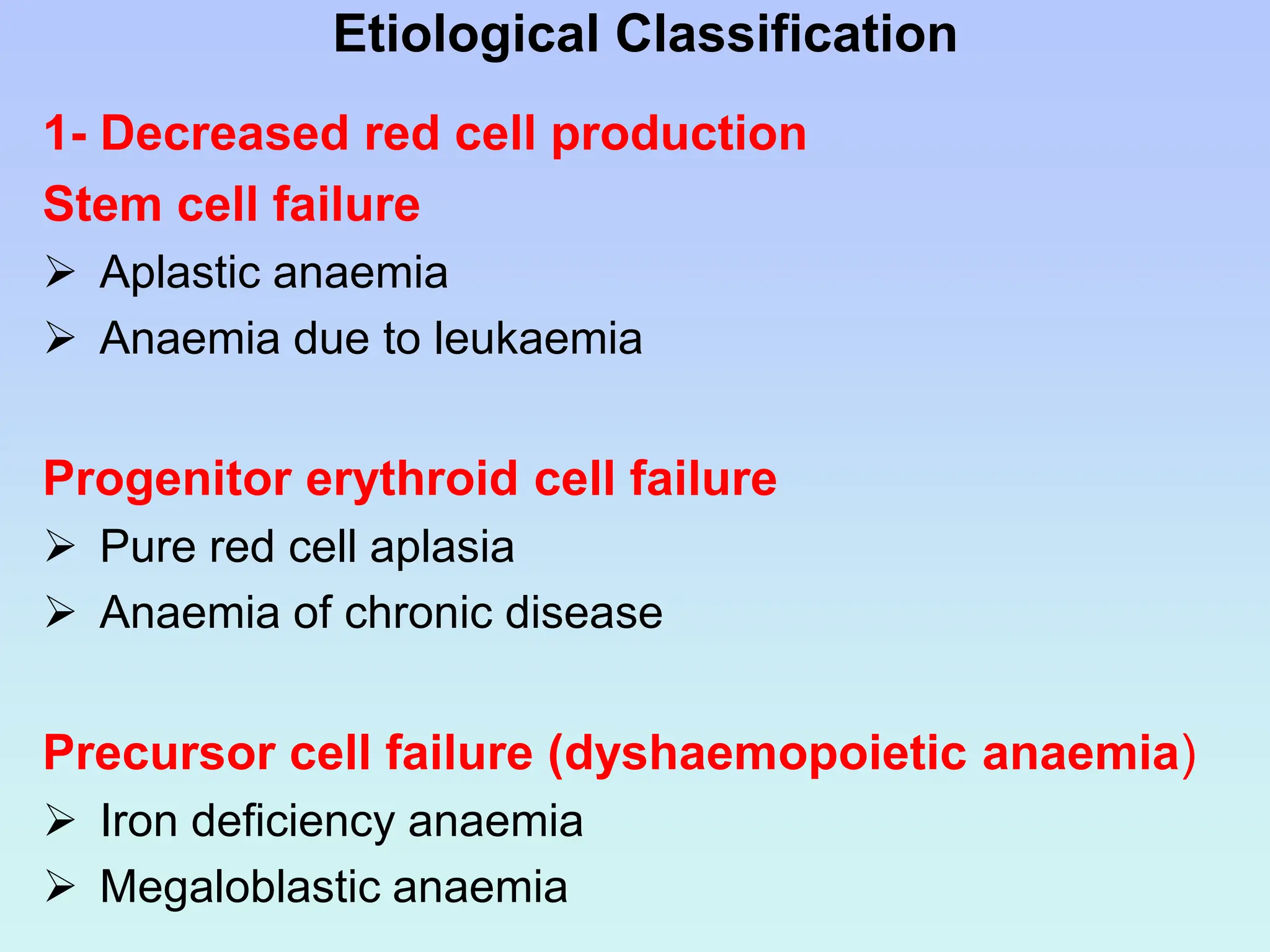
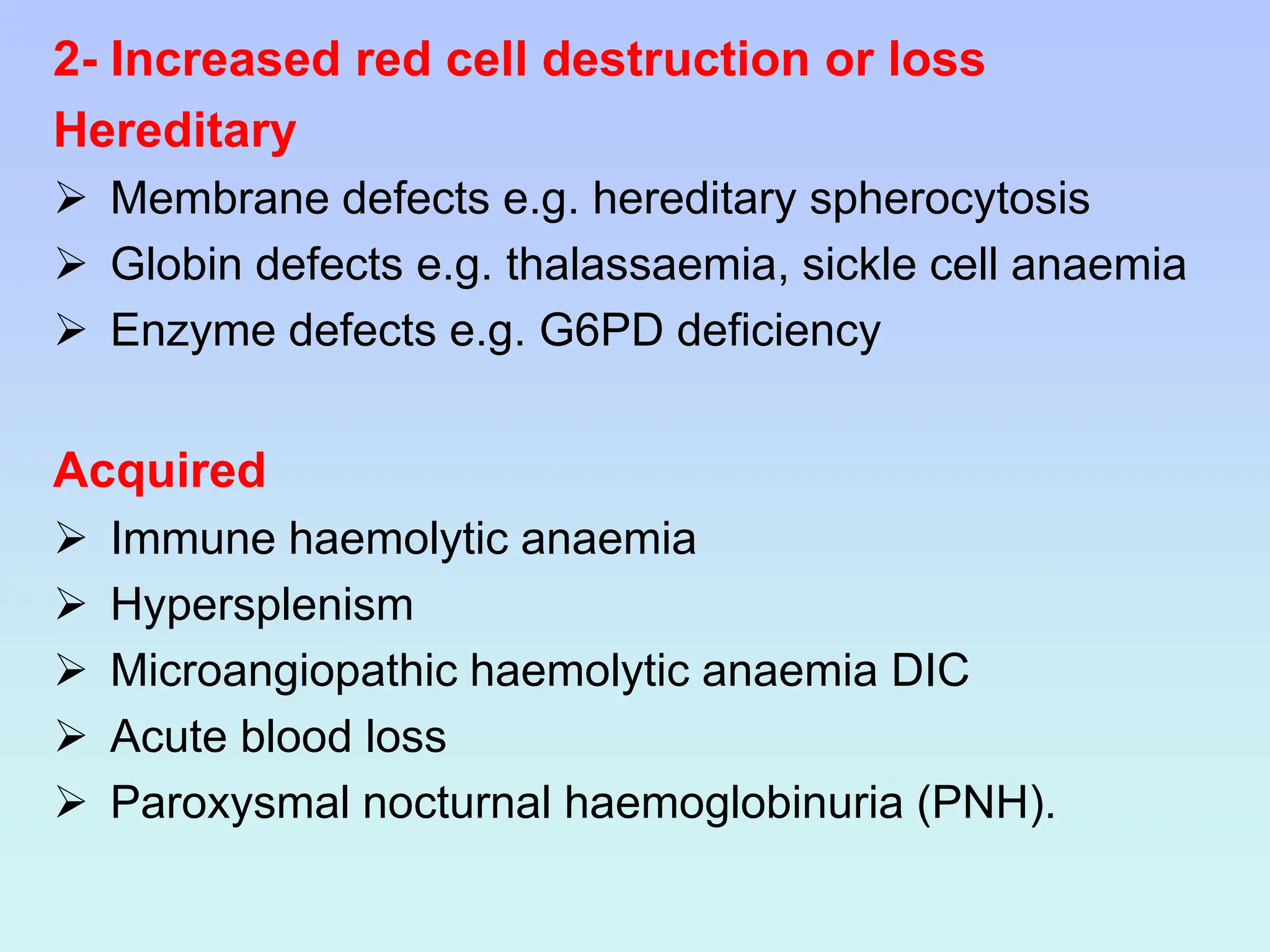
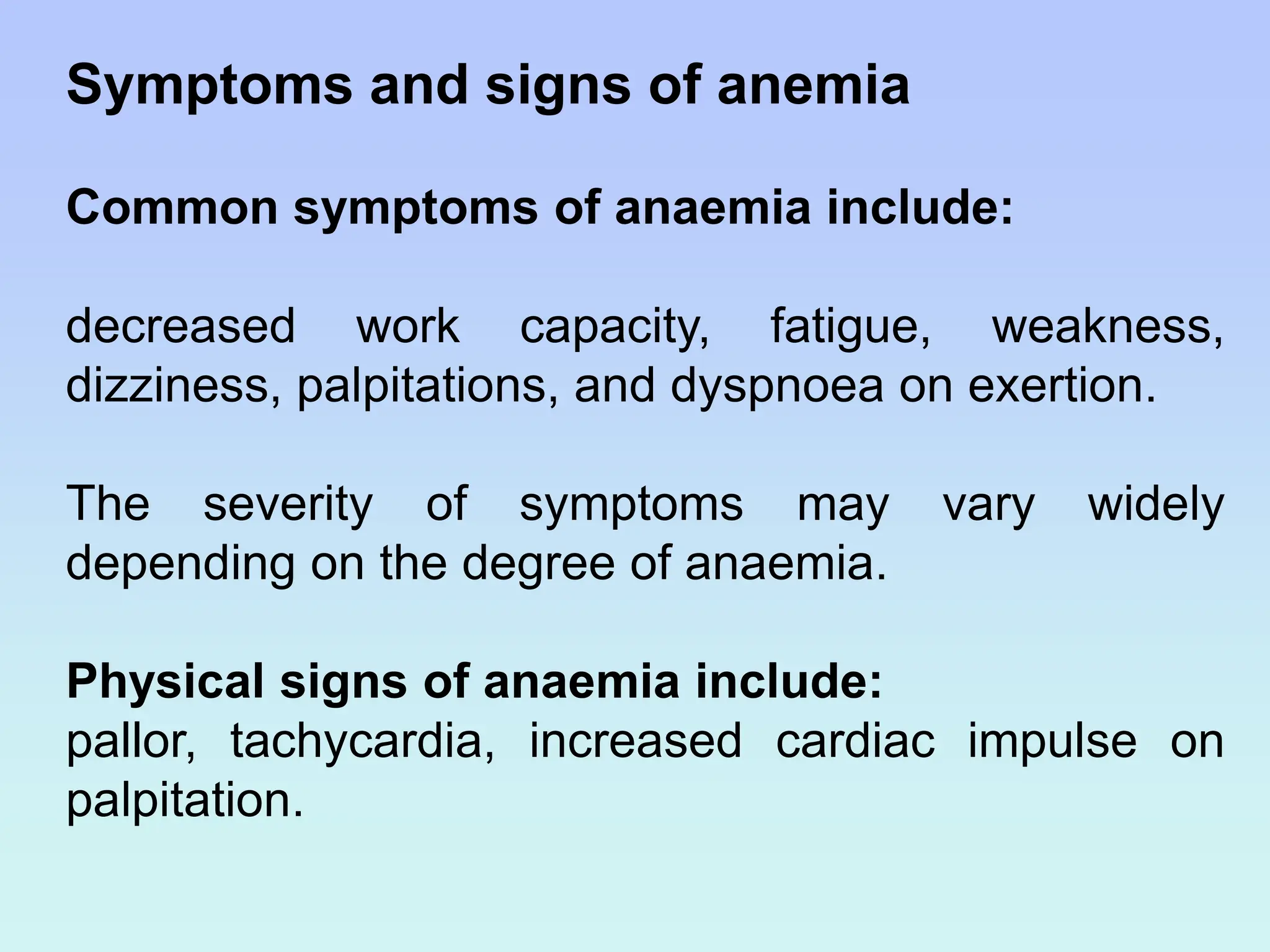
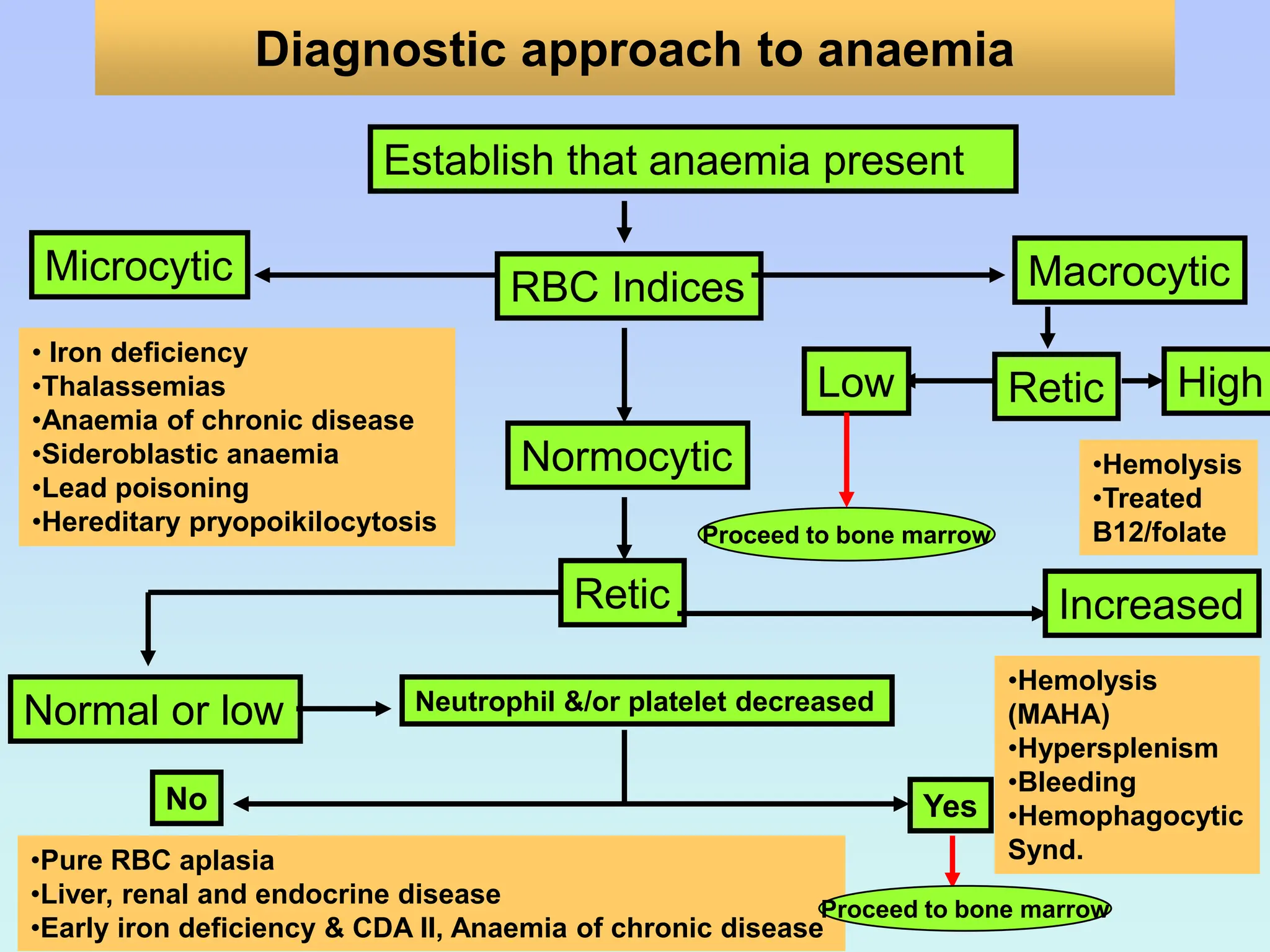
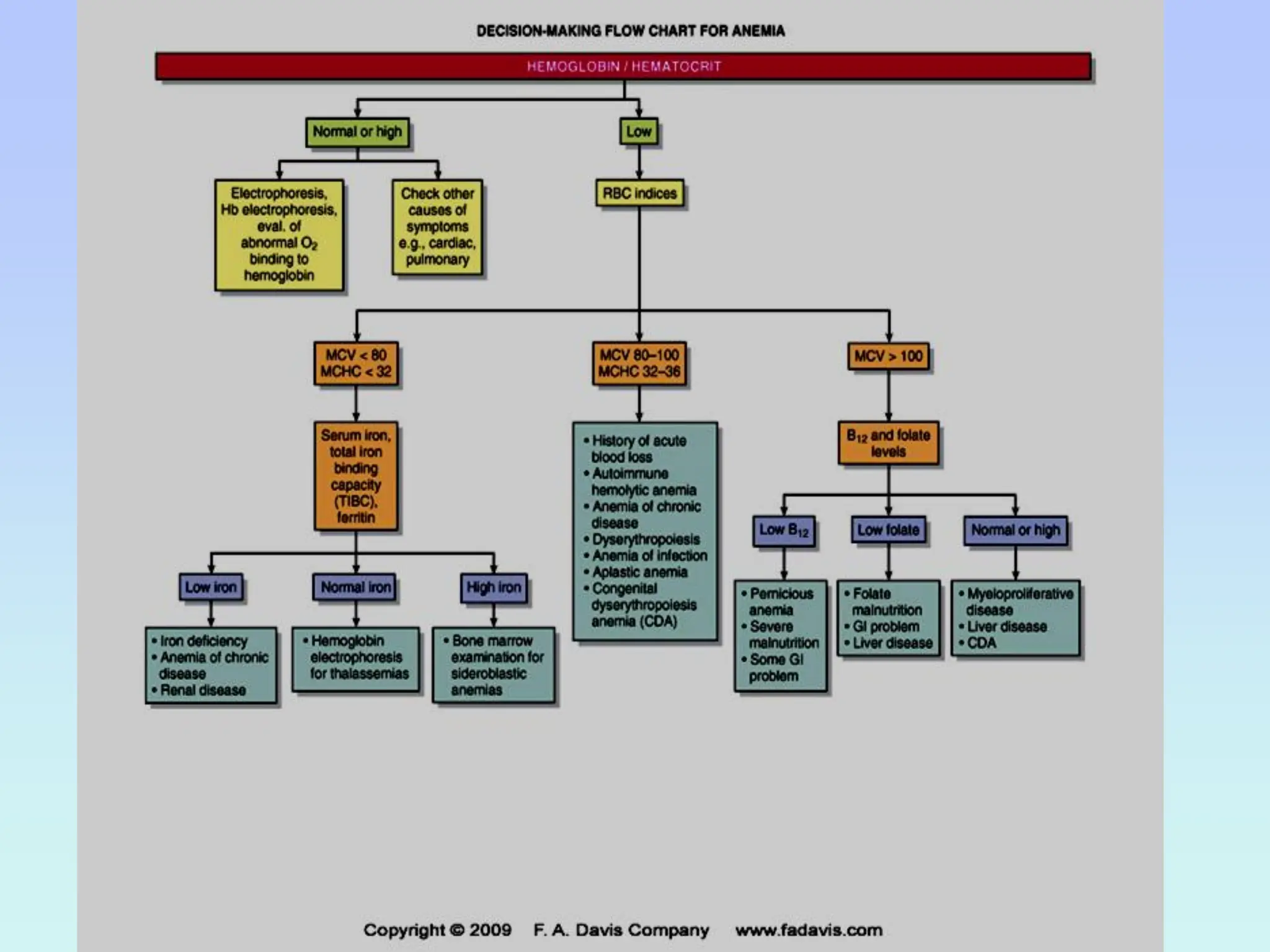
This document provides a comprehensive overview of anemia, detailing its definition, classification, symptoms, and diagnostic approaches. Anemia is characterized by a reduction in hemoglobin concentration, with causes classified morphologically, functionally, and etiologically. Key laboratory investigations include complete blood counts and reticulocyte counts to determine underlying causes and guide treatment.