Pathophysiology subject B. Pharmacy student in Sem-II, COPD unit of respiratory system, used by student to under stand those point and concept clear study.
To help by images and proper justification to remember point cover.
Chronic Obstructive PulmonaryDisease (COPD) or Chronic Obstructive Airway
Disease (COAD) or Chronic Airway Obstruction (CAO), are commonly used clinical
terms for a group of pathological conditions in which there is chronic, partial or
complete, obstruction to the airflow at any level from trachea to the smallest airways
resulting in functional disability of the lungs i.e. these are diffuse lung diseases.
One etiologic factor which is a common denominator in all forms of COPD is smoking.
The following entities are included in COPD:
I. Chronic bronchitis ( Long term inflammation of the bronchi)
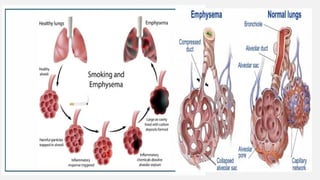
II. Emphysema (Permanent enlargement of the airspaces & Destruction of the
walls alveolar sac)
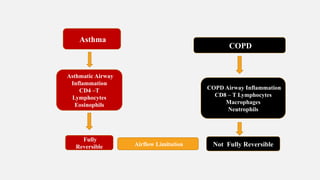
III. Bronchial asthma (Reversible airflow obstruction)
IV. Bronchiectasis (Persistent, productive cough with large amounts of sputum)
V. Small airways disease (bronchiolitis)
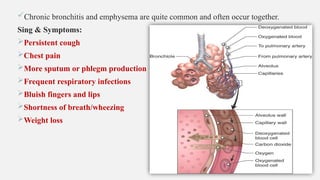
Chronic bronchitis andemphysema are quite common and often occur together.
Sing & Symptoms:
Persistent cough
Chest pain
More sputum or phlegm production
Frequent respiratory infections
Bluish fingers and lips
Shortness of breath/wheezing
Weight loss
7.
CHRONIC BRONCHITIS
Chronic bronchitis is a common condition defined clinically as persistent cough with expectoration on
most days for at least three months of the year for two or more consecutive years.
The cough is caused by over secretion of mucus. Inspite of its name, chronic inflammation of the
bronchi is not a prominent feature. The condition is more common in middle-aged males than
females; approximately 20% of adult men and 5% of adult women have chronic bronchitis, but only
a minority of them develop serious disabling COPD. Quite frequently, chronic bronchitis is associated
with emphysema.
• ETIOPATHOGENESIS:
The two most important etiologic factors responsible for majority of cases of chronic bronchitis are:
Cigarette Smoking and Atmospheric Pollution. Other Contributory Factors Are Occupation,
Long Term Exposure to Toxic Chemicals, Chronic Infection, Familial and Genetic Factors.
8.
CLINICAL FEATURES:
There isconsiderable overlap of clinical features of chronic bronchitis and pulmonary
emphysema as quite often the two coexist.
Some important features of ‘predominant bronchitis’ are as under:
1. Persistent cough with copious expectoration of long duration; initially beginning in a
heavy smoker with ‘morning catarrh’ or ‘throat clearing’ which worsens in winter.
2. Recurrent respiratory infections are common.
3. Dyspnoea(Shortness of breath) is generally not prominent at rest but is more on
exertion.
4. Patients are called ‘blue bloaters’ due to cyanosis and oedema.
5. Features of right heart failure (cor pulmonale) are common.
6. Chest X-ray shows enlarged heart with prominent vessels.
9.
EMPHYSEMA
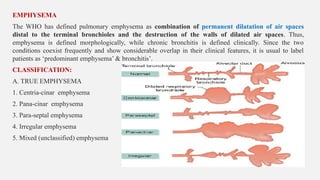
The WHO hasdefined pulmonary emphysema as combination of permanent dilatation of air spaces
distal to the terminal bronchioles and the destruction of the walls of dilated air spaces. Thus,
emphysema is defined morphologically, while chronic bronchitis is defined clinically. Since the two
conditions coexist frequently and show considerable overlap in their clinical features, it is usual to label
patients as ‘predominant emphysema’ & bronchitis’.
CLASSIFICATION:
A. TRUE EMPHYSEMA
1. Centria-cinar emphysema
2. Pana-cinar emphysema
3. Para-septal emphysema
4. Irregular emphysema
5. Mixed (unclassified) emphysema
10.
B. OVERINFLATION
1. Compensatoryover-inflation (compensatory emphysema) - Over expansion of alveoli in one part
of the lung.
2. Senile hyperinflation (aging lung, senile emphysema) – Enlargement of alveolar spaces.
3. Obstructive over-inflation (infantile lobar emphysema) – Most affected lobes.
4. Unilateral translucent lung (unilateral emphysema) – Abnormal over-inflation one lung
5. Interstitial emphysema (surgical emphysema) – Injury subcutaneous tissues
11.
• ETIOPATHOGENESIS:
• Thecommonest form of COPD is the combination of chronic bronchitis and pulmonary
emphysema. Chronic bronchitis, however, does not always lead to emphysema nor all
cases of emphysema have changes of chronic bronchitis.
• The association of the two conditions is principally linked to the common etiologic factors
— most importantly tobacco smoke and air pollutants.
• Other less significant contributory factors are occupational exposure, infection and
somewhat poorly-understood familial and genetic influences.
• However, pathogenesis of the most significant event in emphysema, the destruction of the
alveolar walls, is not linked to bronchial changes but is closely related to deficiency of
serum alpha-1-antitrypsin (α1-protease inhibitor) commonly termed protease-antiprotease
hypothesis detailed below.
12.
• Protease-antiprotease hypothesis:
•Alpha-1-antitrypsin (α-1-AT), also called α1-protease inhibitor (α-1-Pi), is a glycoprotein
that forms the normal constituent of the α1-globulin fraction of the plasma proteins on
serum electrophoresis.
• The single gene locus that codes for α-1-AT is located on the long arm of chromosome 15.
It is normally synthesized in the liver and is distributed in the circulating blood, tissue
fluids and macrophages.
• The normal function of α1-AT is to inhibit proteases and hence its name α1- protease
inhibitor. The proteases (mainly elastases) are derived from neutrophils. Neutrophil
elastase has the capability of digesting lung parenchyma but is inhibited.
• doing so by anti-elastase effect of α1-AT.
13.
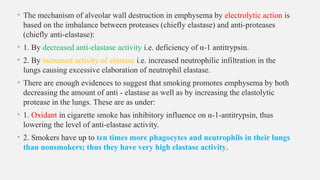
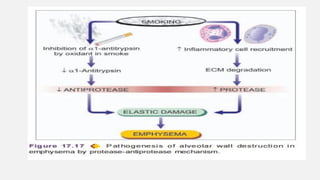
• The mechanismof alveolar wall destruction in emphysema by electrolytic action is
based on the imbalance between proteases (chiefly elastase) and anti-proteases
(chiefly anti-elastase):
• 1. By decreased anti-elastase activity i.e. deficiency of α-1 antitrypsin.
• 2. By increased activity of elastase i.e. increased neutrophilic infiltration in the
lungs causing excessive elaboration of neutrophil elastase.
• There are enough evidences to suggest that smoking promotes emphysema by both
decreasing the amount of anti - elastase as well as by increasing the elastolytic
protease in the lungs. These are as under:
• 1. Oxidant in cigarette smoke has inhibitory influence on α-1-antitrypsin, thus
lowering the level of anti-elastase activity.
• 2. Smokers have up to ten times more phagocytes and neutrophils in their lungs
than nonsmokers; thus they have very high elastase activity.
15.
Treatment of COPD:
•SMOKING CESSATION
1) Short-acting bronchodilators
1) Albuterol
2) Long-acting bronchodilator
1) Salmeterol
3) Combination of anti-cholinergic and -agonist bronchodilator
ẞ
1) Ipratropium + albuterol. 2) Tiotropium.
4) Methyl xanthines (Theophylline) Has anti-inflammatory affect and improves respiratory muscle
function, stimulates the respiratory center, and promotes bronchodilation
5) Inhaled corticosteroids
1) Fluticasone.
6) Combination of Inhaled corticosteroid and long-acting -agonist
ẞ
1) Fluticasone + salmeterol (Advair)






























![RENAL_SYSTEM[1].pptx Pathophysiology Subject B. Pharmacy First Year Sem-II](https://cdn.slidesharecdn.com/ss_thumbnails/renalsystem1-250514234559-3fde01e4-thumbnail.jpg?width=640&height=640&fit=bounds)















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














