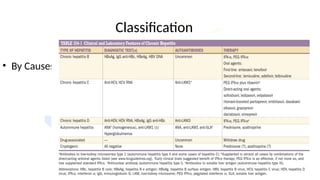
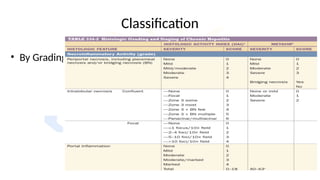
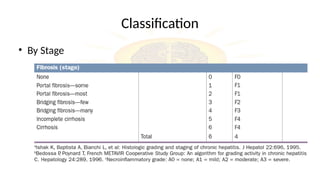
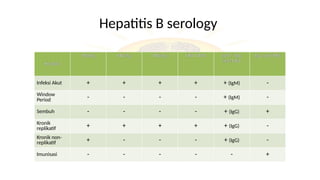
Chronic hepatitis encompasses various liver disorders with inflammation and necrosis persisting for over six months, classified mainly by cause and stage. Chronic hepatitis B can manifest with a wide range of symptoms, and its diagnosis involves serological markers and laboratory findings, while treatment options include several antiviral medications depending on the severity and replication status. Chronic hepatitis D may complicate hepatitis B without increasing the likelihood of progression to chronic disease, and treatment is focused on long-term interferon administration.


![Treatment
• Seven drugs have been approved for treatment of chronic hepatitis
B:
1. injectable interferon (IFN) α and pegylated interferon (long-
acting IFN bound to polyethylene glycol, PEG [PEG IFN]) and
2. The oral agents lamivudine, adefovir dipivoxil, entecavir,
telbivudine, and tenofovir disoproxil fumarate (TDF).
• Management of chronic hepatitis B is directed at suppressing the
level of virus replication](https://image.slidesharecdn.com/chronichepatitis-250112022027-649dc590/85/Chronic-hepatitis-chronic-hepatitis-learn-10-320.jpg)