Downloaded 209 times


![Pulmonary emboli
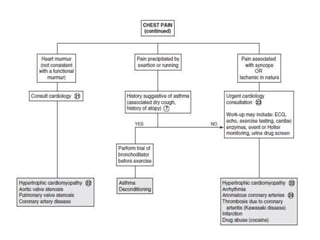
• Risk factors for venous thrombosis (e.g., oral
contraceptives, recent abortion or surgery
[especially cardiac], the presence of a central
venous line, immobilization, sepsis,
hypercoagulable states, vascular malformations)
should raise suspicion for pulmonary emboli.
• Associated symptoms include dyspnea, cough,
hypoxia, and occasionally, hemoptysis.
• If emboli are suspected, appropriate labs and
imaging (spiral CT or pulmonary angiography)
should be performed.](https://image.slidesharecdn.com/chestpaininchildren-180502225808/85/Chest-pain-in-children-21-320.jpg)
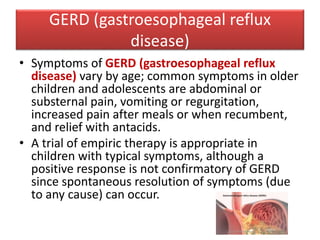
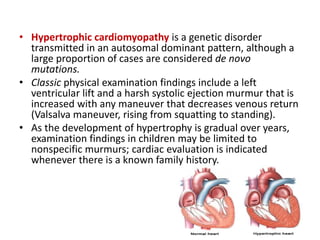
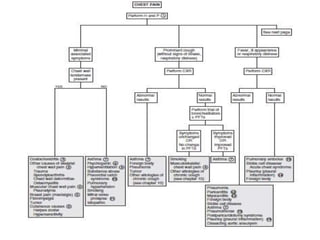

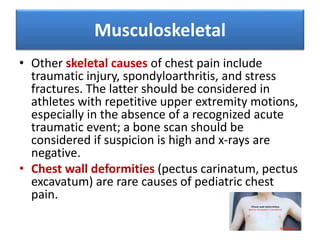
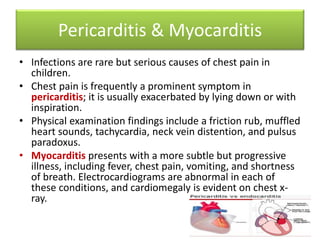
Chest pain is a common symptom in children and adolescents that is rarely due to cardiac issues. A thorough history and physical exam are usually sufficient to evaluate pediatric chest pain without screening tests. Common non-cardiac causes of chest pain in youth include musculoskeletal issues like costochondritis, respiratory problems like asthma, and psychological factors. Providers must carefully distinguish cardiac causes from non-cardiac etiologies to appropriately manage pediatric patients experiencing chest pain.























































































