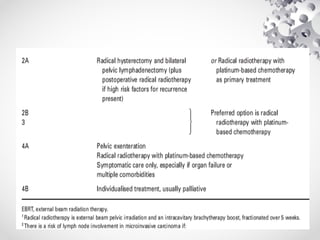
Cervical cancer is a leading cause of cancer deaths among females in Malawi, especially in those aged 15-44 years, primarily linked to HPV infection. The document details the pathophysiology, risk factors, and various management and prevention strategies, including vaccination and screening methods. Key classifications for diagnosis are provided, alongside recommended interventions and investigations for effective patient management.




















![DOC-20241220-WA0005[1].pptx screening of breast cancer](https://cdn.slidesharecdn.com/ss_thumbnails/doc-20241220-wa00051-250706171952-02b5ca46-thumbnail.jpg?width=640&height=640&fit=bounds)






























![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)








