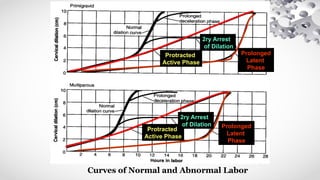
Abnormal labor is defined as any deviation from the normal progress of labor due to various factors including dysfunctional uterine activity, fetal issues, pelvic inadequacies, or maternal conditions. Diagnosis involves monitoring labor phases and recognizing patterns of protraction or arrest disorders, with management strategies typically including oxytocin administration or cesarean section if progress stalls. Risks associated with abnormal labor include maternal anxiety, fetal distress, and complications such as obstructed labor or uterine rupture.



































![ABNORMAL LABOUR[]{}#%^*+=_\|~<>€£¥•.,?!’-/:(($$&@“.,?!’pdf](https://cdn.slidesharecdn.com/ss_thumbnails/abnormallabour-240814080030-7769169f-thumbnail.jpg?width=640&height=640&fit=bounds)






























