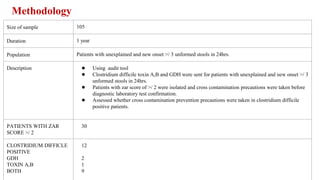
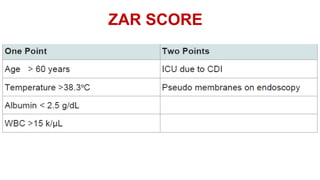
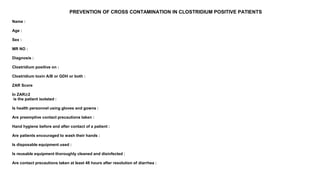
This clinical audit examines health care practices and Clostridium difficile incidence in a tertiary care unit. The aims are to initiate early isolation of C. difficile patients, educate staff on prevention precautions, and adhere to infection control guidelines. A sample of 105 patients were audited over one year. Of 30 patients with a ZAR score of 2 or higher, 12 tested positive for C. difficile. Precautions were taken for all 30 patients. The audit found that teamwork and understanding of responsibilities helped prevent C. difficile cross-contamination.