• A 23-yearsold young male was playing football
in the playground of KEMU where he was
suddenly collapse and was brought to
emergency of Mayo Hospital. The boy was
started with ACLS protocol in the emergency.
• Unfortunately, He could not be reverted, and
was declared dead.
• 1 year later, his brother who was doing his house
job, started having exertional dyspnea, he was
diagnosed to have cardiomyopathy, shifted to US
for open heart surgery. He also was found dead
one day while he was doing an exertion
3.
Constitutes agroup of diseases that
directly affect the structural or
functional ability of the myocardium
4.
Classification
Primary:
It refersto those conditions in which
the etiology of heart disease is unknown.
Secondary:
It refers that the cause of myocardial
diseases are known.
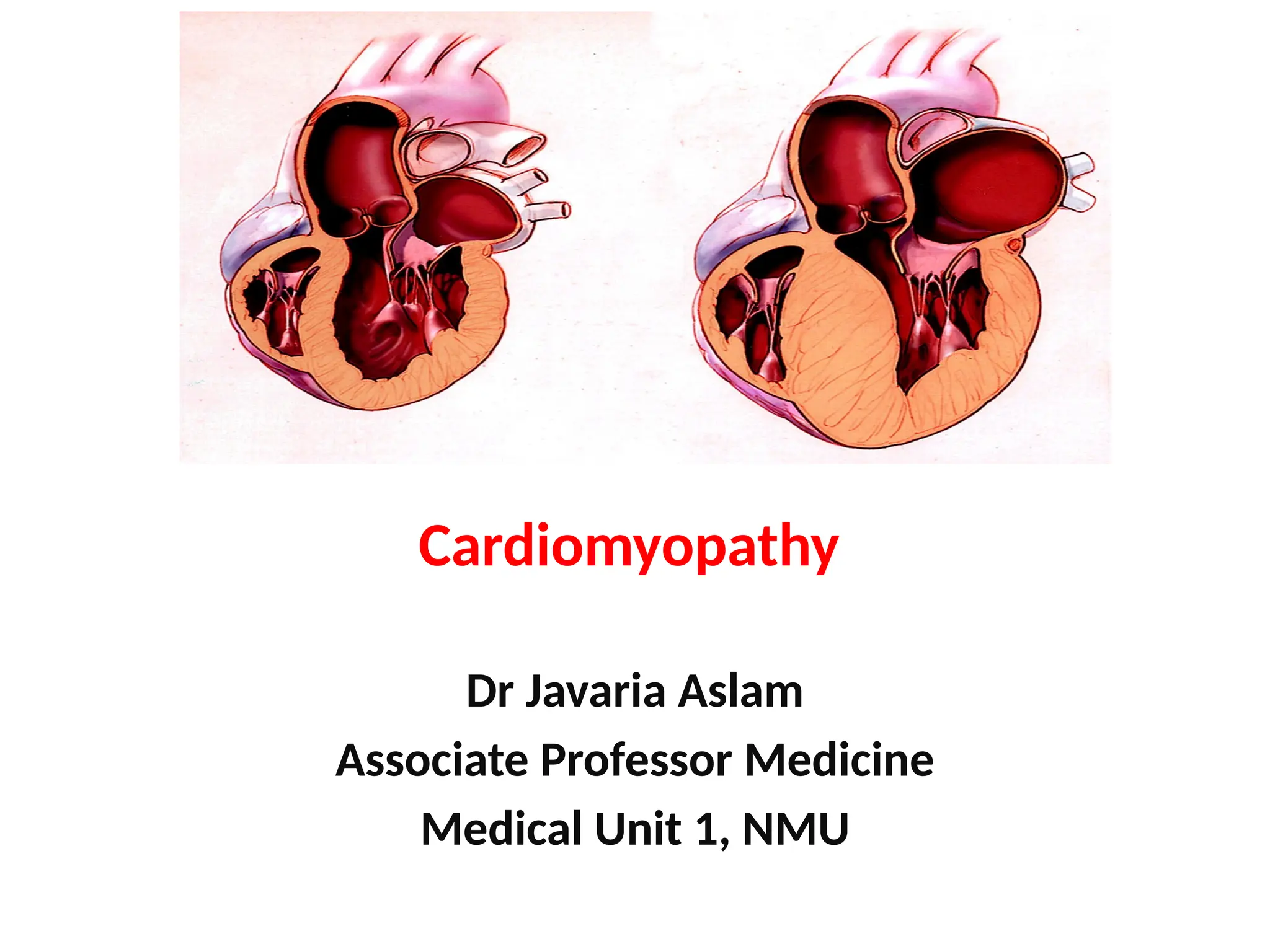
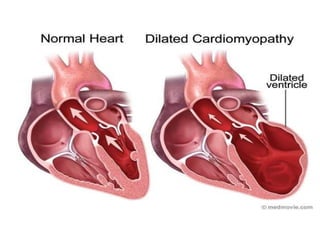
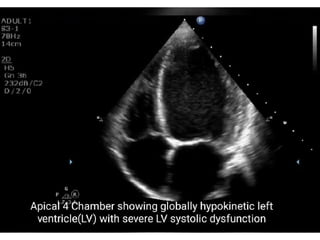
It isa condition in which the hearts
ability to pump blood OR to adjust the
incoming blood is decreased because the
left ventricle, is enlarged or weakened.
DEFINITION
8.
Characterized by diffuseinflammation and
rapid degeneration of myocardial fibers
ventricular dilation
impairment of systolic function
Atrial enlargement and stasis of blood in the
left ventricle cardiomegaly
PATHOPHYSIOLOGY
9.
Cardiotoxic agentslike alcohol or coccaine
Genetic
Hypertension
Ischemia(CAD)
Muscular dystrophy (Weakening and wasting
of muscles)
Myocarditis
Pregnancy
Valve disease
ETIOLOGY
History
Echocardiography
Chest x-ray: shows the signs of cardiomegaly
ECG: reveals tachycardia, bradycardia and
dysarrythmias.
Cardiac catheterization: it is performed to
confirm CAD
DIAGNOSTIC MEASURES
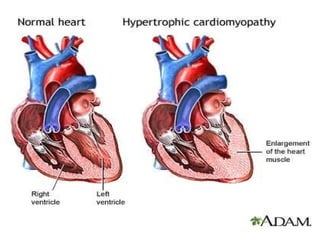
Assymetric leftventricular hypertrophy
without ventricular dilation.
When the septum between two ventricles
become enlarged and obstructs the
blood flow from left ventricle, it is
known as hypertrophic obstructive
cardiomyopathy.
HYPERTROPHY CARDIOMYOPATHY
18.
Aortic stenosis
Genetic
Hypertension
More common in men between ages 30 to
40
ETIOLOGY
19.
Thickened intra-ventricular septumand
ventricular wall
ventricular hypertrophy
diastolic
dysfunction
impaired ventricular filling and obstruction to
decreased outflow
PATHOPHYSIOLOGY
20.
Exertional dyspnea(Shortness of breath
during exercise)
Decreased cardiac output
Fatigue
Angina
Syncope
Hypertension
Cardiac MRI.A cardiac MRI uses magnetic fields
and radio waves to create images of your heart.
Cardiac MRI is often used in addition to
echocardiography in the evaluation of people
with hypertrophic cardiomyopathy.
Septal myectomy:
Itis an open heart surgical procedure
in which the surgeon removes the part
of thickened , over grown septum
between the ventricles.
SURGICAL MANAGEMENT
25.
Septal ablation:
Inthis procedure a small portion of the
thickened heart muscle is destroyed by
injecting alcohol through a long, thin
tube into the artery supplying blood to
that area.
26.
Implantable cardioverter-defibrillator(ICD):
It is recommended when the persons have life
threatening heart rhythm disorders. It is a small
instrument which can be implanted in the chest
as a pacemaker
27.
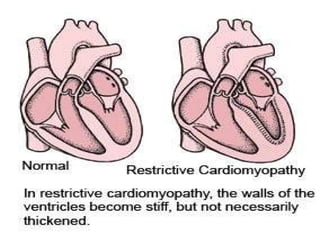
• Disease ofthe heart muscle that impairs
diastolic filling and stretch and the systolic
function remains unaffected.
RESTRICTIVE CARDIOMYOPATHY
29.
Unknown etiology
Myocardial fibrosis,
Endocardial fibrosis,
Sarcoidosis and
Radiation to the thorax
ETIOLOGY
30.
etiologic factors
Stiffness ofthe ventricular wall with loss of
ventricular compliance
Ventricles become resistant to filling
decrease cardiac output
PATHOPHYSIOLOGY
31.
Fatigue
Exerciseintolerance
Dyspnea
Orthopnea(shortness of breath (dyspnea) which occurs when
lying flat)
Syncope
Palpitations
Peripheral edema
Jugular venous distention
CLINICAL MANIFESTATIONS
32.
Chest x-ray:shows cardiomegaly
ECG: shows tachycardia
Echocardiography : for the visualization of
left ventricle
CT-Scan and MRI Scan
INVESTIGATIONS
A hearttransplantation may be
considered if the heart function is
very poor and the symptoms are
severe.
35.
Instruct thepatient to take all medicines on
prescribed time.
Encourage to use low sodium diet
Instruct to drink more water
Instruct the patient to maintain proper body
weight
Teach the patient to balance activity and
rest
Instruct the patient to avoid vigorous
activities and exercises
MANAGEMENT
36.
Encourage toperform stress reduction
activities.
Teach about breathing and coughing
exercise
Suggest the family members to learn about
CPR.
37.
• A 25years old lady presented in emergency
with worsening dyspnea for 3 weeks. He had
delivered to a baby almost 2 months ago. On
examination she had bilateral basal fine
inspiratory crackles. The JVP was raised and
there was also mild pedal edema.