
Recommended
More Related Content
Similar to Caffeine intake in children in the United States and 10-ytre.docx
Similar to Caffeine intake in children in the United States and 10-ytre.docx (20)
More from humphrieskalyn
More from humphrieskalyn (20)
Recently uploaded
Recently uploaded (20)
Caffeine intake in children in the United States and 10-ytre.docx
- 1. Caffeine intake in children in the United States and 10-y trends: 2001–20101–4 Namanjeet Ahluwalia, Kirsten Herrick, Alanna Moshfegh, and Michael Rybak ABSTRACT Background: Because of the increasing concern of the potential adverse effects of caffeine intake in children, recent estimates of caffeine consumption in a representative sample of children are needed. Objectives: We provide estimates of caffeine intake in children in absolute amounts (mg) and in relation to body weight (mg/kg) to examine the association of caffeine consumption with sociodemo- graphic factors and describe trends in caffeine intake in children in the United States. Design: We analyzed caffeine intake in 3280 children aged 2–19 y who participated in a 24-h dietary recall as part of the NHANES, which is a nationally representative survey of the US population with a cross-sectional design, in 2009–2010. Trends over time be- tween 2001 and 2010 were examined in 2–19-y-old children (n = 18,530). Analyses were conducted for all children and repeated for
- 2. caffeine consumers. Results: In 2009–2010, 71% of US children consumed caffeine on a given day. Median caffeine intakes for 2–5-, 6–11-, and 12– 19-y olds were 1.3, 4.5, and 13.6 mg, respectively, and 4.7, 9.1, and 40.6 mg, respectively, in caffeine consumers. Non-Hispanic black chil- dren had lower caffeine intake than that of non-Hispanic white counterparts. Caffeine intake correlated positively with age; this association was independent of body weight. On a given day, 10% of 12–19-y-olds exceeded the suggested maximum caffeine intake of 2.5 mg/kg by Health Canada. A significant linear trend of decline in caffeine intake (in mg or mg/kg) was noted overall for children aged 2–19 y during 2001–2010. Specifically, caffeine in- take declined by 3.0 and 4.6 mg in 2–5- and 6–11-y-old caffeine consumers, respectively; no change was noted in 12–19-y-olds. Conclusion: A majority of US children including preschoolers con- sumed caffeine. Caffeine intake was highest in 12–19-y-olds and remained stable over the 10-y study period in this age group. Am J Clin Nutr 2014;100:1124–32. INTRODUCTION Caffeine is a commonly consumed stimulant present naturally in or added to foods and beverages. Caffeine consumption in children has received considerable interest because of the con- cern of adverse health effects. Caffeine intake of 100–400 mg has been associated with nervousness, jitteriness, and fidgetiness
- 3. (1, 2). Because of the continued brain development involving myelination and pruning processes, children may be particularly sensitive to caffeine (3, 4). There has been some evidence that has linked caffeine intake in children to sleep dysfunction, el- evated blood pressure, impairments in mineral absorption and bone health, and increased alcohol use or dependence (1, 5–7). In addition, the routine use of caffeinated sugar-sweetened beverages may contribute to weight gain and dental cavities (8). Caffeine toxicity in children has also been described involving tachycardia, central nervous system agitation, gastrointestinal disturbance, and diuresis (6, 9, 10). Health Canada has put forth maximal daily caffeine intake guidelines for children and ado- lescents (6, 11). Although no such recommendations have been set in the United States, the American Academy of Pediatrics has underscored that “caffeine and other stimulant substances contained in energy drinks have no place in the diet of children” (12). Caffeine consumption has also been associated with certain health benefits such as increased endurance, attention, and vig- ilance and a reduced reaction time in some studies (9, 13, 14). Perceived positive effects on mood and cognition as well as physical performance may encourage preteens and adolescents to consume caffeinated products (2, 15, 16). The literature on caffeine consumption in a representative sample of US children has been primarily based on older data, namely the US Department of Agriculture Continuing Survey of Food Intakes by Individuals (CSFII)5 1994–1996 and 1998 (16, 17). In addition, caffeine intake from beverages from the 1999 US Share of Intake Panel (SIP) survey in caffeine consumers has also been published (18). A 2010 US Food and Drug Admin- istration report also presented findings from the analysis of
- 4. older data from NHANES 2005–2006 (19). Because of the current 1 From the Division of Health and Nutrition Examination Surveys, Na- tional Center for Health Statistics, CDC, Hyattsville, MD (NA and KH); the National Center for Environmental Health, CDC, Atlanta, GA (MR); and the Food Surveys Research Group, Beltsville Human Nutrition Research Center–Agricultural Research Service, USDA, Beltsville, MD (AM). 2 Findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Center for Health Statistics, CDC. 3 This work was not supported by any external grant. 4 Address correspondence to N Ahluwalia, Division of Health and Nutri- tion Examination Surveys, National Center for Health Statistics, CDC, 3311 Toledo Road, Room 4110, Hyattsville, MD 20782. E-mail: [email protected] cdc.gov. 5 Abbreviations used: CSFII, Continuing Survey of Food
- 5. Intakes by In- dividuals; MEC, mobile examination center; PIR, poverty income ratio; SIP, Share of Intake Panel. ReceivedDecember 19, 2013. Accepted for publication July 3, 2014. First published online August 27, 2014; doi: 10.3945/ajcn.113.082172. 1124 Am J Clin Nutr 2014;100:1124–32. Printed in USA. � 2014 American Society for Nutrition D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 debate on the safety of caffeine intake by children (1, 12, 18) and deliberations to evaluate maximal intake recommendations, it is important to describe caffeine intake from more recent data available on a nationally representative sample such as the NHANES. Trends in beverage consumption have changed over time (16,
- 6. 20), and several caffeinated beverages and energy drinks have been introduced in the past decade, some marketed especially to youth (12, 15, 16). Few reports have described trends in caffeine intake both in milligrams and milligrams per kilogram of body weight by age in the United States (16, 21). Thus, our objective was to provide estimates of the distribution of caffeine intake in absolute amounts and in milligrams per kilogram in a representative sample of American children (2–19 y old) by using the most recent di- etary data available from the NHANES (ie, 2009–2010) in re- lation to demographic characteristics and examine the trends in caffeine consumption between 2001 and 2010 in children. SUBJECTS AND METHODS Study design The NHANES is a series of large, complex, stratified, multistage probability surveys of the US civilian, noninstitutionalized pop- ulation conducted by the National Center for Health Statistics, CDC (22). Briefly, NHANES is conducted yearly in w5000 individuals, and data are publicly released every 2 y on w10,000 individuals. Participants in the NHANES are administered a se- ries of questionnaires in a detailed in-home interview followed by a scheduled visit at the mobile examination center (MEC). At the MEC visit, participants receive a physical examination as well as a dietary interview, which is commonly referred to as the What We Eat in America component of the NHANES. The NHANES protocol was approved by the National Center for Health Statistics’s Research Ethics Review board. Informed
- 7. consent was obtained from persons aged $18 y. For participants ,18 y of age, written parental consent was obtained, and child assent was obtained for individuals from 7 to 17 y of age. The most recent available data on caffeine intake from the NHANES (from the 2009–2010 survey) were used for the current analysis to describe caffeine consumption by demographic characteris- tics; data from this single survey cycle were sufficient to provide stable national estimates. We used NHANES data from 2001 to 2010 (2001–2002, 2003–2004, 2005–2006, 2007–2008, and 2009–2010 survey cycles) to conduct the trends analysis; be- cause of changes in the dietary data collection methodology on merging of the CSFII with NHANES in 1999–2000, data from 1999 to 2000 were not included in the trends analysis. The un- weighted total examination response rate for the 5 survey cycles examined for participants 2–19 y of age ranged from 81% to 88% (23). Dietary interview The type and quantity of all foods and beverages consumed in a single 24-h period, specifically the 24-h period before the dietary interview (from midnight to midnight) at the MEC, were collected by trained interviewers with the use of a computer- assisted dietary interview system with standardized probes (ie, the USDA’s Automated Multiple-Pass Method). Specifically for beverages for which caffeine may be removed such as soda, coffee, tea, and energy drinks, probes were used to ascertain if the bev- erage reported was caffeine free. The Automated Multiple-Pass Method is designed to enhance a complete and accurate data collection while reducing the respondent burden (24, 25). For children aged #5 y, interviews were obtained through proxies, generally a parent. Proxies also assisted with dietary interviews
- 8. of children aged 6–11 y. Dietary intakes were self-reported for participants aged $12 y. Since 2003–2004, a second, telephone- administered 24-h recall has been collected (3–10 d after the first 24-h recall at the MEC), but only one 24-h dietary recall was included in this analysis to maximize the comparability between surveys. Furthermore, one 24-h recall is sufficient to estimate population means because the effects of random errors associ- ated with dietary recall, including the day-to-day variability, are generally assumed to cancel out if days of the week are evenly represented (26). Caffeine intake for all foods and beverages (including energy drinks) consumed during the 24-h period was calculated by using the USDA Food and Nutrient Database for Dietary Studies (27). The basis of nutrient values for foods and beverages, such as energy drinks, is the USDA National Nutrient Database for Standard Reference. Sources of nutrient data include scientific literature, data provided by food companies and trade associa- tions, and USDA analytical contracts. Caffeine intake was es- timated by summing the caffeine consumed for each food and beverage during the 24-h recall. Demographic variables Sex, age, race-Hispanic origin, and poverty income ratio (PIR) were used. Age was categorized as 2–5, 6–11, and 12–19 y TABLE 1 Percentage of US children aged 2–19 y old who consumed caffeine on a given day by demographic characteristics: NHANES 2009– 2010
- 9. 1 Characteristic n (% 6 SE) P All children 3280 (71.0 6 1.0) — Age ,0.01 2–5 y 861 (58.3 6 2.4) 6–11 y 1154 (74.9 6 1.7) 12–19 y 1265 (74.5 6 2.2) Sex NS M 1712 (70.6 6 1.9) F 1568 (71.5 6 1.3) Poverty income ratio2 NS #130% 1422 (70.0 6 1.8) 131–349% 1023 (74.2 6 1.9) $350% 555 (69.6 6 2.7) Race-Hispanic origin3 ,0.001 Non-Hispanic white 1101 (74.9 6 1.8)a Non-Hispanic black 654 (56.3 6 2.2)b Mexican American 914 (71.7 6 2.0)a 1 NS at P $ 0.05. A test of linear trend was used for ordinal variables (age and poverty income ratio) and Wald’s F test was used for sex and race- Hispanic origin; significance was set at P , 0.05. Different superscript
- 10. letters represent a significant difference between categories compared by using the t test adjusted with the Bonferroni method for multiple compari- sons. 2 Index calculated by dividing family income by a federal poverty threshold specific to family size defined by the US Census Bureau. 3 “Other” race category not shown. CAFFEINE INTAKE IN US CHILDREN 1125 D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 consistent with NHANES sample-selection methods (28). Self- reported race-Hispanic origin was categorized as non-Hispanic white, non-Hispanic black, Mexican American, and other. Par- ticipants with a race-Hispanic origin categorized as other were included in overall estimates, but findings from this group are not reported (because of the small sample size and unstable variance estimates for a very heterogeneous group). Socioeco-
- 11. nomic status was defined by using the PIR, which is an index calculated by dividing family income by a federal poverty threshold specific to family size defined by the US Census Bu- reau (29). The PIR was categorized as #130%, 131–349%, and $350%; for reference, a family income that corresponds to a 130% PIR qualifies for the Supplemental Nutrition Assistance Program (formerly the Food Stamp Program) and free school meals (30). Analytic population All children and adolescents aged 2–19 y who participated in the examination component of the NHANES were eligible for the dietary interview. In each survey cycle, a small proportion (4–6%) of participants were excluded because their 24-h recalls did not meet the standards of reliability that ensure the com- pleteness of recalls (31). In addition, 5 children who were re- portedly breastfed during the 24-h recall were excluded from the analysis because their caffeine intakes from breast milk could not be ascertained. The final analytic sample, after exclusions, comprised 4288, 3824, 4029, 3159, and 3280 participants aged 2–19 y in 2001–2002, 2003–2004, 2005–2006, 2007–2008, and 2009–2010, respectively. Data analysis Statistical analyses were conducted with SAS software (version 9.3; SAS Institute Inc) and SUDAAN software (version 11.0; RTI International). Caffeine intake on a given day was examined in absolute amounts (mg) and in relation to body weight (mg/kg) in all analyses. Caffeine intake displayed a skewed distribution; w30% of the analytic population did not report any caffeine in- take during the 24-h recall period. Thus, logarithmically (base
- 12. 10) transformed data on caffeine intake were used to test statistical hypotheses because they were identified (by using the Box-Cox procedure in SAS) to be more consistent with a normal distri- bution (32, 33). To accommodate respondents who reported no caffeine consumption on the day of recall, caffeine intakes of zero were set to 0.0001 to allow the log base 10 transformation. Ex- treme values were examined to determine whether they exerted undue influence. Plots of dietary sample weight compared with caffeine intake showed that extreme values were not associated with influential weights. Preliminary analyses indicated that the exclusion of these extreme values did not change the results; thus, no exclusions or corrections were made. Dietary sample weights were used to account for a differential probability of selection and adjust for nonresponse, noncoverage, and sample design. These publically available sample weights also include a poststratification step to balance recalls across days of the week (31). Weighted, untransformed estimates of the 50th (median), 75th, 90th, and 95th percentiles and percentages (6SEs) were com- puted for children and adolescents (aged 2–19 y) by demo- graphic characteristics. Statistical hypotheses regarding the TABLE 2 Caffeine intake on a given day by demographic characteristics for US children 2–19 y old: NHANES 2009–2010 1 Characteristics
- 13. Caffeine Pn Median2 75th percentile 90th percentile 95th percentile mg/d All children 3280 4.6 30.8 94.6 147.6 — Age ,0.0001 2–5 y 861 1.3 5.9 13.4 23.8 6–11 y 1154 4.5 19.2 49.7 72.3 12–19 y 1265 13.6 70.9 147.9 260.5 Sex NS M 1712 4.7 30.0 102.1 169.5 F 1568 4.5 31.3 85.1 132.5 Poverty income ratio 3 NS #130% 1422 4.5 30.2 77.4 131.7 131–349% 1023 5.5 36.4 106.5 141.9 $350% 555 3.6 26.5 88.9 153.0 Race-Hispanic origin 4 ,0.0001
- 14. Non-Hispanic white 1101 6.4 a 43.2 112.0 177.9 Non-Hispanic black 654 1.3b 9.7 55.2 93.1 Mexican American 914 4.2a 22.7 70.3 112.8 1 Medians and percentiles were calculated from untransformed weighted data; 5th and 25th percentiles are not presented and were essentially equal to zero because of a high proportion of children who did not consume any caffeine. A test of linear trend was used for ordinal variables age and poverty income ratio. Wald’s F test was used for sex and race- Hispanic origin. Significance was set at P , 0.05. Different superscript letters represent a significant difference between categories compared by using the t test adjusted with the Bonferroni method for multiple comparisons. 2 All statistical tests were performed on log-transformed means. 3 Index calculated by dividing family income by a federal poverty threshold specific to family size defined by the US Census Bureau. 4 “Other” race category not shown. 1126 AHLUWALIA ET AL D ow
- 15. nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 proportion of children who consumed caffeine in relation to sociodemographic variables were tested on weighted, untrans- formed percentages. Hypotheses concerning caffeine intake (mg and mg/kg) in relation to sociodemographic variables were tested by using weighted means of the log-transformed variable. SEs were estimated by using Taylor’s series linearization. Statistical hypotheses were tested by using Wald’s F tests with a = 0.05. If the hypothesis that the mean or percentage of all subgroups being equal was rejected, pairwise t tests were performed. An adjustment for multiple comparisons was made by using the Bonferroni method (34). Linear trends in log-transformed caffeine intake by age and PIR were determined by using orthogonal contrast matrices (35). We also tested for linear trends in log- transformed caffeine intake across the survey periods between 2001 and 2010 by using orthogonal contrast matrices (35); tests were conducted for all children and within age groups over time. Analyses were carried out for all children in the analytic population and re- peated for children who consumed caffeine (consumers only). For the purpose of the current analyses, caffeine consumers
- 16. were defined as children who reported the consumption of caffeine on the 24-h dietary recall. RESULTS A majority (71%) of 2–19-y-olds consumed caffeine on a given day (Table 1). A linear trend was noted in the proportion of 2–19-y-olds who consumed caffeine with age but not PIR. No differences were seen between males and females in terms of the proportion of children who consumed caffeine. However, dif- ferences were noted in caffeine consumption by race-Hispanic origin as follows: non-Hispanic black children (56%) were less likely to consume caffeine than were non-Hispanic white (75%) or Mexican American (72%) children (Table 1); however, no differences between non-Hispanic white or Mexican American children were noted. The distribution of caffeine intake (mg) on a given day by selected demographic characteristics (Table 2) showed that the median caffeine intake by US children 2–19 y of age was 4.6 mg. An increasing linear trend in caffeine intake was noted by age. No significant associations were shown between the PIR and caffeine intake. Non-Hispanic black children consumed significantly less caffeine than did non-Hispanic white or Mexican American children (Table 2). No differences in caffeine intake between non-Hispanic white and Mexican American children were noted. When these analyses were restricted to children who con- sumed caffeine (ie, consumers only) (Table 3), the median caffeine intake on a given day was 12.4 mg. The significant
- 17. linear trend for caffeine intake and age remained, with the oldest age group (12–19-y-olds) having the highest caffeine intake (40.6 mg). Non-Hispanic black children consumed significantly less caffeine (8.0 mg) than did non-Hispanic white children (14.4 mg) (Table 3). No other racial-ethnic group differences were noted. When caffeine intake (mg) was expressed in relation to body weight (kg), the median caffeine consumption for US children 2–19 y of age was 0.15 mg/kg (Table 4). Associations of caffeine intake (mg/kg) with age and race-Hispanic origin were similar TABLE 3 Caffeine intake in consumers of caffeine on a given day by demographic characteristics for US children 2–19 y old: NHANES 2009–2010 1 Characteristics Caffeine Pn Median2 75th percentile 90th percentile 95th percentile mg All children 2230 12.4 52.2 116.6 184.0 — Age ,0.0001 2–5 y 485 4.7 10.3 20.9 36.1 6–11 y 826 9.1 31.4 58.5 85.3
- 18. 12–19 y 919 40.6 96.6 186.3 284.4 Sex NS M 1154 12.1 56.2 124.0 223.6 F 1076 12.6 49.0 105.3 148.0 Poverty income ratio3 NS #130% 952 14.3 51.6 98.9 155.3 131–349% 717 11.6 55.4 119.4 184.2 $350% 382 9.5 48.7 113.3 204.4 Race-Hispanic origin 4 ,0.01 Non-Hispanic white 819 14.4 a 60.1 137.3 220.2 Non-Hispanic black 367 8.0b 41.3 89.4 109.6 Mexican American 633 11.6a,b 42.5 91.5 131.5 1 Medians and percentiles were calculated from untransformed weighted data. A test of linear trend was used for ordinal variables age and poverty income ratio. Wald’s F test was used for sex and race-Hispanic origin. Significance was
- 19. set at P , 0.05. Different superscript letters represent a significant difference between categories compared by using the t test adjusted with the Bonferroni method for multiple comparisons. 2 All statistical tests were performed on log transformed means. 3 Index calculated by dividing family income by a federal poverty threshold specific to family size defined by the US Census Bureau. 4 “Other” race category not shown. CAFFEINE INTAKE IN US CHILDREN 1127 D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 as noted for caffeine intake in absolute amounts (mg). Non- Hispanic black children had significantly lower caffeine intake (0.04 mg/kg) than did other race-ethnicities examined (Table 4). When analyses of caffeine intake (mg/kg) were restricted to
- 20. children who consumed caffeine, (ie, consumers only) (Table 5), the median caffeine intake was 0.40 mg/kg on a given day. A linear trend in caffeine intake (mg/kg) with age was again observed. As for the results concerning the absolute amount (mg) of caffeine ingested in consumers only, the finding that non-Hispanic black children consumed significantly lower caffeine (0.24 mg/kg) than did non-Hispanic white children (0.47 mg/kg) remained unaltered (Table 5). No other race-ethnic differences were noted. Caffeine intake did not differ by sex or poverty level whether expressed as total intake (mg) or in relation to body weight (mg/kg) for all children 2–19 y of age or in caffeine consumers 2–19 y of age (Tables 2–5). We estimated 90th and 95th percentiles of caffeine intake by various sociodemographic factors to provide national estimates that may be useful for policy makers in future evaluations of the upper end of the distribution. As expected, the 90th percentile of caffeine intake (mg) was lower in all children than caffeine consumers (Tables 2 and 3, respectively). Health Canada has put forth maximal caffeine intake (mg) guidelines for children that vary by age; specifically, 45, 62.5, and 85 mg caffeine/d have been suggested as maximum caffeine intakes for 4–6-, 7–9-, and 10–12-y-olds, respectively (11). Our analyses show that most (90–95%) children ,12 y old had caffeine intakes below these guidelines (Tables 2 and 3). For older children, caffeine con- sumption guidance has been based on milligrams per kilogram of body weight; Health Canada has suggested that daily caffeine intake for children .12 y of age should be ,2.5 mg/kg (6, 11).
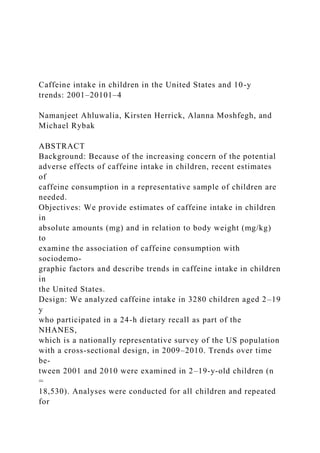
- 21. Our findings indicated that 90% of children 12–19 y of age and $75% and ,90% of 12–19-y-old caffeine consumers on a given day met these guidelines and had caffeine intakes ,2.5 mg $ kg21 $ d21 (Tables 4 and 5, respectively). We also examined trends in caffeine intake from 2001 to 2010. The caffeine intake in 2–19-y-old children decreased overall in the 10-y study period for all children (Figure 1A; n = 18,530 and P , 0.05) and caffeine consumers only (Figure 1B; n = 12,776 and P , 0.001). No major trends were noted for specific age groups in all children (caffeine consumers and non- consumers) (Figure 1A). However, when trends analyses were restricted to caffeine consumers only, 2–5- and 6–11-y-olds showed a significant decrease in caffeine intakes from 2001– 2002 to 2009–2010 (Figure 1B; P-trend , 0.001 for both age groups); the magnitude of these changes, however, was small, by 3.0 and 4.6 mg in children 2–5 and 6–11 y of age, respectively. Identical findings were noted with caffeine intake expressed as milligrams per kilogram of body weight (data not shown) for all children (consumers and nonconsumers of caffeine) as well as for children who consumed caffeine. DISCUSSION Caffeine intake in children has received much attention be- cause of potential adverse health effects (1, 2, 10, 36). Most TABLE 4 Caffeine intake in relation to body weight on a given day by demographic characteristics for US children 2–19 y old: NHANES 2009–20101 Caffeine
- 22. Characteristic n Median2 75th percentile 90th percentile 95th percentile P mg/kg All children 3280 0.15 0.75 1.78 2.70 — Age ,0.01 2–5 y 861 0.11 0.36 0.86 1.43 6–11 y 1154 0.15 0.62 1.68 2.49 12–19 y 1265 0.22 1.13 2.45 3.27 Sex NS M 1712 0.15 0.72 1.83 2.98 F 1568 0.15 0.80 1.69 2.58 Poverty income ratio3 NS #130% 1422 0.15 0.77 1.71 2.76 131–349% 1023 0.17 0.86 1.87 2.70 $350% 555 0.13 0.63 1.47 2.44 Race-Hispanic origin4 ,0.001 Non-Hispanic white 1101 0.19 a 0.90 2.09 3.02 Non-Hispanic black 654 0.04
- 23. b 0.28 1.07 1.55 Mexican American 914 0.14a 0.65 1.47 2.21 1 Medians and percentiles were calculated from untransformed weighted data. Fifth and 25th percentiles are not presented and were essentially equal to zero because of a high proportion of children who did not consume any caffeine. A test of linear trend was used for ordinal variables age and poverty income ratio. Wald’s F test was used for sex and race- Hispanic origin. Significance was set at P , 0.05. Different superscript letters represent a significant difference between categories compared by using the t test adjusted with the Bonferroni method for multiple comparisons. 2 All statistical tests were performed on log transformed means. 3 Index calculated by dividing family income by a federal poverty threshold specific to family size defined by the US Census Bureau. 4 “Other” race category not shown. 1128 AHLUWALIA ET AL D ow nloaded from
- 24. https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 healthy persons tolerate caffeine well; however, there is a large variation in individuals in their responses to caffeine (37, 38). Estimates of caffeine consumption in a nationally representative sample of young children that were based on recent data may be informative for updating recommendations. To our knowledge, this is the first report of caffeine intake in US children aged 2– 19 y, which was examined both in absolute amount (mg) and milli- grams per kilogram of body weight, and its associations with sociodemographic factors from the most-recent available na- tional data from NHANES 2009–2010. In addition, trends in caffeine consumption (both in mg and mg/kg) over a decade (2001–2010) are reported for the first time to our knowledge. In the current study, 71% of US children aged 2–19 y con- sumed caffeine on a given day. Our finding that 58% of 2–5-y- olds and 75% of 6–11-y-olds consumed caffeine on a given day was lower than estimates reported by Frary et al (16) on the basis of older national data from the CSFII in these age groups. In that study, 76% of 2–5-y-olds and 86% of 6–11-y-olds con- sumed caffeine. For older children, Frary et al (16) reported that 91 and 88% of 12–17-y-old boys and girls, respectively, con- sumed caffeine on a given day. Because of differences in ages reported, no direct comparison could be made for older children. We showed that over one-half of US children aged 2–5 y and 3
- 25. in 4 children aged $6 y consumed caffeine on a given day. This finding is important because food habits are formed early and continue into later years and in light of the American Academy of Pediatrics recommendation that “caffeine and other stimulant substances contained in energy drinks have no place in the diet of children” (12). We noted a positive linear trend between age and caffeine consumption (expressed as mg or mg/kg) as has been reported in other studies (16, 18, 19, 39). This association may be driven by biological changes such as disrupted sleep rhythm in puberty (40) as well as psychosocial factors including a greater autonomy in beverage purchase and consumption, peer pressure, and desire for enhanced academic or physical performance (1, 15, 41, 42). Limited comparative estimates of caffeine intake are available from large representative studies (16, 18, 19, 43). Besides dif- ferences in study designs, methodologies, time periods, and the use of different age and sex groups, an additional complexity arises because most studies have reported mean intakes (despite a skewed distribution for caffeine). For comparison purposes, we computed mean caffeine intakes (6SEs) for 2–5-, 6–11-, and 12–19-y-olds. These intakes were 5.8 6 0.45, 17.2 6 1.1, and 58.3 6 6.4 mg, respectively, in all children and 10.0 6 1.0, 23.0 6 1.4, and 78.3 6 7.4 mg, respectively, in caffeine con- sumers. These estimates are similar to those reported for the NHANES 2005–06 (19) but lower than those reported for caffeine consumers in the SIP survey (1-5-y olds: 13.5 mg/d) (18) and the CSFII in middle to late 1990s (2–5-y-olds: 16 mg) (16). Caffeine is generally regarded as a safe substance; however, the US Food and Drug Administration has suggested the use of the .90th percentile to indicate a “heavy consumption” of
- 26. caffeine (18, 19). Our results showed that, in adolescents ages 12–19 y, caffeine intake at the 90th percentile was 2.45 mg/kg. This intake is identical to the maximal consumption limit sug- gested for children by Health Canada (6, 11) that was based on reported behavioral effects (44). On the basis of the NHANES TABLE 5 Caffeine intake in relation to body weight on a given day in caffeine consumers by demographic characteristics for US children 2–19 y old: NHANES 2009–20101 Characteristic n Caffeine PMedian2 75th percentile 90th percentile 95th percentile mg/kg All children 2230 0.40 1.13 2.27 3.18 — Age ,0.01 2–5 y 485 0.29 0.62 1.34 1.34 6–11 y 826 0.30 0.90 1.80 2.77 12–19 y 919 0.64 1.47 2.66 3.65 Sex NS M 1154 0.39 1.18 2.49 3.26 F 1076 0.40 1.09 2.11 2.77
- 27. Poverty income ratio3 NS #130% 952 0.44 1.10 2.19 3.47 131–349% 717 0.43 1.24 2.46 3.04 $350% 382 0.31 0.86 1.79 3.10 Race-Hispanic origin4 ,0.01 Non-Hispanic white 819 0.47 a 1.32 2.58 3.28 Non-Hispanic black 367 0.24 b 0.74 1.46 1.86 Mexican American 633 0.35a,b 0.93 1.81 2.56 1 Medians and percentiles were calculated from untransformed weighted data. A test of linear trend was used for ordinal variables age and poverty income ratio. Wald’s F test was used for sex and race-Hispanic origin. Significance was set at P , 0.05. Different superscript letters represent a significant difference between categories compared by using the t test adjusted with the Bonferroni method for multiple comparisons. 2 All statistical tests were performed on log transformed means.
- 28. 3 Index calculated by dividing family income by a federal poverty threshold specific to family size defined by the US Census Bureau. 4 “Other” race category not shown. CAFFEINE INTAKE IN US CHILDREN 1129 D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 2009–2010, we showed that 10% of children 12–19 y of age consumed .2.5 mg caffeine/kg on a given day and ,25% of 12–19-y-old caffeine consumers had intakes greater than this guideline. Children may metabolize caffeine differently than adults do (18) and show a large variation in body weight across childhood, and recommendations to limit caffeine intake have been based on body weight for children by Health Canada (6, 11). Few reports have examined caffeine intake in children expressed as milli- grams per kilogram, and they presented findings in caffeine consumers only (16, 18, 21, 43). Thus, there has been no
- 29. comparative literature on caffeine consumption in all children (caffeine consumers and nonconsumers) as has been provided in this study. Our estimates of caffeine intake (mg/kg) in caffeine consumers were generally lower than those previously reported (16, 18, 21). Frary et al (16), on the basis of older CSFII data, reported 0.4, 0.4, 0.5, and 0.6 mg/kg for 2–5-, 6–11-, and12–17-y-old boys and 12– 17-y-old girls, respectively, compared with our estimates of 0.3 mg/kg for 2–5- and 6–11-y-olds. Barone and Roberts (21) re- viewed studies up to the early 1990s and showed that caffeine intake (mg/kg) declined between 1975 and 1989. Our finding of a significant linear decreasing trend from 2001 to 2010 sug- gested that this trend has likely continued since that report (21) and could explain our lower estimates. We also examined sociodemographic patterns in caffeine consumption related to race-Hispanic origin and income. Our finding that non-Hispanic black children consumed significantly less caffeine than that of non-Hispanic white children was consistent with findings from the Bogalusa study (39) and CSFII (17). However, to our knowledge, this is the first report to show higher caffeine intake by Mexican American compared with non- Hispanic black 2–19-y-olds. In the current study, we did not find any difference in caffeine intake in relation to socioeconomic status that was contrary to findings from a small study that in- volved 24–32-mo-old children (45). Other authors have reported lower caffeine intakes by female than male children (46); this difference was more pronounced particularly at older ages (16,
- 30. 19). However, we did not find a significant association with sex, which was consistent with findings from the SIP survey (18). FIGURE 1. Trends over time in caffeine intake on a given day (mg) in US children aged 2–19 y: 2001–2010. Trends are shown for all children aged 2–19 y (A) (n = 18,530) and caffeine consumers aged 2–19 y (B) (n = 12,776). P-linear trend , 0.05 by using the t statistic for all children 2–19 y of age (A); NS for specific age groups (A). P-linear trend , 0.001 by using the t statistic for caffeine consumers 2–19 y of age, and P-linear trend , 0.001 for both 2–5- and 6– 11-y-old groups (B). Error bars represent 6 1 SE; bars capped by diamonds, circles, dashes, and triangles represent variations for all (solid line), 2–5-y-old (dashed and dotted line), 6–11-y-old (dotted line), and 12–19-y- old (dashed line) children, respectively. 1130 AHLUWALIA ET AL D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 Overall, findings for the association of caffeine intake with sociodemographic factors were consistent whether caffeine in-
- 31. take was expressed as an absolute amount or in milligrams per kilogram. Moreover, results were similar when analyses were conducted with all children or consumers only. The only ex- ception was that differences in caffeine intake by race-Hispanic origin were less prominent in consumers only. Specifically, caffeine intake of non-Hispanic black and Mexican American children was no longer different in consumers. Last, our results from the trend analysis showed a significant, albeit small, decline over the 10-y study period (2001–2010) in caffeine intake in all children and caffeine consumers only re- gardless of how caffeine intake was expressed (ie, mg or mg/kg). The decrease in caffeine intake (mg) observed over this period was significant only in younger caffeine consumers (ages ,12 y), which suggested that caffeine intake by adolescents (aged 12–19 y) who consumed the highest amounts of caffeine in all age groups examined remained stable over the 10-y study pe- riod. In view of an increasing choice of products that contain caffeine such as energy drinks targeted to youth, another pos-
- 32. sibility is that children may be replacing some of their caffeine intakes from sodas by other caffeinated products such as energy drinks. This hypothesis fits well with the findings from the NHANES that showed a decrease in soda along with a signifi- cant increase in energy or sport-drink consumption in 2–19-y- olds (20). The NHANES design allows the estimation of caffeine con- sumption on a representative sample and examination of the association of caffeine consumption with sociodemographic factors including race-Hispanic origin. The continuous nature of the NHANES since 1999 offers the possibility of evaluating trends over time from different survey cycles that used the same data-collection methodology and are linked to nutrient data banks that are updated periodically to capture new products introduced during the survey years. The current analyses were based on a single 24-h recall that was sufficient to estimate population- level estimates because random errors associated with a dietary recall, including the day-to-day variability, can be generally
- 33. assumed to cancel out if days of the week are evenly represented (26). The database used in this study did not include caffeine intake from herbals, supplements including energy shots, or medications. In conclusion, this study provides updated national estimates of caffeine intakes in children that may be useful in the context of the mounting evidence of adverse health effects associated with high caffeine intake while balancing benefits of caffeine. Future research should identify the contribution of specific foods and beverages to caffeine intake as well as the chief sources of caffeine in children and adolescents. We are grateful to Margaret Carroll for her expert guidance with the sta- tistical analysis. The authors’ responsibilities were as follows—NA: was responsible for the concept development, supervision of the statistical analysis, and writing of the manuscript; KH: conducted the statistical analysis and assisted with
- 34. preparing the tables and figure; NA and KH: were responsible for the final content of the manuscript; and all authors: provided input on the writing of the manuscript and reviewed and provided critical feedback on the manu- script. None of the authors had a conflict of interest. REFERENCES 1. Temple JL. Caffeine use in children: what we know, what we have left to learn, and why we should worry. Neurosci Biobehav Rev 2009;33: 793–806. 2. Temple JL, Dewey AM, Briatico LN. Effects of acute caffeine admin- istration on adolescents. Exp Clin Psychopharmacol 2010;18:510–20. 3. De Bellis MD, Keshavan MS, Beers SR, Hall J, Frustaci K, Masalehdan A, Noll J, Boring AM. Sex differences in brain maturation during childhood and adolescence. Cereb Cortex 2001;11:552–7. 4. White AM. Understanding adolescent brain development and its im- plications for the clinician. Adolesc Med State Art Rev 2009;20:73–90, viii–ix.
- 35. 5. Arria AM, Caldeira KM, Kasperski SJ, Vincent KB, Griffiths RR, O’Grady KE. Energy drink consumption and increased risk for alcohol dependence. Alcohol Clin Exp Res 2011;35:365–75. 6. Nawrot P, Jordan S, Eastwood J, Rotstein J, Hugenholtz A, Feeley M. Effects of caffeine on human health. Food Addit Contam 2003;20:1–30. 7. Savoca MR, MacKey ML, Evans CD, Wilson M, Ludwig DA, Harshfield GA. Association of ambulatory blood pressure and dietary caffeine in adolescents. Am J Hypertens 2005;18:116–20. 8. Lim S, Zoellner JM, Lee JM, Burt BA, Sandretto AM, Sohn W, Ismail AI, Lepkowski JM. Obesity and sugar-sweetened beverages in African- American preschool children: a longitudinal study. Obesity (Silver Spring) 2009;17:1262–8. 9. Hughes JR, Hale KL. Behavioral effects of caffeine and other meth- ylxanthines on children. Exp Clin Psychopharmacol 1998;6:87– 95. 10. Seifert SM, Schaechter JL, Hershorin ER, Lipshultz SE. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics 2011;127:511–28.
- 36. 11. Health Canada. Caffeine in food. Available from: http://www.hc-sc.gc. ca/fn-an/securit/addit/caf/food-caf-aliments-eng.php (cited 26 August 2013). 12. Committee on Nutrition and the Council on Sports Medicine and Fit- ness. Sports drinks and energy drinks for children and adolescents: are they appropriate? Pediatrics 2011;127:1182–9. 13. European Food Standard Agency Panel on Dietetic Products Nutrition and Allergies. Scientific Opinion on the substantiation of health claims related to caffeine and increase in physical performance during short- term high-intensity exercise, increase in endurance performance, increase in endurance capacity, and reduction in the rated perceived exertion/effort during exercise. Available from: http://www.efsa.europa.eu/en/efsajournal/ doc/2053.pdf (cited 26 August 2013). 14. Leviton A. Behavioral correlates of caffeine consumption by children. Clin Pediatr (Phila) 1992;31:742–50. 15. Bunting H, Baggett A, Grigor J. Adolescent and young adult percep- tions of caffeinated energy drinks. A qualitative approach. Appetite 2013;65:132–8.
- 37. 16. Frary CD, Johnson RK, Wang MQ. Food sources and intakes of caf- feine in the diets of persons in the United States. J Am Diet Assoc 2005;105:110–3. 17. Ahuja J, Perloff BP. Caffeine and theobromine intakes of children: results from CSFII 1994-96, 1998. Fam Econ Nutr Rev 2001;13:47–51. 18. Knight CA, Knight I, Mitchell DC, Zepp JE. Beverage caffeine intake in US consumers and subpopulations of interest: estimates from the Share of Intake Panel survey. Food Chem Toxicol 2004;42:1923–30. 19. Somogyi LP. Caffeine intake by the US Population. US Food and Drug Administration. Available from: www.fda.gov/downloads/AboutFDA/ CentersOffices/OfficeofFoods/CFSAN/CFSANFOIAElectronicR eadingRoom/ UCM333191.pdf (cited 26 August 2013). 20. Kit BK, Fakhouri TH, Park S, Nielsen SJ, Ogden CL. Trends in sugar- sweetened beverage consumption among youth and adults in the United States: 1999-2010. Am J Clin Nutr 2013;98:180–8. 21. Barone JJ, Roberts HR. Caffeine consumption. Food Chem Toxicol 1996;34:119–29. 22. Zipf G, Chiappa M, Porter KS, Ostchega Y, Lewis B, Dostal
- 38. J. The National Health and Nutrition Examination Survey: plan and opera- tions, 1999-2010. National Center for Health Statistics, Vital Health Stat Series 1 2013;56:1–37. 23. CDC, National Center for Health Statistics. NHANES response rates and population totals. Available from: http://www.cdc.gov/nchs/ nhanes/response_rates_CPS.htm (cited 15 July 2013). 24. Blanton CA, Moshfegh AJ, Baer DJ, Kretsch MJ. The USDA Auto- mated Multiple-Pass Method accurately estimates group total energy and nutrient intake. J Nutr 2006;136:2594–9. CAFFEINE INTAKE IN US CHILDREN 1131 D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 25. Thompson FE, Subar AF. Dietary assessment methodology. Edtion ed. In: Coulston AM, Boushey CJ, Ferruzzi MG, ed. Nutrition in the
- 39. prevention and treatment of disease. 3rd ed. Boston, MA: Academic Press, 2013. 26. Gibson R. Principles of nutritional assessment. 2nd ed. Oxford, United Kingdom: Oxford University Press, 2005. 27. US Department of Agriculture. Agricultural Research Service: Food Surveys Research Group. Available from: http://www.ars.usda.gov/ Services/docs.htm?docid=12085 (cited16 July 2013). 28. Curtin LR, Mohadjer LK, Dohrmann SM, Montaquila JM, Kruszan- Moran D, Mirel LB, Carroll MD, Hirsch R, Schober S, Johnson CL. The National Health and Nutrition Examination Survey: sample de- sign, 1999-2006. Vital Health Stat 2 2012;155:1–39. 29. United States Census Bureau. Poverty. Available from: http://www. census.gov/hhes/www/poverty/methods/definitions.html (accessed 26 August 2013). 30. US Department of Agriculture. Supplemental Nutrition Assistance Program (SNAP)- Eligibility. Food and Nutrition Service. Available from: http://www.fns.usda.gov/snap/eligibility (cited 18 July 2014). 31. CDC. National Center for Health. Available from:
- 40. http://www.cdc. gov/nchs/nhanes/nhanes2009-2010/DR1TOT_F.htm (accessed 15 July 2013). 32. Korn E, Graubard B. Analysis of health surveys. New York, NY: John Wiley & Sons Inc, 1999. 33. Wolter K. Introduction to variance estimation. New York, NY: Springer-Verlag, 1985. 34. Miller R. Developments in multiple comparisons. J Am Stat Assn 1977;72:779–88. 35. Winer B. Statistical principles in experimental design. New York, NY: McGraw-Hill Companies, 1971. 36. Seifert SM, Seifert SA, Schaechter JL, Bronstein AC, Benson BE, Hershorin ER, Arheart KL, Franco VI, Lipshultz SE. An analysis of energy-drink toxicity in the National Poison Data System. Clin Toxicol (Phila) 2013;51:566–74. 37. Castellanos FX, Rapoport JL. Effects of caffeine on development and behavior in infancy and childhood: a review of the published literature. Food Chem Toxicol 2002;40:1235–42.
- 41. 38. Rétey JV, Adam M, Khatami R, Luhmann UF, Jung HH, Berger W, Landolt HP. A genetic variation in the adenosine A2A receptor gene (ADORA2A) contributes to individual sensitivity to caffeine effects on sleep. Clin Pharmacol Ther 2007;81:692–8. 39. Arbeit ML, Nicklas TA, Frank GC, Webber LS, Miner MH, Berenson GS. Caffeine intakes of children from a biracial population: the Bo- galusa Heart Study. J Am Diet Assoc 1988;88:466–71. 40. Carskadon MA. Sleep in adolescents: the perfect storm. Pediatr Clin North Am 2011;58:637–47. 41. Hattersley L, Irwin M, King L, Allman-Farinelli M. Determinants and patterns of soft drink consumption in young adults: a qualitative analysis. Public Health Nutr 2009;12:1816–22. 42. Rath M. Energy drinks: what is all the hype? The dangers of energy drink consumption. J Am Acad Nurse Pract 2012;24:70–6. 43. Knight CA, Knight I, Mitchell DC. Beverage caffeine intakes in young children in Canada and the US. Can J Diet Pract Res 2006;67:96–9. 44. Bernstein GA, Carroll ME, Crosby RD, Perwien AR, Go FS, Benowitz NL. Caffeine effects on learning, performance, and anxiety in normal
- 42. school-age children. J Am Acad Child Adolesc Psychiatry 1994;33: 407–15. 45. Skinner JD, Carruth BR, Houck KS, Morris M, Moran J 3rd, Coletta F. Caffeine intake in young children differs by family socioeconomic status. J Am Diet Assoc 2000;100:229–31. 46. Ellison RC, Singer MR, Moore LL, Nguyen US, Garrahie EJ, Marmor JK. Current caffeine intake of young children: amount and sources. J Am Diet Assoc 1995;95:802–4. 1132 AHLUWALIA ET AL D ow nloaded from https://academ ic.oup.com /ajcn/article-abstract/100/4/1124/4576506 by guest on 05 M arch 2020 You will be responsible for answering this question with the required number of examples and historical periods. Please respond to the following question in 400-500 words. Your short essays should be well-organized, thoughtful analyses that engage the course material. Your responses must discuss
- 43. specific works of art/architecture and provide ample visual evidence from the textbook to support your argument. Use the lecture notes and textbook for support, but you do not need to consult outside sources. Your response will run through TurnItIn software, so be sure to cite the textbook, when necessary. Question: Over the course of the five hundred years we have studied this semester, the representation of subjectivity in portraiture has changed drastically. Please choose four examples and discuss the changing approach to subjectivity by considering not only aspects such as realism and style but also qualities such as the implied movement/activity of the sitter, the gaze, attributes, etc. At least one of your examples (but no more than two) must be from before the first half of the semester (prior to the midterm). You may analyze how the different concepts of subjectivity relate to the culture/society in question. Your four examples must come from four different stylistic periods. Each of the four examples must be identified by artist, title, date, medium, and cultural/historical period. 4 Examples: Jan van Eyck, Giovanni Arnolfini and His Wife, 1434. Oil on wood, 29 90 × 19 10 120. National Gallery, London. John Henry Fuseli, The Nightmare, 1781. Oil on canvas, 39 3340 × 49 1120. Detroit Institute of the Arts (Founders Society purchase with funds from Mr. and Mrs. Bert L. Smokler and Mr. and Mrs. Lawrence A. Fleishman). Henri Matisse, Woman with the Hat, 1905. Oil on canvas, 29 7 30 × 19 1110. San Francisco Museum of Modern Art, San Francisco
- 44. Kehinde Wiley, Napoleon Leading the Army over the Alps, 2005. Oil on canvas, 99 × 99. Brooklyn Museum, Brooklyn (Collection of Suzi and Andrew B. Cohen). SAMPLE ESSAY Question: Compare Michelangelo and Titian’s approach to color and nature. “Michelangelo and Titian are both outstanding artists who have made huge impacts on the subject of art, though their approaches to their work can be hugely different. Influenced hugely by High Renaissance artists Leonardo Da Vinci and Raphael, Titian encourages imaginations and participations from viewer. Michelangelo, on the other hand, references more to human anatomy and the central belief of Humanism: beauty of body. The way they expresses such difference is mainly through colors and contour: Michelangelo cast more emphasis on the harsh contour as well as the contrast between colors; while Titian neglects contour and focuses more on natural color. Firstly, the color styles of the two are significantly different. Take Last Judgement (1541) as an example. In this masterpiece, the artist depicts a scene where one line of people is elevating to the heaven while the other line falling into the hell. In an attempt to express the seriousness of the religions and holiness, as well as the perfection of human bodies, Michelangelo mixes his colors with black and white, as a mean to raise the contrast level between each objects that make up the space, so that the skins can look perfectly pale and the holiness can be highlighted. Clearly contradicting the color style of Michelangelo, Titian tend to use more soft, natural colors, of which the brightness and intensity are often not very high. His Meeting of Bacchus and Ariadne (1523) marks his signature natural way of using colors. In this work, he used variety of earth toned red and yellow to detail the figures, clothings, and animals. Even the color selections for negative space, sky and
- 45. ground, does not like abrupt at all, due to his avoidance of high contrast between elements. Secondly, the two artists have a different view on the use of contour lines as well. Michelangelo advocates harsh contours as he believes it singularizes the beauty of human and makes movements vivid. In Michelangelo’s Creation of Adam (1512), he made huge emphasis on the contour of every object within the painting. From god, Adam, to the smaller details like the fabrics behind them. If you look closely, the contour around the body of Adam is so harsh that it looks as if Adam is floating. On the other hand, preferring imagination over reality and stressing the nature over perfection, Titian avoids all forms of clear lines and harsh contours. In Titian’s pastoral symphony (1510), there is barely contour lines since he gives positive space a very natural colors that mesh well with the negative space. As a result, the contour is barely seen and the painting as a whole, looks more like natural world where no contour lines exist. To sum up, both Michelangelo and Titian are outstanding masters with respect to their eras. And their ways of using color and contour, though vastly different from each other, reflect their own background, style, and school. Most importantly, both styles are intriguing to the futurity.” 1006! CHAPTER 32 Contemporary Art Worldwide Kehinde Wiley. !e paintings and photographs of Basquiat, Marshall, and Simpson, which all fea- ture African Americans as subjects, stand in vivid contrast to the near-total absence of blacks in Western painting and sculpture until the past half century. One major contemporary artist who has set out to correct that discriminatory imbalance
- 46. is Los Angeles native K"#$%&" W$'"( (b. 1977). Wiley earned his BFA at the San Francisco Art Institute and his MFA at Yale University and is currently based in New York City, where he was artist-in-residence at the Studio Museum in Har- lem in 2001–2002. Wiley has achieved renown for his large-scale portraits of young urban African American men. His trademark paintings, however, are reworkings of historically important portraits in which he substitutes )gures of young black men in contemporary dress in order to situate them in what he calls “the )eld of power.” A characteristic example is Napoleon Lead- ing the Army over the Alps (*$+. 32-4) based on Jacques-Louis David’s painting (*$+. 27-2A) of the same subject. To evoke the era of the original, Wiley presented his portrait of an African Ameri- can Napoleon on horseback in a gilt wood frame. Although in many details an accurate reproduc- tion of David’s canvas, Wiley’s version is by no means a mechanical copy. His heroic narrative unfolds against a vibrantly colored ornate wallpa- per-like background instead of a dramatic sky—a distinctly modernist reminder to the viewer that this is a painting and not a window onto an Alpine landscape. Faith Ringgold. Like Bas- quiat and Wiley, M"',$% E&-./&0 (b. 1937) has examined the lives—or, more precisely, the death by lynching (*$+. 32-4A)—of
- 47. African American men in his art. Similarly, Simpson 32-5 F!"#$ R"%&&'(), Who’s Afraid of Aunt Jemima? 1983. Acrylic on canvas with fabric borders, quilted, 79 60 * 69 80. Private collection. In this quilt, a medium associated with women, Ringgold presented a tribute to her mother that also addresses African American culture and the struggles of women to overcome oppression. 32-4A EDWARDS, Tambo, 1993. 32-4 K+$"%)+ W"(+,, Napoleon Leading the Army over the Alps, 2005. Oil on canvas, 99 * 99. Brooklyn Museum, Brooklyn (Collection of Suzi and Andrew B. Cohen). Wiley’s trademark paintings are reworkings of famous portraits (FIG. 27-2A) in which he substitutes young African American men in contemporary dress in order to situate them in “the field of power.” 1 ft. 1 ft. 30702_ch32_rev03_1002-1041.indd 1006 30/07/18 12:03 pm © 2 01 8
- 51. ia l o r m at ch th e pu bl is he d pr od uc t. Copyright 2020 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. WCN 02-200-203 of the status quo gave rise to the notion of an artistic avant- garde.
- 52. !e term, which means “front guard,” derives from 19th-century French military usage. !e avant-garde were the troops sent ahead of the army’s main body to scout the enemy’s position and strength. Politicians who deemed themselves visionary and forward thinking subsequently adopted the term. It then migrated to the art world in the 1880s, when artists and critics used it to refer to the Realists, Impressionists, and Post-Impressionists—artists who were ahead of their time and who transgressed the limits of established art forms. Today, art historians generally use the term to describe more nar- rowly the modernist art movements of the opening decades of the 20th century. FAUVISM In 1905, at the third Salon d’Automne (Autumn Salon) in Paris, a group of young painters exhibited canvases so simpli"ed in design and so shockingly bright in color that a startled critic, Louis Vaux- celles (1870–1943), described the artists as Fauves (“wild beasts”). !e Fauves were totally independent of the French Academy and the “o#cial” Salon (see “Academic Salons and Independent Art Exhibitions,” page 853). !eir aim was to develop an art having the directness of Impressionism but employing intense color juxtaposi- tions for expressive ends. Building on the legacy of artists such
- 53. as Vincent van Gogh and Paul Gauguin, the Fauves went even further in liberating color from its descriptive function and exploring the e$ects that di$erent colors have on emotions. !e Fauves produced portraits, landscapes, still lifes, and nudes of spontaneity and verve, with rich surface textures, lively linear patterns, and, above all, bold colors. In an e$ort to release internal feelings, they employed star- tling contrasts of vermilion and emerald green and of cerulean blue and vivid orange held together by sweeping brushstrokes and bold patterns. !e Fauve painters never o#cially organized, and within "ve years, most of the artists had departed from a strict adherence to Fauve principles and developed their own more personal styles. During its brief existence, however, Fauvism made a signi"cant contribution to the direction of art by demonstrating color’s struc- tural, expressive, and aesthetic capabilities. Henri Matisse !e dominant Fauve artist was Henri Matisse (1869–1954), who believed that color could play a primary role in conveying meaning, and consequently focused his e$orts on developing this notion. In an early painting, Woman with the Hat (fig. 29-2), Matisse depicted his wife, Amélie, in a rather conventional manner
- 54. compositionally, but the seemingly arbitrary colors immediately startle the viewer, as does the sketchiness of the forms. !e entire image—the wom- an’s face, clothes, hat, and background—consists of patches and splotches of color juxtaposed in ways that sometimes pro- duce jarring contrasts. Matisse explained his approach in this painting and his contemporary Le Bonheur de Vivre (fig. 29-2A): “What characterized Fauvism was that we rejected imitative colors, and that with pure colors we obtained stronger reactions.”1 For Matisse and the Fauves, therefore, color became the formal element most responsible for pictorial coherence and the primary conveyor of meaning (see “Henri Matisse on Color,” page 890). Harmony in Red. !ese color discoveries reached maturity in Matisse’s Red Room (Harmony in Red; fig. 29-3). !e subject is the interior of a comfortable, prosperous household with a maid plac- ing fruit and wine on the table, but Matisse’s canvas is radically dif- ferent from traditional paintings of domestic interiors (for example, figs. 25-19 and 25-19A). !e Fauve painter depicted objects in simpli"ed and schematized fashion and .attened out the forms. For example, Matisse eliminated the front edge of the table, rendering the table, with its identical patterning, as .at as the wall behind
- 55. it. !e window at the upper le/ could also be a painting on the wall, further .attening the space. Everywhere, the colors contrast richly and intensely. Matisse’s process of overpainting reveals the impor- tance of color for striking the right chord in the viewer. Initially, this work was predominantly green. !en Matisse repainted it blue, but blue also did not seem appropriate to him. Not until he repainted the canvas red did Matisse feel that he had found the right color for the “harmony” he wished to compose. 29-2A MATISSE, Le Bonheur de Vivre, 1905–1906. 29-2 Henri Matisse, Woman with the Hat, 1905. Oil on canvas, 29 7 340 × 19 11120. San Francisco Museum of Modern Art, San Francisco (bequest of Elise S. Haas). Matisse’s portrayal of his wife, Amélie, features patches and splotches of seemingly arbitrary colors. He and the other Fauve painters used color not to imitate nature but to produce a reaction in the viewer. 1 ft. Every thumbnail image has a corresponding full-size MindTap Bonus Image and content in the MindTap reader for this chapter.! 889
- 56. 30702_ch29_rev03_886-931.indd 889 12/06/18 11:00 am © 2 01 8 C en ga ge L ea rn in g. A ll R ig ht s R es er ve
- 57. d. T hi s co nt en t i s no t y et fi na l a nd C en ga ge L ea rn in
- 59. nt m at er ia l o r m at ch th e pu bl is he d pr od uc t. Copyright 2020 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. WCN 02-200-203
- 60. 808! CHAPTER 27 Romanticism, Realism, Photography: Europe and America, 1800 to 1870 ROMANTICISM Whereas Neoclassicism’s rationality reinforced Enlightenment thought, particularly Voltaire’s views (see “Voltaire,” page 779), Romanticism owed much to the ideas of Jean-Jacques Rousseau (see “Rousseau,” page 781). Rousseau’s exclamation “Man is born free, but is everywhere in chains!”—the opening line of his Social Contract (1762)—summarizes a fundamental Romantic premise. Romanticism emerged from a desire for freedom—not only politi- cal freedom but also freedom of thought, feeling, action, worship, speech, and taste. Romantics asserted that freedom was the right and property of all. !ey believed that the path to freedom was through imagination and feeling rather than reason. !e allure of the Romantic spirit grew dramatically during the late 18th century, when the term originated among German liter- ary critics. !eir aim was to distinguish peculiarly “modern” traits from the Neoclassical traits that already had displaced Baroque and Rococo design elements. Consequently, some scholars refer to Romanticism as a phenomenon that began around 1750 and ended about 1850, but most use the term more narrowly to denote an art movement that "ourished from about 1800 to 1840, between Neo-
- 61. classicism and Realism. Roots of Romanticism !e transition from Neoclassicism to Romanticism in art was more than a stylistic shi#. It represented a philosophical change in emphasis from calculation to intuition, from reason to emotion. Among the leading manifestations of Romanticism was height- ened interest in the medieval period and in the sublime. For people living in the 18th century, the Middle Ages were the “dark ages,” a time of barbarism, superstition, mystery, and miracle. !e Romantic imagina- tion stretched its perception of the Middle Ages into all the worlds of fantasy open to it, includ- ing the ghoulish, infernal, terrible, nightmarish, grotesque, and sadistic—the imagery that comes from the chamber of horrors when reason sleeps. Related to the imaginative sensibility was the period’s notion of the sublime. Among the indi- viduals most involved in studying the sublime was the British politician and philosopher Edmund Burke (1729–1797). In A Philosophical Enquiry into the Origins of Our Ideas of the Sublime and Beautiful (1757), Burke articulated his de$nition of the sublime: feelings of awe mixed with terror. Burke observed that pain or fear evoked the most intense human emotions and that these emotions could also be thrilling. !us raging rivers and great storms at sea could be sublime to their view- ers. Accompanying this taste for the sublime was the taste for the fantastic, occult, and macabre. John Henry Fuseli. !e Swiss painter Johann Heinrich Füssli, better known by his English
- 62. name—J%&' H(')* F+,(-. (1741–1825)—lived in Rome from 1770 to 1778, settled in England in 1799, and eventually became a member of the Royal Academy of Art and one of its instruc- tors. Largely self-taught, he contrived a distinc- tive manner to express the fantasies of his vivid 27-8 J!"# H$#%& F'($)*, !e Nightmare, 1781. Oil on canvas, 39 3 340 + 49 1 1 20. Detroit Institute of the Arts (Founders Society purchase with funds from Mr. and Mrs. Bert L. Smokler and Mr. and Mrs. Lawrence A. Fleishman). The transition from Neoclassicism to Romanticism marked a shift in emphasis from reason to feeling. Fuseli was among the first painters to depict the dark terrain of the human subconscious. imagination. Fuseli specialized in night moods of horror and in dark fantasies—in the demonic, the macabre, and o#en the sadistic. In !e Nightmare (/.0. 27-8), a beautiful young woman lies asleep, draped across the bed with her limp arm dangling over the side. An incubus, a demon believed in medieval times to prey, o#en sexually, on sleeping women, squats ominously on her body. In the background, a ghostly horse with "aming eyes bursts into the scene from beyond the curtain. Despite the temptation to see the painting’s title as a pun because of this horse, the word
- 63. nightmare in fact derives from “night” and “Mara.” Mara was an evil spirit in Scandinavian mythology who tormented and su1ocated sleepers. Fuseli was among the $rst to attempt to depict the dark terrain of the human subconscious that became fertile ground for later artists. William Blake. In their images of the sublime and the terrible, Romantic artists o#en combined something of Baroque dyna- mism with naturalistic details in their quest for grippingly moving visions. !ese elements became the mainstay of Romantic art and contrasted with the more intellectual, rational Neoclassical themes and compositions. !e two were not mutually exclusive, however. Gros, Girodet-Trioson, and Ingres e1ectively integrated elements of Neoclassicism with Romanticism. So, too, did the visionary English poet, painter, and engraver W.--.23 B-24( (1757–1827). Blake greatly admired ancient Greek art because it exempli- $ed for him the mathematical and thus the eternal, and his work o#en incorporated classical references. Yet Blake did not align himself with prominent Enlightenment $gures. Like many other Romantic artists, he also found the art of the Middle Ages appeal- ing. Blake derived the inspiration for many of his paintings and poems from his dreams. !e importance he attached to these 1 ft. 30702_ch27_rev03_800-847.indd 808 11/06/18 4:40 pm
- 67. nt m at er ia l o r m at ch th e pu bl is he d pr od uc t. Copyright 2020 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. WCN 02-200-203
- 68. Flanders 577 crown at his feet and resplendent in a deep- scarlet mantle—presides in majesty. To God’s right is the Virgin, represented, as in the Gothic age and in a small Jan van Eyck diptych (two- paneled painting; !"#. 20-10A), as the queen of Heaven, with a crown of 12 stars on her head. John the Baptist sits to God’s le$. To either side is a choir of angels, with an angel playing an organ on the right. Adam and Eve appear in the far panels. %e inscriptions in the arches above Mary and Saint John extol the Virgin’s virtue and purity and Saint John’s greatness as the forerunner of Christ (see “Early Christian Saints,” pages 246–247). %e inscription above the Lord’s head translates as “%is is God, all-powerful in his divine majesty; of all the best, by the gentle- ness of his goodness; the most liberal giver, because of his in&nite generosity.” %e step behind the crown at the Lord’s feet bears the inscription “On his head, life without death. On his brow, youth without age. On his right, joy without sadness. On his le$, security without fear.” %e entire altarpiece ampli&es the central theme of salvation. Even though humans, personi&ed by Adam and Eve, are sinful, they will be saved because God, in his in&nite love, will sac-
- 69. ri&ce his own son for their sake. %e panels of the lower register extend the symbolism of the upper. In the center panel, saints arrive from the four corners of the earth through an opulent, 'ower-spangled landscape. %ey pro- ceed toward the altar of the Lamb and the octagonal fountain of life (compare !"#. 20-2). %e book of Revelation passage that recounts the adoration of the Lamb is the main reading on All Saints’ Day (November 1). %e Lamb symbolizes the sacri&ced son of God, whose heart bleeds into a chalice, while into the fountain spills the “pure river of water of life, clear as crystal, proceeding out of the throne of God and of the Lamb” (Rev. 22:1). On the right, the 20-10A VAN EYCK, Madonna in a Church, ca. 1430–1440. A SECOND OPINION Giovanni Arnolfini and His Wife In 1434, Jan van Eyck depicted Giovanni Arnolfini, a Lucca financier who had established himself in Bruges as an agent of the Medici family, and his second wife in their home (FIG. 20-11). Arnolfini holds the hand of his spouse, whose name is not known. That much is certain, but the purpose and meaning of the double portrait remain the subject
- 70. of con- siderable debate, with a few new interpretations having been advanced just during the last several years. According to the traditional interpreta- tion of the painting, Jan recorded the couple taking their marriage vows. As in the Mérode Triptych (FIG. 20-8), almost every object portrayed car- ries meaning. For example, the little dog symbolizes fidelity (the com- mon canine name Fido originated from the Latin fidere, “to trust”). The finial (crowning ornament) of the marriage bed at the right is a tiny statue of Saint Margaret, patron saint of childbirth. (The bride is not yet preg- nant, although the fashionable costume she wears makes her appear so.) From the finial hangs a whiskbroom, symbolic of domestic care. Indeed, even the placement of the two figures in the room is meaningful. The woman stands near the bed and well into the room, whereas the man stands near the open window, symbolic of the outside world. Many art historians, however, dispute this interpretation because, among other things, the room in which Arnolfini and his wife stand is a public reception area, not a bedchamber. One scholar has suggested that Arnolfini is conferring legal privileges on his wife to conduct busi-
- 71. ness in his absence. Another thinks that this may be a memorial portrait of a wife who died in childbirth. In any case, an important aspect of the painting is that the artist functions as a witness to whatever event is taking place. In the back- ground, framed by the arms and joined hands of the two figures, is a convex mirror (complete with its spatial distortion, brilliantly recorded; compare FIG. 22-40), in which Jan depicted not only the principals, Arnolfini and his wife, but also two persons who look into the room through the door. (Arnolfini’s raised right hand may be a gesture of greeting to the two men.) One of these must be the artist himself, as the elegant inscription above the mirror, Johannes de Eyck fuit hic (“Jan van Eyck was here”), announces that he was present. The self- portrait also underscores the painter’s self-consciousness as a professional art- ist whose role deserves to be recorded and remembered. 20-11 J!" #!" E$%&, Giovanni Arnol!ni and His Wife, 1434. Oil on wood, 29 90 ' 19 10 120. National Gallery, London. Jan van Eyck played a major role in establishing portraiture as an important Flemish art form. In this portrait of an Italian financier and his wife, he also portrayed himself in the convex mirror on the rear wall.
- 72. 1 ft. 30702_ch20_rev03_566-591.indd 577 08/06/18 5:50 pm © 2 01 8 C en ga ge L ea rn in g. A ll R ig ht s R es er
- 76. Copyright 2020 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. WCN 02-200-203